



Abstract
Purpose: Workplace burnout in academia is a problem that affects career satisfaction and longevity. The purpose of this study was to determine the prevalence of burnout among entry-level dental hygiene program directors.
Methods: The Copenhagen Burnout Inventory (CBI) survey was used to determine prevalence of burnout in 325 dental hygiene program directors from across the United States. The survey was disseminated electronically. The CBI contains 19 questions that measure overall, personal, work-related, and client/student-related burnout on a five-point Likert type scale. The survey also included nine demographic and three open-ended questions related to burnout. Descriptive statistics, one sample t-tests, and one-way ANOVA tests were used to analyze the data.
Results: One hundred twenty-seven dental hygiene program directors completed the survey for a 39.1% response rate. Most participants (62.2%, n=79) indicated moderate to high burnout on the personal burnout subscale, approximately one half (51.2%, n=65) on the work-related burnout subscale, and one third (33.1%, n=42) on the client/student-related burnout subscale. No statistically significant differences were found when comparing mean scores between directors of two-year and four-year program or between participants under age 50 and those 50 years of age and older (p-values>0.05). Program directors with teaching workloads of 51-60% had significantly lower burnout on the work-related burnout subscale when compared to participants with teaching workloads of 31-40% (p=0.045). Participants with the lowest workload allocations for administrative duties had higher overall mean burnout scores.
Conclusion: Results from this study suggest one out of two dental hygiene program directors have symptoms of some type of burnout with the highest prevalence rate in the personal burnout subscale. Findings underscore the need for further research to identify stressors that lead to burnout as well as identify prevention strategies that promote a healthier work climate for dental hygiene program administrators.
Introduction
Workplace burnout is a major psychosocial problem associated with job negativity, decreased work efficiency, and adverse health effects.1-4 Defined as a prolonged response to chronic emotional and interpersonal work stressors, burnout is associated with feelings of emotional exhaustion, increased job negativity, and reduced personal accomplishment.1-3 While depression and burnout share similar traits, burnout involves only work stressors while depression involves both work-related and personal life stressors and issues.1,4 Burnout is fostered by unsuccessful attempts to cope with workplace stress over time.3,4 It has been reported as a frequent occurrence in many service-related professions throughout the world and research suggests high prevalence rates in both teachers and health care providers.5-15
The World Health Organization (WHO) describes burnout as an occupational syndrome, rather than a medical condition, that occurs when poorly managed workplace stress becomes a chronic condition.16 Others have described burnout as a disharmony between the individual and the work environment leading to both physical and mental health issues.10-13 Clinical manifestations of burnout include headaches, GI problems, sleep disturbances, eating disorders, and muscle aches11,16 Psychosocial issues include workplace fear, anxiety, cynicism, lack of motivation, disillusionment, decreased self-efficacy, energy depletion, and impaired job performance; these psychosocial impacts have also been connected to substance abuse issues.12,16 Burnout in health care professionals has been linked to patient safety issues, increased health care costs, and workforce well-being.17-20 Moreover, increased medical errors and poorer patient outcomes have been linked to professional burnout.17-21 For example, Shanafelt et al. found physicians with high levels of burnout reported three times the number of medical errors as compared to non-burnout physicians.21
Program administrators of academic departments may be particularly prone to burnout.22 Being responsible for day-today program operations, overseeing and hiring faculty, budget concerns, accreditation, increasing teaching workloads, service requirements, and in some cases scholarly activities and research, are all important administrative functions leading to stress and possible burnout. Research suggests a high correlation between program director turn over and burnout.22-24 O’Connor et al. found one third of medical residency program directors experienced burnout and half considered resigning in the preceding year of the study; in just four years, 50% of medical residency program directors had changed nationally.22
In health care programs, changing of program directors is costly, may negatively impact program stability, and affects faculty, patients, and students.22-23 Moreover, research suggests burnout affects the longevity and quality of academic careers, and female directors tend to experience higher levels of burnout than their male counterparts.22-25 For example, Walter et al. found women program directors of athletic training education programs had significantly greater emotional exhaustion levels than men, although tenure-track program directors had higher emotional exhaustion scores than tenured directors, regardless of gender.26 Windover et al. also found burn-out among program directors was strongly associated with work-home conflicts, more commonly reported among female program directors than males.3
There is a gap in the literature related to burnout in dental hygiene program administrators and whether they are affected by workplace burnout. However, several studies have researched levels of burnout among academic program directors.22-25 Porter et al. surveyed family medicine program directors with nearly one third reporting high emotional exhaustion burnout scores.24 Similarly, De Oliveria et al. found that 52% of anesthesiology program directors were at high risk for developing burnout.23,24 Only one study could be found on burnout involving dental hygiene program directors, with 43% of the participants (n=20) reporting moderate to high emotional exhaustion burnout levels.27 More research is needed to identify whether dental hygiene program directors are affected by burnout, especially since leadership burnout may not only negatively affect the individual, but also the academic unit in its entirety. The purpose of this study was to address this gap in the literature by determining the prevalence of burnout among entry-level dental hygiene program directors; additionally, this study aimed to identify differences in burnout among two-year and four-year program directors and workload status of participants.
Methods
A descriptive survey design was used to collect data regarding the level of burnout experienced by dental hygiene program directors. This study was determined to be exempt by the Old Dominion University College of Health Sciences Institutional Review Board Committee. The 19-item Copenhagen Burnout Inventory (CBI), a valid and reliable measuring instrument, was emailed to 325 dental hygiene program directors of entry-level dental hygiene programs, as reported by the American Dental Hygienist Association.28 Data was collected via three electronic mailings over 6 weeks using Qualtrics (Provo, UT, USA).
At the beginning of the survey, an introductory statement was provided informing participants that participation was voluntary, responses would remain anonymous, and they would be reported in group form only. Voluntary informed consent was understood upon return of the survey. The CBI is divided into three subcategories: personal burnout, work-related burnout, and client-related burnout. In each subcategory, the degree of physical and psychological fatigue and exhaustion is measured as perceived by the individual, that which is related to work, and that which is related to clients/students.28
The CBI includes six items measuring personal burnout, seven items measuring work-related burnout, and six items related to client/student-related burnout.28 Questions are measured on a five-point Likert type scale with some questions assessed by intensity (very low to very high) and others by frequency (never to always). Scoring ranged from 0 to 100, with scores of 1-49 indicating low burnout, 50-74 indicating moderate burnout, 75-99 indicating high burnout, and a score of 100 indicating severe burnout. The survey also consisted of nine questions related to gender, age, academic rank, and program demographics; additionally, two open-ended questions related to personal and professional factors contributing to stress and burnout status, a question regarding leaving an administrative position due to stress, and three questions related to workload. A panel of dental hygiene faculty reviewed the additional questions in the survey outside of the CBI to establish content validity and to test clarity of instructions. Modifications to the survey instrument were made based on the panel’s review.
Descriptive statistics were calculated for overall CBI scores and each subcategory to determine burnout prevalence. Open-ended questions were transcribed and qualitatively analyzed. Responses were coded based on reported personal and professional stressors. All coding was reviewed by a colleague prior to frequency analysis to establish content reliability. Differences in response frequency issues were discussed, and calibration in responses was achieved. Additionally, independent samples t-tests were utilized to compare entry-level program directors at two-year and four-year institutions on burnout levels, as well as those under 50 years old to those 50 or older. Finally, a one-way, between-subjects ANOVA test was utilized to compare various workload subgroups of participants on burnout levels.
Results
Of the 325 program directors invited to participate in the online survey, 127 completed the survey for a response rate of 39.1% (n=127). The majority of participants were female (94.5%), Caucasian (89.76%), and 50 years of age or older (72%). Over three quarters of the respondents held a master’s degree (77%, n=98), while 19% (n=24) held doctoral degrees; five respondents (4%) indicated a baccalaureate degree as their highest level of education. Over two-thirds (67%, n=85) were employed at two-year technical or community college programs while the remainder (33%, n=42) were employed at four-year programs. Demographic characteristics are shown in Table I.
Participant demographics
Results revealed the total average overall burnout score for participants was 46.03, indicating overall low burnout. However, the majority of participants (62.2%, n=79) had scores indicating moderate to high burnout on the personal burnout subscale, with a little more than one third with scores indicating low burnout (37.8%, n=48). On the work-related burnout subscale, approximately one half of the participants (51.2%, n=65) had scores indicating moderate to severe burnout. Data on the client/student-related burnout subscale indicated approximately one third of participants had scores indicating moderate to high burnout (33.1%, n=42). Mean CBI subscale scores for participants were 54.07 (moderate) on personal burnout, 46.79 (low) on work-related burnout, and 37.11 (low) on client/student-related burnout. Frequencies of responses and scores on subscales of the CBI and the item distributions are shown in Table II.
Frequencies of responses and scores on subscales of Copenhagen Burnout Inventory
When comparing two-year program directors to four-year program directors, an independent samples t-test revealed no statistically significant differences on the overall burnout [t(125)=1.16, p=.25, r=.10], personal burnout [t(125)=0.277, p=.78, r=.02], work-related burnout [t(125)=.998, p=.32, r=.08], or client/student-related burnout [t(125)=1.84, p=.07, r=.16] subscales between groups. Additionally, independent samples t-tests indicated no statistically significant differences on overall burnout [t(125)=0.91, p=.36, r=.08] or any of the three subscale scores [personal burnout: t(125)=0.82, p=.41, r=.07; work-related burnout t(125)=0.58, p=.57, r=.05; and client/student-related burnout t(125)=1.14, p=.26, r=.10] when comparing program directors under 50 years old to those 50 years and older,.
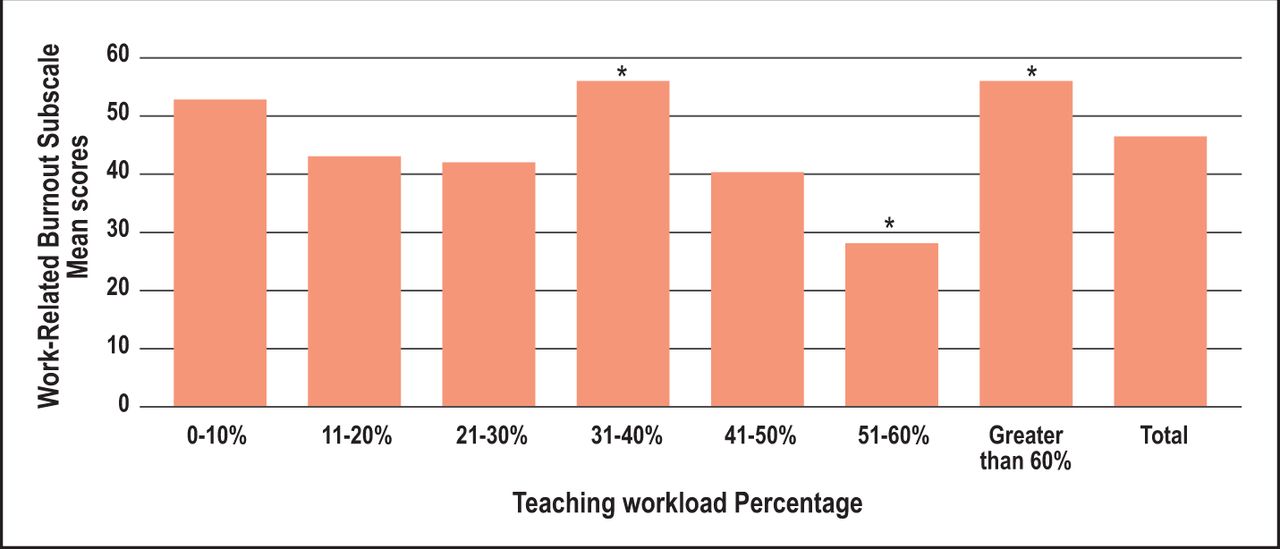
Percentages of workload allocations for administrative, teaching, and research/scholarly activities are summarized in Table III. Comparisons of overall CBI and subscale burnout mean scores in each category were conducted using one-way, between-subjects ANOVA analyses. No statistically significant differences were found for overall CBI mean scores or any of the subscales based on administrative or research/scholarly activity workloads (p-values>0.05). However, there were statistically significant differences identified when comparing teaching workloads for program directors on the work-related burnout subscale (F(6, 126)=2.942, p=0.010). Tukey post hoc tests revealed program directors with teaching workloads of 51-60% indicated significantly lower burnout on the work-related burnout subscale when compared to program directors with teaching workloads of 31-40% (x=29.76, x=55.36, respectively; p=0.045) and greater than 60% (x=29.76, x=55.71, respectively; p=0.028) (Figure 1).
Mean scores on overall Copenhagen Burnout Inventory and subscales based on workload allocations

Work-related burnout subscale scores based on teaching workload percentages.
*p<0.05 (51-60% when compared to both 31-40% and greater than 60%)
While ANOVA revealed few statistically significant findings related to workload, participants with the lowest workload allocations for administrative duties had higher overall mean burnout scores (Table III). Additionally, those with the lowest workload allocation for administrative duties (1-10%) had moderate average scores for the overall burnout scale (x=54.82), as well as the three subscales (personal x=61.11, work-related x=52.38, client-related x=51.39) which were not seen with any other groups of workload allocation. Program directors with high teaching workload allocations (greater than 60%) also had moderate average scores on the overall CBI (x=53.68) and two of the subscales (personal x=58.33, work-related x=55.71), though average scores were low for the client/student-related burnout subscale (x=45.67).
Participants responded to open-ended questions related to personal and professional factors that contribute to stress and overall feelings of burnout (Table IV). Over one quarter of the respondents identified stressors (27.5%, n=35) related to budget concerns, college policies, and college politics, while 21.6% (n=27) identified faculty and/or staff management as major contributory factors to stress and burnout. Another notable stressor recognized by participants was the lack of time during each workday to complete tasks, excessive hours worked, and excessive duties added on an annual basis with no time allotted for completion (16.5%, n=21). When participants were asked whether they had ever considered leaving their position as an administrator due to stress, more than two thirds (69.29%, n=88) responded “yes.”
Response frequencies regarding personal and professional factors contributing to stress or burnout
Discussion
Workplace burnout is a complex interplay of stressors that cause physical, emotional, and mental exhaustion. Decreasing energy, control, and resources in the presence of excessive demands associated with burnout make job satisfaction, motivation, and career growth difficult. The multiple demands of dental hygiene program administrators including administrative issues, budget management, accreditation, and workload allocations may place them at risk for burnout.
Results from this survey indicate approximately one out of two dental hygiene program directors are experiencing some type of burnout, with the highest prevalence scores in the personal burnout category. Personal burnout scores measure how tired or exhausted individuals feel. In general, these results suggest high numbers of dental hygiene program directors are experiencing both physical and psychological fatigue. A comparison of scores from the personal burnout subscale with the work and student-related subscale scores, suggests some of the participants’ exhaustion and burnout levels may be related to non-work factors, such as health or family concerns. Struggling to find a balance between home and work life may also contribute to feelings of exhaustion experienced by female program directors who responded. These findings were also demonstrated with responses to open-ended questions, with participants reporting personal factors contribute to feelings of stress and burnout. These results are similar to a previous study of female athletic training program directors, who were more likely to experience emotional exhaustion than their male counterparts related to burnout.26 In this study, the vast majority of participants were female (95%) suggesting that traditional gender roles may explain the prevalence of high scores on the personal burnout subscale.
Results on the work-related burnout subscale revealed that more than one half the respondents had moderate to severe burnout. This subscale examines the level of psychological and/or physical fatigue, in addition to perceived exhaustion, as it relates to an individual’s work. Findings from this study are congruent with other studies of burnout in health care professions where the number of working hours, higher workloads, and other exhausting work factors, significantly contribute to burnout among health care workers.12,24,27,33,35 When evaluating workload and burnout scores, it was hypothesized that experienced faculty with heavy administrative, teaching, and/or scholarly activity workloads would score higher on professional burnout subscales, however results from this study did not support this concept. Participants scored low to moderate on overall burnout and subscales regardless, of their workload allocations. However, those with the least amount of workload allocation for administrative duties (1-10%) scored in the moderate range on the overall burnout index, as well as all three subscales. No other administrative workload allocations resulted in moderate burnout on all subscales or on the overall instrument. The stress of trying to balance teaching, service, and possibly research responsibilities, with minimal administrative release time, likely contributes to this finding.
Research suggests professionals who maintain constant relationships with other individuals with small recovery times, are more likely to experience prolonged fatigue and burnout.12,29,30 Program directors with minimal release time would experience extremely small recovery times in completing various administrative and teaching tasks, leading to prolonged fatigue and mental exhaustion. These factors may also contribute to data suggesting that the majority of respondents had considered leaving their administrative positions due to stress. Similar results were found with medical residency program directors, where 85% of the participants meeting the criteria for burnout, had considering resigning in the preceding year.22
For most participants, results on the client/student-related burnout subscale indicated working with students was not central to the overall burnout dental hygiene program directors experience; a majority of the respondents scored low on the client/student-related burnout subscale. Program directors may find working with students a rewarding part of their workday, unrelated to administrative or work demands as a program director. It is also possible that as a program director, less time is spent working with students. Moreover, the typically small class sizes in dental hygiene programs and the ability to spend up to two years with the same cohort of students may lend itself to more personalization, resulting in more positive experiences. Several participants noted that they enjoyed working with students and did not feel that this contributed to feelings of burnout.
Results related to other demographics suggest neither age nor academic setting affect overall or subscale burnout scores in program directors, since the mean scores were relatively similar among age groups and regardless of employment setting. This contrasts with other studies indicating that younger participants had higher burnout scores.31-33 While these studies indicated a lack of professional maturity and confidence were possible contributors to burnout, this was not reflected in the results in this study. Dental hygiene program directors had moderate to high prevalence rates of burnout related to personal and work-related factors, regardless of demographics or employment settings.
Moderate, high or severe burnout, whether personal or work-related, would suggest that administrators in higher education need to be proactive in identifying and alleviating burnout in midlevel administrators, such as dental hygiene program directors, since burnout is detrimental to an individual’s overall health and may even effect health care outcomes.3-11 Moreover, burnout negatively impacts the work unit as a whole. Workplace health promotion programs designed to reduce occupational stress, enhance coping resources, and propose interventions for prevention and treatment are recommended to reduce burnout,27,34 On-site childcare and flexible work schedules with remote access may decrease workplace stress. Flextime policies could permit program directors to determine their work hours, while a flexplace policy would allow directors to determine where they will work.35 While full time flexible scheduling may not be always be a realistic option, remote access and part-time flexible scheduling might be feasible and reduce stressors. Increased flexibility might allow program directors to schedule some work hours to align with public transportation and childcare schedules, reducing stress and burnout.35 In general, reviewing and addressing environmental issues contributing to stress, such as noise, lighting, temperature extremes, air quality, and ergonomic factors may also help alleviate stressors in the workplace.36,37
Dental hygiene program directors may benefit from evidence-based stress management workshops designed to promote strategies for dealing with work stressors. Physical fitness activities, in particular, are recommended as stress relievers. However, implementation of physical activity programs may be challenging for overworked dental hygiene directors, especially considering all of the personal factors contributing to burnout. Results from this study support previous recommendations for stress and burnout prevention in this population including training in time management, relaxation, and nutritional guidance.27 Workplace burnout may result in increased turnover of dental hygiene program directors. Institutions of higher education should value stress reduction techniques as a means to decrease turnover rates and increase career longevity of their program administrators.
There are several limitations that may have impacted the results of this study. Program directors experiencing burnout may have been more likely to respond to the survey, resulting in an over-representation of burnout experiences. Burnout prevalence was measured through self-report which may have caused bias in the key variables. The low response rate (39%) also limits generalization of the results; it cannot be assumed that these findings are representative of all US dental hygiene program directors. Additionally, many respondents indicated factors that may influence burnout experiences that were not measured with the CBI instrument, including upper administration, budget constraints, and faculty interactions. Future research should focus on the impact of burnout on career satisfaction and longevity in dental hygiene program directors, prevalence in graduate and post-licensure programs, and best practices for prevention.
Conclusion
Results from this study suggest that one out of two dental hygiene program directors have experienced symptoms of some type of burnout. Among the three dimensions evaluated, the prevalence of personal burnout was the highest level identified, suggesting that work-life balance may be the greatest challenge contributing to burnout among dental hygiene program directors. Furthermore, administrators with the lowest workload allocation for administrative duties had the highest burnout scores, indicating that lack of time to accomplish the required duties associated with their position, may increase burnout. Findings from this study underscore the need for further research to identify stressors associated with burnout as well as identify prevention strategies that promote a healthier work climate for dental hygiene program administrators. Additionally, future research should also explore the impact of burnout on the career longevity of dental hygiene program directors.
Footnotes
This manuscript supports the NDHRA priority area, Professional development: Occupational Health (determination and assessment of risks).
- Received April 7, 2020.
- Accepted June 25, 2020.
- Copyright © 2021 The American Dental Hygienists’ Association





{kind=link}