



Abstract
Purpose: Autism spectrum disorder (ASD) is a developmental disorder affecting an individual’s ability to communicate, interact, behave, and learn. The purpose of this study was to determine knowledge, attitudes, and confidence of dental hygiene students in providing care to children with ASD as a mechanism for evaluating dental hygiene curricula for patients with special needs.
Methods: A simulated-virtual training (SVT) intervention was developed as an interactive approach for educating dental hygiene students on providing care to a child patient with ASD. The SVT intervention consisted of a scenario in which the clinician “interacted” with a child with ASD who was having difficulty in the dental environment. Pre- and post-test surveys measured students’ knowledge, attitudes, and perceived confidence related to providing dental hygiene services to children with ASD prior to and following the intervention. The Wilcoxon Signed Rank was used to determine statistical significance at the p=.05 level.
Results: Thirty-three second year dental hygiene students completed the pre- and post-test surveys for a response rate of 97%. Statistically significant differences were observed for self-reported confidence to provide care to patients with ASD upon graduation, assessment of the unique needs of children with ASD, and an understanding of the dental needs for children with ASD (p<0.05). Participants’ confidence with performing dental hygiene services on children with ASD greatly increased, with statistically significant difference found for almost all services (i.e., oral exam, oral hygiene instruction, oral photos, radiographs, scaling, fluoride treatment; p<0.05) except selective polishing. Most (90%) agreed that there is a need for additional/elective resources to help increase comfort in providing care to children with ASD.
Conclusion: Results indicate the SVT intervention increased students’ knowledge, attitudes, self-perceived confidence, and comfort. Dental and dental hygiene curricula could include technologies and intervention methods to advance access to dental care by children with ASD.
- access to care
- special needs patients
- autism spectrum disorder
- clinical education
- dental hygiene education
Introduction
The National Autism Association (NAA) states that autism spectrum disorder (ASD) is the fastest growing developmental disorder affecting an individual’s ability to communicate, interact, behave, and learn.1 Over the past few decades in the United States (US) alone, there has been a significant increase in the number of children diagnosed with ASD. According to the Centers for Disease Control and Prevention (CDC), ASD is a life-long disorder that is often diagnosed before the age of 3 years.2 Characteristics associated with ASD include social delays, varying levels of communication, and unusual interests or beahviors.2 In addition, there are several characteristics that a child with ASD might exhibit such as eye contact avoidance, loneliness, speech and language skills delay, unusual sensory reactions (i.e., sound, taste, look, feel), unresponsiveness to their name by 12 months of age, and inability to adapt to minor changes. Other symptoms can include hyperactivity, impulsivity, short attention span, aggression, self-injury, temper tantrums, unusual eating and sleeping habits, unusual mood or emotional reactions, lack of fear or more fear than expected, and unusual reactions to the way things sound, smell, taste, look, or feel.2
Current prevalence rates estimate that 1 in 44 children are diagnosed with ASD, with males affected at least four times more frequently than females.3 With the publication of the American Psychiatric Association’s fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) in 2013, substantial changes were made to the diagnosis of ASD; the four separate disorders that included autistic disorder (autism), Asperger’s disorder, pervasive developmental disorder not otherwise specified, and childhood disintegrative disorder were combined into a single condition with varying levels of symptom severity.4 Due to the significant increase in childhood diagnoses and changes made to the DSM-5, it is increasingly important for health professionals to be aware of ASD and the characteristics associated with this disorder.
As the ASD population grows, oral health implications should be considered.5-8 Children with ASD require detailed oral hygiene home care and routine dental hygiene visits. Studies have shown significant differences between child patients with ASD and cohorts without ASD regarding oral hygiene.5,6,8,9,10 Child patients with ASD typically have a higher prevalence for dental caries, a higher incidence of gingivitis and periodontal disease, delayed tooth eruption, and have increased harmful oral habits such as mouth breathing, tongue thrusting, xerostomia, and bruxism.5-8,10 All of these characteristics negatively impact a child’s oral health resulting in the need for dental support and intervention techniques.5-10 Many children with ASD have increased anxiety when visiting the dental office, which leads to difficulty communicating their feelings, sensory sensitivities, and a fear of the unknown.6 Since many children with ASD cannot effectively communicate, behaviors occurring during dental procedures may be perceived as noncompliant or uncooperative behaviors, which may be problematic for dental professionals, especially for those without advanced knowledge and skills to manage these behaviors.5,7,9,11
Dental hygienists specialize in preventative techniques and treatments, making it critical for them to have the knowledge and understanding to treat children with ASD. While dental hygienists may be exposed to educational content in their didactic curriculum on providing care to patients with ASD, research has shown that there is a general lack of experiential training.16-18 The most recent Commission on Dental Accreditation (CODA), Standards for Dental Hygiene Education states, “Graduates must be competent in providing dental hygiene care for the child, adolescent, adult, geriatric, and special needs patient populations” (Standard 2-12).19 To meet this standard, dental hygiene programs may have varying definitions of competency and clinical experiences related to patients with special needs and may not be inclusive of patients with an ASD diagnosis.
Research shows there is a high percentage of dental professionals who report inadequate preparation during their formal training to meet the clinical needs of children with ASD,11-15 which may lead to feelings of uncertainty and doubt in treating these pediatric patients with special needs. There are a limited number of studies that have examined the confidence of dental professionals with managing child patients with ASD,11-15 and gap in the literature regarding the confidence of dental hygienists in this area. Minimum experience with pediatric patients with ASD may also lead to a decrease in clinicians’ comfort level to provide treatment, ultimately resulting in limited access to care.11-15 Therefore, developing innovative experiential learning via simulated or virtual trainings for dental hygiene students that focuses on providing care to children with ASD is warranted. The purpose of this pilot study was to assess the use of a simulated-virtual training (SVT) educational module to improve dental hygiene students’ self-reported knowledge, attitudes, and perceived confidence in providing care to children with ASD.
Methods
A single group, pre- post-test design was used to examine dental hygiene students’ self-reported knowledge, attitudes, perceived confidence, and comfort toward dental hygiene care management for children with ASD prior to and following participating in a simulated-virtual training (SVT) intervention. A convenience sample of second-year, entry-level dental hygiene students from a four-year public institution located in an urban city in the Southeastern US was invited to participate. Old Dominion University’s Institutional Review Board approved the study (#20-139).
Data collection
An investigator designed survey, “Dental Hygiene Students’ Knowledge, Attitudes, and Perceived Confidence Treating Children with ASD” was adapted from Mohebbi et al.12 The original instrument measured dental students’ knowledge, attitudes/confidence, and barriers in providing oral health care to patients with disabilities.12 The survey was modified to managing children with ASD while performing dental hygiene services. An expert panel of dental hygienists reviewed the modified survey for face and content validity. In addition, the survey was piloted twice among a small sample of dental hygiene students who had graduated one year prior to the initiation of the study. Modifications were made based on feedback received. The final pre-and post-survey instrument contained 32-items consisting of true/false, multiple choice, and statements on a 5-point Likert-scale. Data was collected on the following outcomes: knowledge (n=5), attitudes (n=9), confidence (n=7), comfort (n=4), and demographic variables (i.e., age, gender, race/ethnicity, prior educational training related to ASD), and was self-administered through an online survey platform (Qualtrics, Provo, UT, USA).
Intervention
The SVT intervention was developed as a one-time multimedia web-based (Articulate Storyline® 360; Articulate, New York, NY, USA) interactive asynchronous module, which simulated behaviors of a child with ASD experiencing anxiety/distress the dental care setting. Dental hygiene student participants were required to utilize theoretical, conceptual, and critical thinking skills to correctly respond to a series of 11 scenarios. Content for each scenario was evidence-based and focused on the dental hygiene process of care. If the dental hygiene student answered the scenario question incorrectly, the module would allow a second attempt. and explanations of the correct answers were provided. Participants had unlimited attempts to complete the module. The SVT intervention was developed and designed by the research team and Old Dominion University’s Center for Learning and Teaching personnel, which consisted of instructional technology specialists, a graphic designer, multimedia manager, and a lead instructional designer.
Procedures
Invitations to participate in the study were sent via email. Students who expressed interest in participating were required to return a signed informed consent document. Once informed consent was obtained, students were enrolled in the SVT intervention, located on an organizational page within the learning management system. After the recruitment period closed, participants received an email notification to complete the pre-test survey within 7 days; thereafter, the SVT intervention module opened for participants. Participants received an email notification to complete the post-test survey two weeks following the completing of the SVT module. Total data collection occurred over 8 weeks, with bi-weekly email reminders. Upon completion of the study, participants received a $10 Amazon e-gift card as thank-you for their participation.
Data Analysis
Descriptive statistics such as means, standard deviations, and frequencies were based on the level of measurement for each variable. There were five statements with the response options of true/false and multiple choice for the knowledge measure. Participants received a score of one or zero for correct and incorrect responses; the percentage of participants who correctly answered each statement before and after the SVT intervention was reported. For the measures of attitude and comfort, a 5-point Likert scale (1=strongly disagree to 5=strongly agree and 1=very little importance to 5=very important) was used. Confidence was measured using a 5-point Likert scale (1=very little confidence to 5=very confident). The Wilcoxon Signed Rank test determined statistically significant mean differences for some outcome variables. The McNemar test was used to determine statistically significant differences between binomial variables that were a repeated measure (e.g., the knowledge variable). Data was analyzed using a software program (SPSS V.26; IBM, Armonk, NY, USA) and alpha was set at 0.05.
The two open-ended questions were qualitatively analyzed using a general inductive approach. The first researcher reviewed all text from each question and developed themes. Using the themes for each open-ended question, a second researcher independently paired the text to the themes. Both researchers then reviewed and discussed the themes, sub-themes, and corresponding statements to determine final agreement. A third reviewer examined the final tables to establish trustworthiness of the content with the themes and sub-themes.
Results
Of the thirty-four dental hygiene students invited to participate in this pilot study, thirty-three dental hygiene students completed the pre-test survey, intervention, and post-test survey for a participation rate of 97%. All participants were female, aged 18-24 years (63.6%), and most of the participants were White. Most (87.8%) reported receiving formal didactic instruction (lecture/face-to-face, online, or a combination) on providing dental hygiene care to individuals with ASD. When asked which dental hygiene courses the formal instruction was provided, most respondents reported dental hygiene theory courses. Prior to the intervention, 100% of participants reported not providing care to a patient with ASD. Sample demographics are shown in Table I.
Sample demographics (n=33)
Five statements (three true/false and two multiple choice items) were used to assess the participants’ knowledge prior to and following the SVT module. In general, knowledge improved on three out of five statements. The greatest increase for correct responses was observed for the statement, “Children with ASD prefer soft and sweet foods” (42.4%, n=14 vs. 66.7%, n=22), however it was not statistically significance (Table II).
Pre- and post-intervention correct knowledge responses (n=33)
Eight statements using a five-point Likert scale ranging from strongly disagree (1) to strongly agree (5) and one statement using a five-point Likert scale ranging from very little importance (1) to very important (5) were used to assess attitudes towards children with ASD. Statistically significant differences were observed for 3 out of 7 statements, which included: “I feel confident that I can provide care to child patients with ASD upon graduation” (3.42 ± 0.94 vs. 3.97 ± 0.73, p=0.01), “I understand how to assess the unique needs of children with ASD” (3.33 ± 0.85 vs. 4.15 ± 0.51, p<0.001), and “I feel that I understand the dental needs of children with ASD” (3.52 ± 0.91 vs. 4.06 ± 0.66, p=0.02) (Table III). The mean perceived confidence improved among participants with statistical significance for all dental hygiene services (i.e., oral exam, OHI, oral photos, radiographs, scaling, fluoride treatment) except one (selective polishing) after completing the SVT module (p≤0.05) (Table IV).
Pre- and post-intervention attitude changes* (n=33)
Pre- and post-intervention confidence to perform dental hygiene services* (n=33)
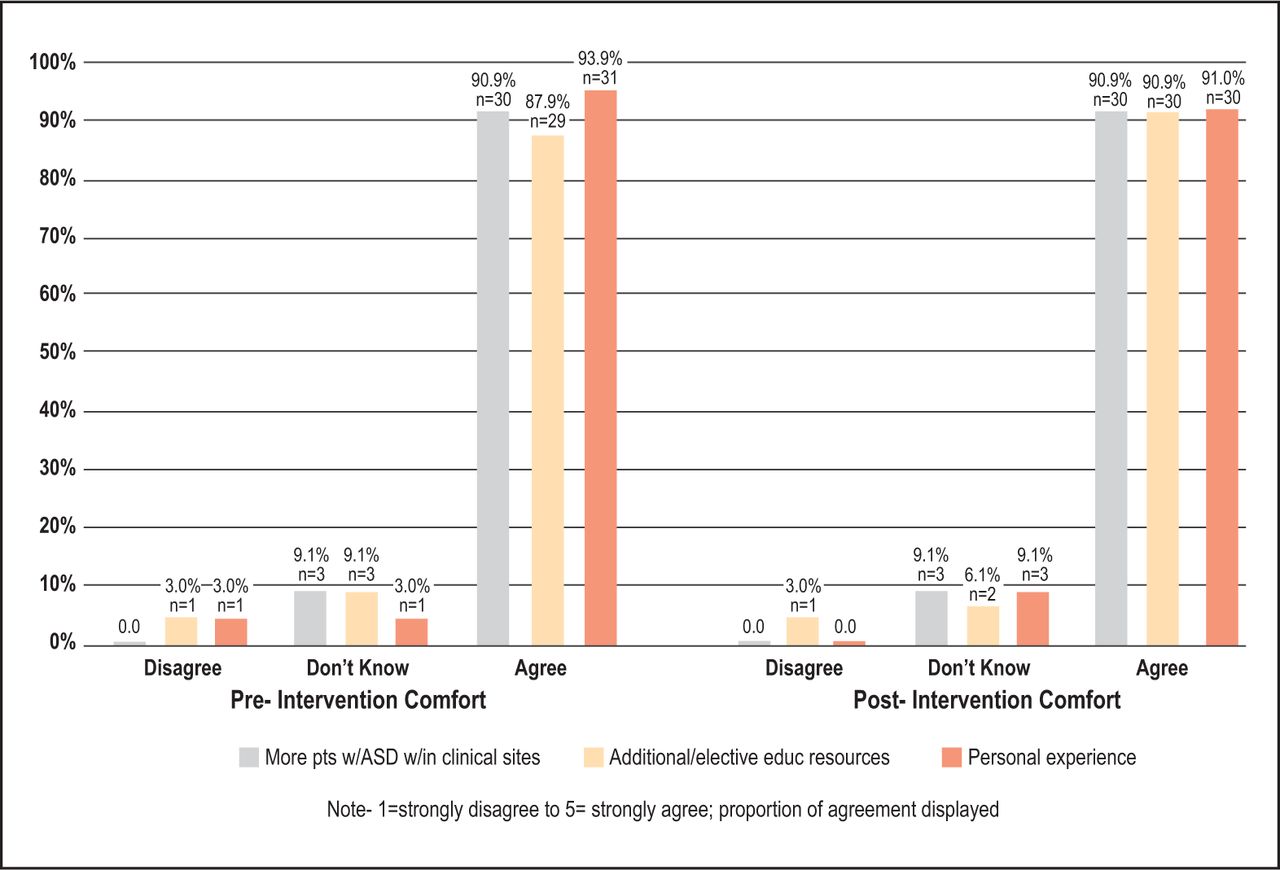
A five-point Likert scale ranging from strongly disagree (1) to strongly agree (5) was used to assess three different strategies that could potentially increase the participants’ comfort levels in providing care to children with ASD. The three strategies assessed were providing care to more patients with ASD within clinical sites, additional or elective resources given to students, and having had personal experiences with an individual with ASD (i.e., family member or friend diagnosed with ASD). In general, most participants agreed or strongly agreed that all three strategies would increase comfort levels before and after completing the SVT module. The greatest change was observed for the strategy of additional or elective resources (87.9%, n=29 vs. 90.9%, n=30) (Figure 1).

Pre vs. Post Intervention Agreement to Comfort Statements
Prior to completing the SVT intervention, participants were invited to provide additional information concerning their learning or clinical experience related to pediatric patients with ASD. A total of seven students provided comments and the themes of patient management, clinical experience, and didactic curriculum emerged. Several participants shared concern and intimidation for patient management with someone who has ASD. In terms of clinical experience, only one participant reported working with children with ASD; the other participants denied any past experiences at the time of the study completion. Lastly, one participant reported wanting more time within the curriculum to ensure adequate preparedness to care for children with ASD.
Participants were invited to provide additional information at the conclusion of the post-test survey. The themes of informative and preparedness emerged from the students’ feedback (n=8). Students reported that the module was valuable and a great educational resource. Some of the responses included: “This module would be a great educational resource in the future to teach students how to better treat ASD patients.” More importantly, students perceived that the module helped broaden their knowledge, understanding, and pre-paredness in providing care to pediatric patients with ASD. One participant reported, “I don’t know how many patients I will encounter that will have ASD, but I do know for sure that I will be able to treat them in a way that makes them feel as comfortable as possible. I will know how to address the situation if they get anxious or don’t want to cooperate, while getting them to trust me.” Another participant reported, “I understand more about patients with ASD because of this course.”
Discussion
Findings from the current study revealed that participants’ knowledge, attitudes, confidence, and comfort improved to some degree after exposure to the SVT intervention. In addition, while participants reported having some didactic content related to patients with ASD, the SVT intervention provided another opportunity for students to learn more about this patient population while also applying their skills related to the dental hygiene process of care. Previous research has found that dental professionals in general do not feel confident and comfortable in providing care to individuals, specifically children, with ASD.12-14,16-18,20-22 One reason for this lack of confidence in the clinical environment is a lack of educational preparation and hands on clinical experiences,16-18 which was also supported by the findings in the present study.
In this study, participants reported no prior clinical experiences with patients with ASD, and some participants reported being unsure of their patient management skills to provide care to these patients. Similarly, participants in the study by Dao et al. agreed there was a lack of experience, training, and education in treating individuals with special needs in dental school settings, making them feel inadequately prepared to provide the appropriate clinical care.14 Similar to Dao’s findings, Wolff et al. found that 75% of dental students reported little or no education or clinical training in managing patients with special needs.21 Romer et al. discovered that dental students indicated limited educational experiences in regard to care of individuals with disabilities.23 Casamassimo et al. found similar results, with only one-fourth of general dentists reporting hands-on experiences with children with special health care needs.24 Previous study findings correlate with the present study regarding inadequate clinical experiences while in an educational setting.14,21,23 The qualitative responses prior to the intervention were also all consistent with previous literature, showing that students do not feel confident, comfortable, or adequately prepared to provide care to children with ASD.12-14,16-18,20-22 In a study by Dougall et al. dental students agreed that in order to increase their confidence in providing care to individuals with disabilities, school curriculum should shift away from the traditional educational methods of focusing on the patient’s medical diagnosis and focus more on patient-centered treatment approaches.16
Knowledge of ASD
Findings from the present study found that there was an increase in the percentage of correct responses for three of the five statements. Surprisingly, two of the statements had a decrease in the percentage correct responses from pre- to post-tests. One possible reason for this finding may be related to the content of the SVT intervention, which primarily focused on what a clinician should do during the dental hygiene process of care appointment for a child with ASD. Moreover, prior to progressing through the scenarios within the SVT module, dental hygiene students watched a brief introduction video that provided high-level background information (i.e., prevalence of ASD diagnosis), which may explain the observed decrease for the correct responses on two of the statements at post-test. The decrease in the correct response pre-post for the statement, “Children with ASD are at a higher risk for oral disease,” is consistent with previous literature. Previous studies also found conflicting, inconsistent results in provider responses when evaluating the oral characteristics and prevalence of dental caries in individuals with ASD compared to individuals without special needs or disabilities.8-10,25-36
Attitudes Toward Children with ASD
Attitudes towards confidence in providing care to patients with ASD upon graduation and understanding how to assess the unique needs of children with ASD, as well as their dental needs, increased among participants following the SVT module. Results from this study are consistent with Mohebbi et al. in which dental students’ knowledge and attitudes towards the oral health care of patients with disabilities improved after receiving an intervention.12 Jones and Miller also examined effectiveness of using an educational module to understand dental hygiene students’ attitudes towards persons with disabilities.37 Results from this study found the educational module increased participants’ attitudes score and allowed for participants to gain a better understanding for a patient-centered approach and advocacy when working with individuals with disabilities.37 Overall, the results of this study correlated with past literature in that educational modules can increase and improve attitudes towards individuals with ASD and patients with special needs in general.
Self-Perceived Confidence
After completing the SVT intervention, participants’ self-perceived confidence improved for all dental hygiene services, with statistically significant differences identified almost all dental hygiene services except selective polishing. The results demonstrated that the constructed SVT module may have improved students’ confidence to progress through specific parts of the dental hygiene process of care, by way of a step-by-step process with immediate feedback for each question posed to the student within each scenario. Similar to the intervention module in this study, Kleinert et al. used a virtual patient module to present a 10-year-old child with Down Syndrome with a painful tooth.15 The researchers found the module increased dental students’ competence and decreased their perception of difficulty in caring for children with developmental disabilities. Results from the Kleinert et al. study demonstrated that a virtual module was an effective educational tool, while preparing students to be sensitive and competent professionals.15 Kleinert et al. also found an educational module provided an experience that simulated the dental setting while implementing problem-solving and dentist-patient communication skills, an important experience that this present study additionally found true. The literature discusses various techniques and tools to help increase engagement with children with ASD in the dental setting. The “tell-show-do” technique has been described as an effective reinforcement to communicate information to patients with ASD.13,38-40 Many of the scenarios presented in the module of the present study followed the “tell-show-do” technique as a means to make the simulated experience comfortable for both the child and the clinician. Other literature mentions techniques including visual pedagogy, video technology, mobile applications, and communication devices.39,41,42 Future research could implement these techniques to increase engagement with children with ASD into a virtual educational module to further evaluate how these tools can increase clinician confidence and comfort.
Provider comfort levels
Most participants agreed that additional or elective educational resources are important strategies for increasing comfort in treating child patients with ASD. Krause et al. found that 64% of US and Canadian dental schools reported offering a special needs course separate from the curriculum.18 Results from Casamassimo et al. indicated more than 40% of general dentists found additional training pertinent to treating children with special health care needs as desirable or very desirable.24 Dehaitem et al. found curriculum overload and limited time were the most frequently reported reasons for minimal content related to caring for individuals with special needs.17 However, neglecting the topic of special needs in both dental and dental hygiene school curricula has potentially led to limited access of for these patients.17 The SVT module was designed to be completed from start to finish over a shorter period of time, while the intervention used in Mohebbi et al., included a 10-day intervention. Still, results from the present study and Mohebbi et al. were similar, suggesting that short-term training is beneficial and can improve students’ attitudes in providing care to children with ASD. The SVT intervention solidified the concept that the provision of additional resources is valuable and improves students’ overall awareness for ways to provide dental care to children with ASD.
This study had limitations. The use of a convenience sample and self-selection influenced the homogenous sample and size, limiting the generalizability of the findings. Self-reporting and recall bias must be considered when using a survey for data collection. Despite these limitations, to the researchers’ knowledge, this was the first study to pilot an intervention with a focus on pediatric patients with ASD specifically for dental hygiene students. Future modifications of the SVT intervention will include more depth and breadth didactic about ASD prior to students completing the scenarios. Other expansion plans include developing the SVT into a virtual platform that will allow for collaboration with other dental hygiene programs to engage in the activity, and the development of a continuing education course for practicing dental hygienists.
Conclusions
The SVT intervention increased dental hygiene students’ knowledge, attitudes, perceived confidence, and comfort to provide care to children with ASD. The SVT intervention was a self-directed module that created experiential learning for dental hygiene students, which allowed them to utilize critical-thinking skills as they applied the dental hygiene process of care to constructed scenarios. The study findings underscore the need for more research about this topic, with the recommendation to extend this study to a broader population of dental hygiene students as well as practicing dental hygienists.
Acknowledgements
This research was funded by the American Dental Hygienists’ Association Institute for Oral Health Research Grant (#RG 20-01).
Footnotes
This manuscript supports the NDHRA priority area Professional development: Education (educational modules).
- Received December 13, 2021.
- Accepted May 3, 2022.
- Copyright © 2022 The American Dental Hygienists’ Association





{kind=link}