



Abstract
Purpose: Quality of life is considered a component of patient centered care. The purpose of this study was to examine the relationship between self-reported oral health related quality of life (OHRQoL) and the actual oral health status of children.
Methods: This retrospective cohort study consisted of pediatric dental chart reviews from three clinics. Demographic and dental visit data along with the child’s OHRQoL utilizing the Pediatric Oral health-related Quality of Life (POQL) instrument, were collected. Associations with untreated decay, treated decay, or POQL score were tested, using Chi-square, Fisher’s exact test, 2-sample t-tests, or ANOVA. Linear regression was used to evaluate the effect of statistical confounders in the relationship between untreated decay and POQL scores. Significance level was set to 0.05.
Results: Two hundred ninety-seven out of 336 children had both POQL and caries data. White children and children with untreated decay had significantly more negative POQL scores. Children rating their oral health as “excellent” or “very good” and children with sealants on molars had significantly more positive POQLs. Associations between POQL scores were significant with untreated decay, but not sealants, when considering both variables in the same model. After adjusting for having sealants, POQL scores were on average 7.5 points higher (more negative) in children with untreated decay, than in children without decay (p<0.001).
Conclusions: Collecting OHRQoL data allows oral health providers to easily incorporate patient perceptions in their assessment and care and would ensure that all oral health needs of the patients are being met. This is important for children, who may have difficulty expressing their concerns, particularly in clinical environments.
Introduction
Health care providers have traditionally been taught to use a “medical model” when treating patients. This model treats the person and their social difficulties as medical problems and does not consider any social determinants of health.1,2 The literature has revealed that this medical model is not optimal due to its restrictions on the individual’s self-identity.3 Emergent trends in contemporary health care challenge providers to focus on the individual’s “strengths, interests, positive functions, needs, and characteristics” rather than their disease.4,5 This trend, “personhood,” is considered a vital element for developing patient rapport and trust.
There is an abundance of evidence to support the concept that engaging people in their own health is a fundamental aspect of providing high-quality health care.6–8 For many decades, the World Health Organization has acknowledged that health goes beyond physical attributes and that an individual’s quality of life should be considered as a component of patient care.9 This concept was more recently emphasized in Healthy People 2020 when the United States (US) Surgeon General incorporated quality of life into its measures. A goal was included to promote “quality of life, healthy development, and health behaviors across all life stages.”10 More importantly, health care providers must also be aware that one’s quality of life is determined by the patient, and not the provider.11
The need to consider quality of life is not exclusive to medical providers. This concept is also essential in dentistry. The American Dental Education Association Commission on Change and Innovation in Dental Education (ADEA CCI) 2.0 is a group of dental education stakeholders concerned with establishing oral health education and practice strategies that are responsive, practical, and collaborative. One of the three goals targeted by the ADEA CCI 2.0 in 2017, was person-centered health care.12 It has been asserted that person-centered health care will become the dominant model of health care delivery in the future and members of the ADEA CCI 2.0 have been establishing innovative ways to prepare the dental workforce for this change.13
One practical method to integrate person-centered care into practice is by including oral-health related quality of life questions (OHRQoL) into patient assessments. These questions are based on the assertion that an acceptable level of oral health, comfort, and function is essential to a person’s overall health.14 Oral-health related quality of life has been defined as a “multidimensional construct that reflects, among other things, an individual’s comfort when eating, sleeping, and engaging in social interaction; their self-esteem; and their satisfaction with respect to their oral health.”15
The University of Missouri – Kansas City Oral Health-Related Quality of Life (UMKC OHRQL) theoretical model, a conceptual model designed to be a foundation for “assessing, planning, implementing, and evaluating” OHRQoL outcomes, was developed in 1998 by Williams et al.16 This model was designed to provide dental hygienists with a framework for developing the current person-centered care environment.16,17 Darby and Walsh discussed the importance of OHRQoL when developing the human needs conceptual model (HNM) for dental hygiene practice.17 While acknowledging OHRQoL in the 1993 publication,17 the most recent version of the HNM incorporates eight human needs into the dental hygiene process of care,18 but does not explicitly capture OHRQoL outcomes in the same way as the UMKC OHRQL theoretical model.15 The UMKC OHRQL model requires examination of specific characteristics of the individual including, sociocultural influences, environmental influences, and economic influences,15 thereby capturing the biopsychosocial measures in the assessment process for consideration in the dental hygiene process of care.18 The UMKC OHRQL model was one of several models studied by Brondani and MacEntree.19 In their findings, Brondani and MacEntree acknowledge the UMKC OHRQL model as being one of a few OHRQoL models to illustrate a change in the understanding of oral health to being about more than just illness.19 Yet, a recent study exploring how the UMKC OHRQL model is being applied in education, research, and practice, found that the collection and use of quality of oral health data has been minimal in all three settings.20 While the foundation has been laid for oral health care practitioners to embrace the person-centered care model, it will take greater effort to bring the education and practice community onboard. For the remainder of this paper, OHRQoL will refer to what is known in the literature as oral health-related quality of life.
The literature on OHRQoL as it applies to adult populations has existed for several decades, however, research on OHRQoL in children has been limited. A variety of instruments for capturing OHRQoL in children have been developed in recent years.21–25 The Pediatric Oral health-related Quality of Life (POQL) instrument was developed by a team of researchers from Boston University, with an emphasis on capturing experiences and views of children and has been shown to be valid and reliable as a measure of OHRQoL in children.26 A study by Gadbury-Amyot et al. revealed that asking OHRQoL questions of children could be integrated into the process of care with minimal disruption and time.27 The investigators found that asking OHRQoL questions of children using the POQL instrument only added an average of 6 minutes to the appointment. Additionally, oral healthcare workers noted that having the OHRQoL information directly from the child, provided greater insight about the child and their oral health.
The POQL has been validated across a wide variety of populations.26,28–30 However, Huntington et al. evaluated the POQL in children from a general, metropolitan population in the US, not limited to a specific race/ethnic group, in order to validate the instrument.26 Further studies are needed to demonstrate that the POQL score is a good indicator for a child’s actual oral health in general populations across the US. The purpose of this study was to examine the relationship between demographics, health perceptions, dental characteristics, and self-reported OHRQoL with actual oral health status for children.
Methods
This retrospective cohort study was approved by the University of Missouri-Kansas City Institutional Review Board (#17-040).
Sample population
A mobile school-based dental program in Kansas, a fixed school-located dental program in Missouri, and a fixed safety net dental clinic in Missouri, participated in this study. All three programs were associated with community health centers and were each unique in the way they delivered oral health care services to children. One program employed dental hygienists to deliver oral health care in schools using portable equipment for the delivery of care. Another program employed a more traditional mix of dental workforce personnel where they delivered oral health care services in fixed school-located dental clinics. The third program conducted screenings in schools, but the actual delivery of care was provided by dentists and dental hygienists in two safety-net dental clinics in the community.
Survey instrument
All three participating programs agreed to integrate a short survey containing the POQL instrument into their standard process of care; hereafter, referred to as the Child Self-Report POQL. Dental hygienists administered the survey by verbally asking children the POQL questions and documenting their answers on a paper copy of the instrument. The survey instrument contained six standalone questions, three on child’s self-reported health and oral health perceptions and three on the child’s self-reported dental history, in addition to the ten original POQL items. The ten POQL questions, which were used to generate the POQL score, elicited concerns that the child had regarding their oral health in the last three months and the frequency and severity of those concerns. of those concerns. The survey instrument is shown in Table I.
Child self-report POQL instrument questions
Data collection
Each clinic generated a list of children who had received dental care at specified school-based dental clinics during a three-month window of time. A retrospective chart review was performed for each child on the list. Data was abstracted from the child’s electronic health record including patient record number, demographic data (age at last visit, gender, race, ethnicity, and insurance status), dental visit data (visit date, number of primary and permanent teeth present, number of teeth with treated and untreated decay, number of permanent molars eligible for and having sealants), and Child Self-Report POQL results. Abstracted data was entered into REDCap (Research Electronic Data Capture; http://project-redcap.org/) and subsequently downloaded into Stata 15.1 (Stata Corp; College Station, TX, USA College Station, TX, USA). All data was abstracted from the child’s most recent visit that contained all the dental data of interest and Child Self-Report POQL.
Statistical analysis
The POQL score was calculated from the ten original questions only, according to instructions obtained from the authors of the POQL instrument. Scores could range from 0 (most positive OHRQoL rating) to 100 (most negative OHRQoL rating). Additional standalone questions on child self-reported health and oral health perceptions within the Child Self-Report POQL were dichotomized. Child rated health in general and rated oral health in general were collapsed to “excellent” or “very good” versus “good”, “fair”, or “poor.” The Child rating of their oral health at present day compared to one year ago was dichotomized to “much better” or “somewhat better” versus “about the same”, “somewhat worse”, or “much worse”.
Descriptive statistics were calculated for all variables of interest. Associations between child characteristics and untreated or treated decay was evaluated using Chi-square or Fisher’s exact tests. Two-sample t-tests with unequal variances, ANOVA, or Welch’s ANOVA were used to test associations between the child characteristics and POQL score. To ensure that difference in the location (the state in which the clinics were located) did not impact the relationship between oral health variables of interest and child POQL scores, a test to determine whether the specific state of location was an effect modifier of those relationships was performed using linear regression with robust standard errors. No effect modification of those relationships was found. Multivariable linear regression models with robust standard errors were also used to evaluate the association between child POQL scores and any significant dental variables after adjusting for any variables found to be statistical confounders (significantly associated with both predictor and outcome). The significance level was set to 0.05.
Results
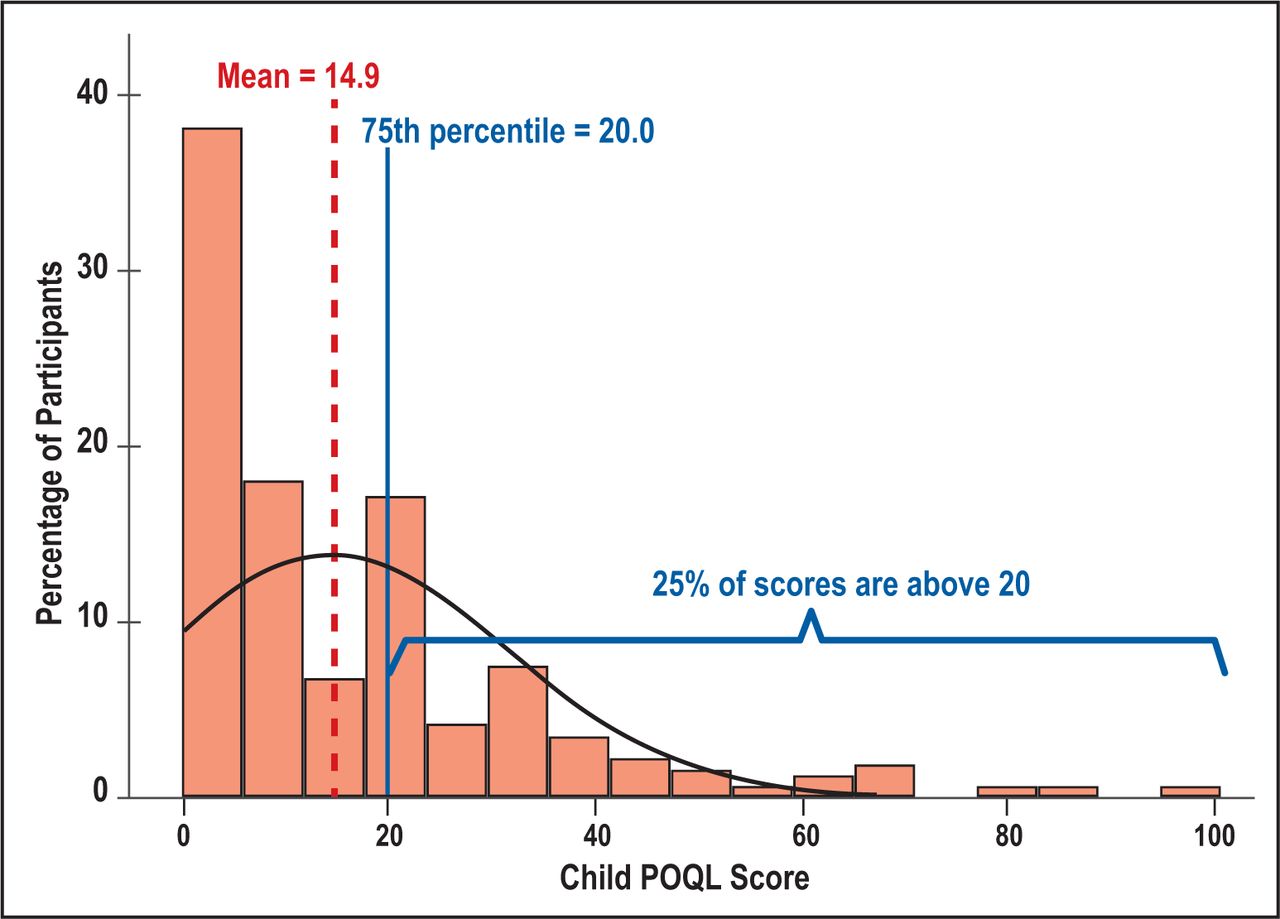
Data was obtained from the dental records of 315 children, between the ages of 8 to 14, who had complete POQL score data. Participants had an average POQL score of 14.9 (± 17.1) where 0 (most positive) was the minimum and 100 (most negative) was the maximum value scored. However, most of the participants had a POQL score of 20 or less (75%) and only 25% of the participants had a POQL score greater than 20 (more negative). The distribution of the POQL scores of the sample are shown in Figure 1. Of the 315 participants with POQL scores, 94% (n=297) had complete caries data charted; 45% (n=134) had untreated decay and 62% (n=184) had treated decay.
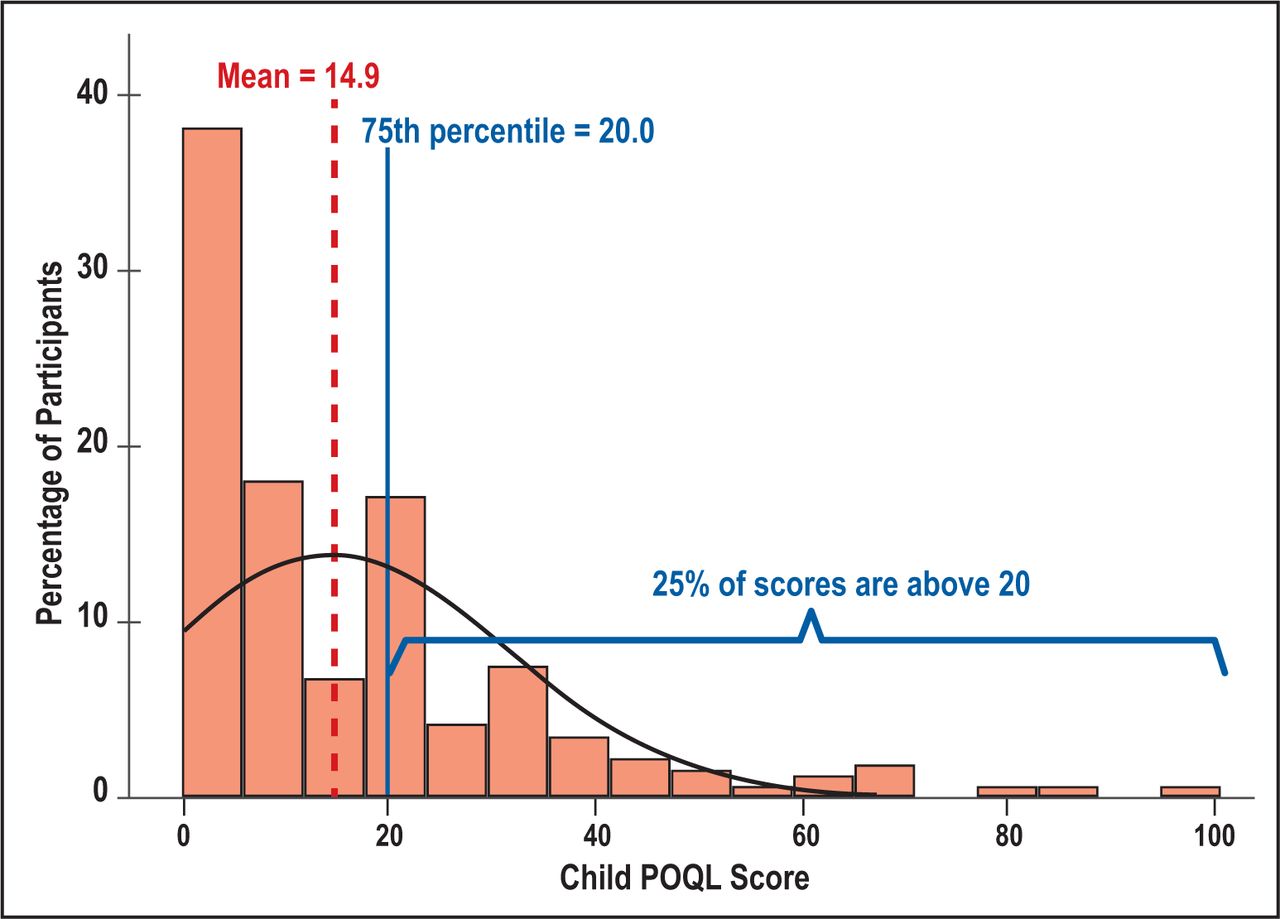
Distribution of child POQL score with a normal density curve showing the Mean and 75th Percentile of the POQL scores overlay.
Demographics
The majority of the children were between 9 and 12 years old (62%, n=183), female (52%, n=155), identified as White race (61%, n=181), and had Medicaid insurance (71%, n=211). Age was not significantly associated with untreated or treated decay nor was it associated with the child’s POQL score. Gender and Hispanic ethnicity were both significantly associated with untreated decay. Males were significantly more likely to have untreated decay than females (52%, n=74 vs 39%, n=60) (p=0.020). Hispanics were significantly more likely to have untreated decay than non-Hispanics (59%, n=71 vs 36%, n=25) (p=0.002). Of the child demographic variables, only insurance status was significantly associated with treated decay. Children with Medicaid insurance were significantly more likely to have treated decay than children with private or no insurance (71%, n=149 vs 62%, n=13 and 33%, n=18 respectively) (p<0.001). Race was the only demographic variable associated with child’s POQL score. White children had significantly more negative mean POQL scores compared to children from other races (16.8 vs 11.5) (p=0.019). Associations between decay and demographic characteristics are shown in Table II.
Decay and POQL scores associations with demographic characteristics (n=297)
Child health perceptions
About half of the children rated their health in general as “excellent” or “very good” (54%, n=160). In contrast, only 37% (n=110) of the children rated their oral health in general as “excellent” or “very good”. Additionally, when asked the question, “Compared to one year ago, how would you describe the health of your teeth or mouth now?”, half of the children (50%, n=147) reported “about the same”, “somewhat worse”, or “much worse.” Oral health ratings were significantly associated with whether the child had untreated decay and with the child’s POQL score. Children who had rated their oral health as “excellent” or “very good,” in general, were significantly less likely to have untreated decay (29%, n=32 vs 54%, n=98) (p<0.001) and had significantly more positive mean POQL scores (10.5 vs 17.5) (p<0.001) than those who rated their oral health as “good”, “fair”, or “poor.” Participants who described their oral health now compared to one year ago as “much better” or “somewhat better” were significantly more likely to have treated decay than children who said it was “about the same”, “somewhat worse”, or “much worse” (70%, n=98 vs 55%, n=80) (p=0.008) Associations of the POQL scores with child health perceptions and dental characteristics and conditions are shown in Table III.
Untreated or treated decay and POQL score associations
Dental characteristics
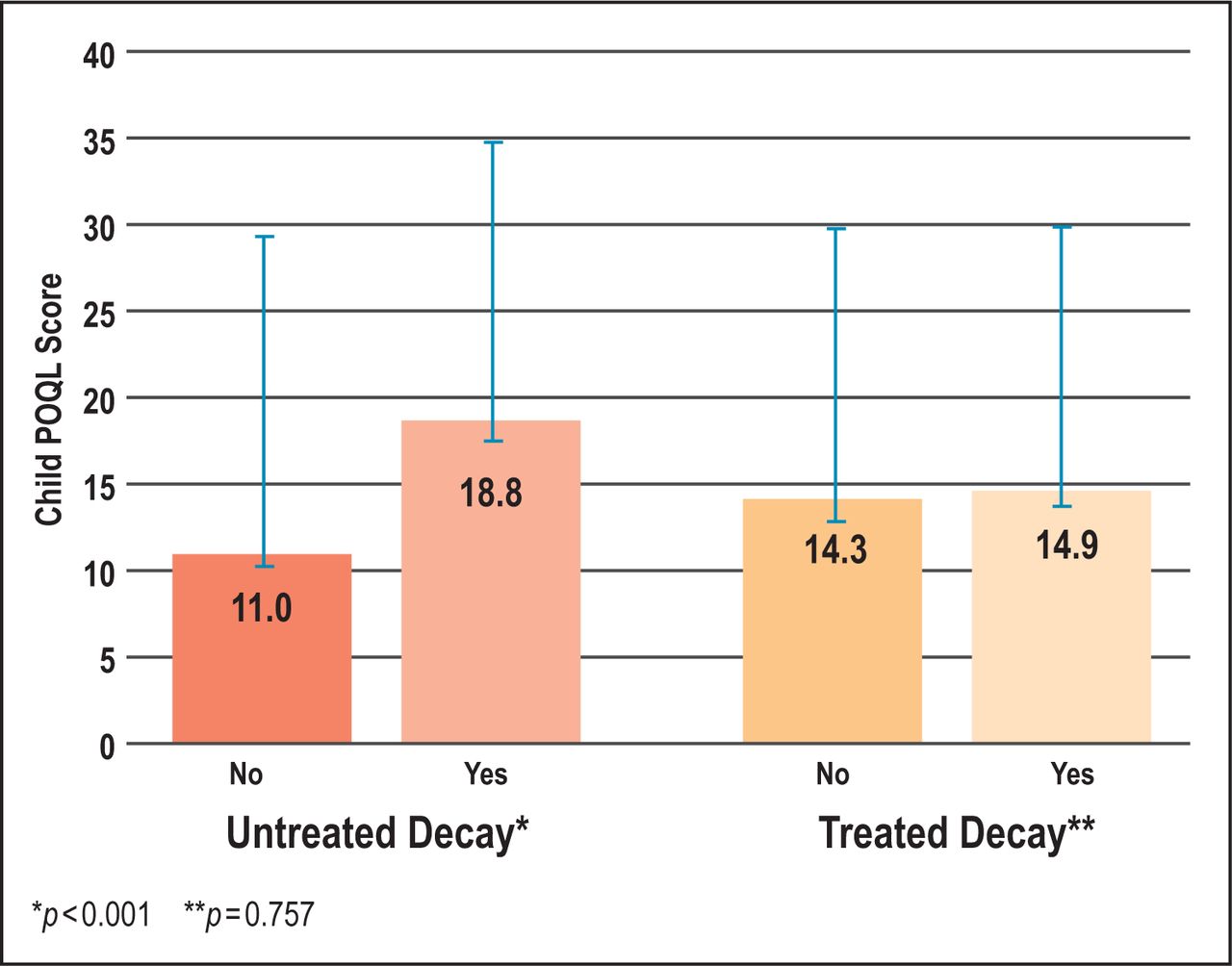
At their most recent dental visit, most of the participants had sealants on molars (70%, n=207). Having sealants placed on molars was significantly associated with untreated decay and child’s POQL score. A child with sealants placed on molars was significantly less likely to have untreated decay (36%, n=75 vs 65%, n=57) (p<0.001) and had significantly more positive mean POQL scores (13.2 vs 17.8) (p=0.037) than a child with no sealants placed on molar teeth. Children with untreated decay had significantly more negative mean POQL scores (18.8 vs 11.0) (p<0.001). Associations between untreated and treated decay with POQL scores are shown in Figure 2.

Associations between untreated and treated decay with POQL score evaluated with 2 sample t-tests with unequal variances.
Adjusted associations with POQL scores
Having sealants on molar teeth and childrens’ perceptions of their oral health were confounders for the association between untreated decay and POQL scores. Therefore, the association between untreated decay and POQL scores was evaluated after adjusting for these variables. The association between untreated decay and POQL scores remained significant in a model adjusting for sealants on molars (slope=7.23, p<0.001), in a model adjusting for child’s rating of their oral health (slope=6.12, p=0.002), and in a model adjusting for both (slope=5.53, p=0.008). Child’s rating of their oral health was significant after adjusting for untreated decay (slope=−5.34, p=0.005) and after adjusting for both untreated decay and sealants on molars (slope=−5.54, p=0.004). However, having sealants on molars was no longer associated with POQL scores in any adjusted model (Table IV).
Associations with Child POQL scores* after Adjustment for Confounding using Linear Regression with Robust Standard Errors.
Discussion
A strong association was found between a child’s self-reported oral health quality of life measure and their actual oral health. Children with untreated decay had more negative POQL scores than children with no untreated decay, similar to the Huntington et al. findings from the POQL instrument validation study. Huntington et al. examined over 3,000 children during a 3-year time period from different schools and dental clinics across a metropolitan area.26 Children with caries, defined as active, untreated decay or any other current dental need requiring immediate treatment, had significantly higher POQL scores than children who were caries free (9.4 vs 6.4) (p=0.003). In this sample of children (n=297), an average POQL for children with and without untreated decay was found to be nearly twice that of Huntington et al. This is most likely due to the differences in regions where the children were living, the Northeast versus the Midwest, and to the much larger sample size of the Huntington et al. study.26 However, even in studies of Native American Indian children, who have been found to have a high caries rate, caregiver reported POQL scores were significantly higher in children having early childhood caries29 or with higher utilization rates of urgent dental services during the past year.31 Notably, the POQL scores were not associated with treated decay, indicating that this particular OHRQoL instrument is sensitive to current oral health concerns and not dental treatment that had occurred in the past.
Results from this study revealed a significantly more positive POQL score in children with sealants placed on molar teeth than children without sealants. Dental sealants have been shown to prevent more than 80% of cavities in the posterior teeth, where the majority of cavities occur32–34 and it is not surprising that children with sealants placed on molar teeth had a more positive oral health quality of life than the children with without sealants. However, using a model that evaluated the associations of POQL scores with both untreated decay and molar sealants together, only the untreated decay was found to be significantly associated with POQL scores. It appears that the relationship between sealant placement and the POQL score was confounded by the child’s current level of untreated decay, suggesting that the OHRQoL in this sample was primarily driven by the child’s current decay status.
Children with Medicaid or private dental insurance in this study had significantly higher rates of treated decay than children without any dental insurance. This may be due to the fact that children with dental insurance coverage are more likely to have treatment performed when needed, than children without insurance coverage.35 White children reported significantly more negative OHRQoL than nonwhite children in this study. It is unclear why this result was found. Future studies should further explore this difference.
Children’s perceptions of their oral health were strongly associated with untreated decay in this study. Children who rated their oral health as “excellent” or “very good” had significantly lower rates of untreated decay than children who rated their oral health as “good”, “fair”, or “poor”. Results from this study demonstrate that the patient’s perception of their present oral health was captured by the POQL instrument.
The Child Self-report POQL instrument shows promise in facilitating person-centered oral health care. The only cost is the minimal amount of time it takes to administer the instrument. Baseline knowledge of a child’s concerns with their oral health can be easily and effectively elicited with the use of this instrument. Follow-up by the oral health care provider on issues that are brought up by the child can aid in improving the child’s overall oral health and oral health quality of life. Oral health providers have reported that the POQL questions help to elicit valuable information, such as a child being bullied because of how their teeth looked, that they would not have otherwise known.27 Traditionally, dental providers in community health settings have not collected quality of life data from the patients during their visits. Oral health care providers should consider integrating OHRQoL instruments as key components of person-centered care, to help ensure that they are able to understand the oral health concerns of their patients, especially children.
Implications of findings and limitations
This study highlights the benefits of utilizing OHRQoL as part of data collection in a person-centered healthcare environment, where patient perceptions play a critical role in their overall assessment and care. It is particularly important to ensure that the oral health care being provided to pediatric patients considers the oral health factors that are important to the individual child.
This study had several limitations. This study was limited to convenience data from three types of dental clinics located in two states, limiting the generalizability of the results. Furthermore, neither the clinics nor the sample population were randomized for enrollment and unmeasured factors could confound associations in the sample. Additionally, each participant’s dental data and the POQL results were taken from the same dental visit. Hence, any causality of the association between POQL scores and dental data would be hard to infer. Future studies should include a larger sample population across multiple states. An important next step in this research would be to conduct a prospective cohort study to evaluate a child’s OHRQoL at the initial baseline visit and evaluate whether the OHRQoL is a predictor for future dental needs.
Conclusion
Higher rates of untreated decay were associated with a more negative OHRQoL in pediatric patients. Oral health care providers should be encouraged to move to a more person-centered care model, where data such as oral health quality of life are collected and factored into patient care. Use of an OHRQoL assessment tool for evaluating a child’s oral health quality of life is strongly associated with their actual dental health and can be a powerful aid in understanding the oral health perceptions and needs of pediatric patients.
Footnotes
This manuscript supports the NDHRA priority area: Population level: Access to care (vulnerable populations)
Disclosure
This study was supported by the National Institute of Dental & Craniofacial Research of the National Institutes of Health under Award Number UH2DE025510. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
- Received October 31, 2019.
- Accepted February 6, 2020.
- Copyright © 2021 The American Dental Hygienists’ Association





{kind=link}
{kind=link}