



Abstract
Purpose: Interprofessional education (IPE) is a means of fostering integration and collaboration between health care professions. The purpose of this study was to evaluate the effect of an IPE educational module on dental hygiene (DH) and physician assistants (PA) students' knowledge of the oral manifestations of menopause and overall confidence in treating these conditions.
Methods: A convenience sample of DH and PA students was used for this mixed-method study. Quantitative data was collected with pre- and post-tests using a modified Readiness for Interprofessional Learning Survey (RIPLS) and a principle investigator (PI)-designed knowledge of menopause test, to determine the students' attitudes and learning levels. Students participated in a one-time workshop that included an educational presentation on the oral manifestations of menopause and a case study exercise using a pseudo-standardized patient. Students from both disciplines, worked in preselected groups to create a patient care plan addressing the oral manifestations of menopause. Qualitative data was collected from student comments.
Results: Study results indicate an increase in participants' knowledge of the oral manifestations of menopause (p<0.05). Results also suggest improved attitudes toward interprofessional teamwork and collaboration (p<0.05), positive professional identity (p<0.05), roles and responsibilities (p<0.05) for IPEC core competencies RR1, RR2, RR3, RR4, interprofessional communication (p<0.05) for IPEC core competencies CC3, CC4, CC 6. Qualitative data from interprofessional care plan formulation and debriefing demonstrated facilitation of gained confidence in applying new skills related to the oral manifestations of menopause.
Conclusion: Patients experiencing menopause are susceptible to oral manifestations. Implementation of an IPE intervention demonstrated correlation between an IPE experience and participants' knowledge, attitudes and confidence. Preparing students to meet the needs of menopausal women may ultimately decrease oral discomfort and improve overall quality of life.
- interdisciplinary Collaboration
- interprofessional education
- oral health promotion
- menopause
- women's health
Introduction
Research supports interprofessional education (IPE) as a means of fostering integration and collaboration between medical and dental health care providers.1-4 The 2010 definition of IPE by the World Health Organization (WHO) states, “Interprofessional education occurs when two or more professions learn about, from and with each other to enable effective collaboration and improve health outcomes.”5 Although interest in IPE has varied over the years, there is an increasing body of evidence supporting the inclusion of dental hygienists (DH) in IPE. 6-8 A recent call to action by Vanderbilt, et al., describes the need for DH to be included in IPE, specifically in regards to dental hygiene and physician assisting education programs.9-11
Since DHs and PAs are frequently the first providers of diagnostic and therapeutic services, IPE between these health care providers is particularly important especially as women from the “baby boomer” generation transition through menopause.12-14 Approximately 65 million women in the U.S. experience oral conditions related to menopause, with 43% of these women reporting oral pain and discomfort as compared to 6% of premenopausal women.14,15 Oral manifestations associated with menopause vary from those that are painful, such as burning mouth syndrome (BMS), to those that are not, such as periodontal disease.16 The range of oral manifestations reported include xerostomia, viscous saliva, increased caries, altered or unpleasant taste, ulcerations, BMS, trigeminal nerve pain, periodontal disease, osteoporotic jaw, and loss of alveolar bone height.17-19 Although recommendations have been made for treating the more specific symptoms such as xerostomia, BMS, and periodontitis, there are no oral care guidelines for menopausal women.16,20 The few recommendations found in the literature generally advise regular dental examinations, professional oral prophylaxis, basic oral care instruction, fluoride use, and the maintenance of a balanced diet including adequate intake of vitamin D and calcium.17,21-23 With the average American woman experiencing menopause at age 51 and a life expectancy of 80 years, addressing the oral health conditions related to menopause plays a critical role in the overall quality of life for this life stage.24
Teaching methodologies in health care training programs incorporating the use of actors trained to portray patients in a simulated clinical setting, (standardized patients or SP), and case studies allowing for new learning to be applied to real-life scenarios following completion of a related lecture or lab, (case-based learning or CBL), have been shown to improve students' confidence within a non-threatening environment.25,26 The use of SP and CBL has been shown to improve students' communication, interviewing, and clinical skills.25,27,28 Research indicates that CBL is commonly used in both DH and PA curricula.29-31 Calhoun, et al., reported that the majority of accredited PA programs use SP as a teaching methodology.32 However, little evidence is found regarding use of SPs in DH education and when reported its use has been limited to tobacco dependence counseling training.26,33 There is a lack of research available regarding use of SPs and CBL in menopause/oral health education across the health care disciplines. The purpose of this study was to evaluate the effect of an IPE educational module on dental hygiene (DH) and physician assistants (PA) students' knowledge of the oral manifestations of menopause, interprofessional collaboration and overall confidence in treating these oral conditions.
Methods
A mixed-method pre- and post-test design evaluated the comparative relationship between DH and PA students related to an educational intervention. Subsequent to Eastern Washington University IRB approval, a convenience sample of DH students from Eastern Washington University (N= 63) and PA students from the University of Washington MEDEX Northwest PA program (N=29), were invited to participate in the study. Inclusion criteria were current enrollment in the DH or PA program and matriculation in the respective program to the point of having had clinical exposure to patients.
DH and PA students were invited to attend separate informational meetings regarding the study. Students who completed a consent form (N=54), were emailed a link to enroll in the study workshop session. The principle investigator (PI) reserved a classroom at the study site equipped with a dental chair and audio-visual equipment for the workshop. All printed forms, tests and supplies were provided to the participants by the PI.
A pseudo-SP was employed to promote student practice in IPE, risk assessment, patient assessment and counseling, and care planning with increased comfort.33 For the purposes of this study, the pseudo-SP did not undergo the minimum of 10 hours of training required to be a true SP,34 but instead completed a one-hour training session. Following the completion of a one-hour training session, the pseudo-SP used a written script specifying signs and symptoms, how to respond to various lines of questioning by providing responses with dialogue, believable patient history of the presenting problem, and other personal information that allowed the pseudo-SP to answer questions participants asked.33
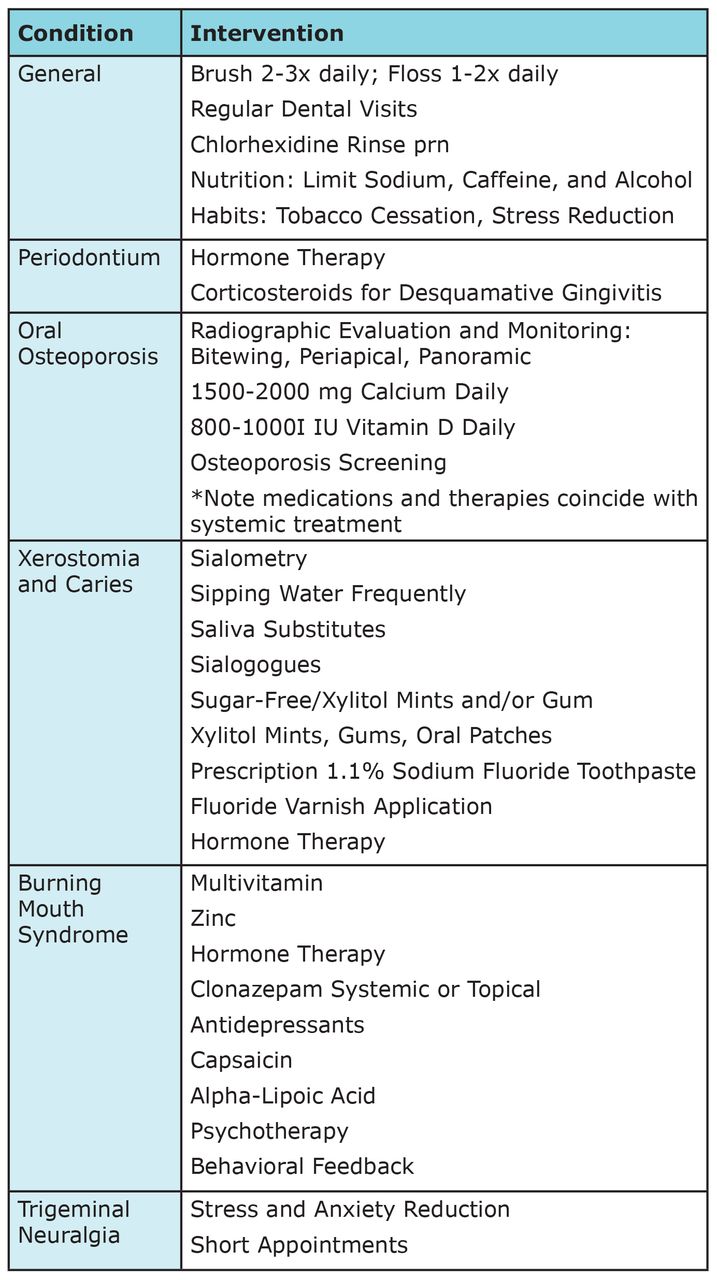
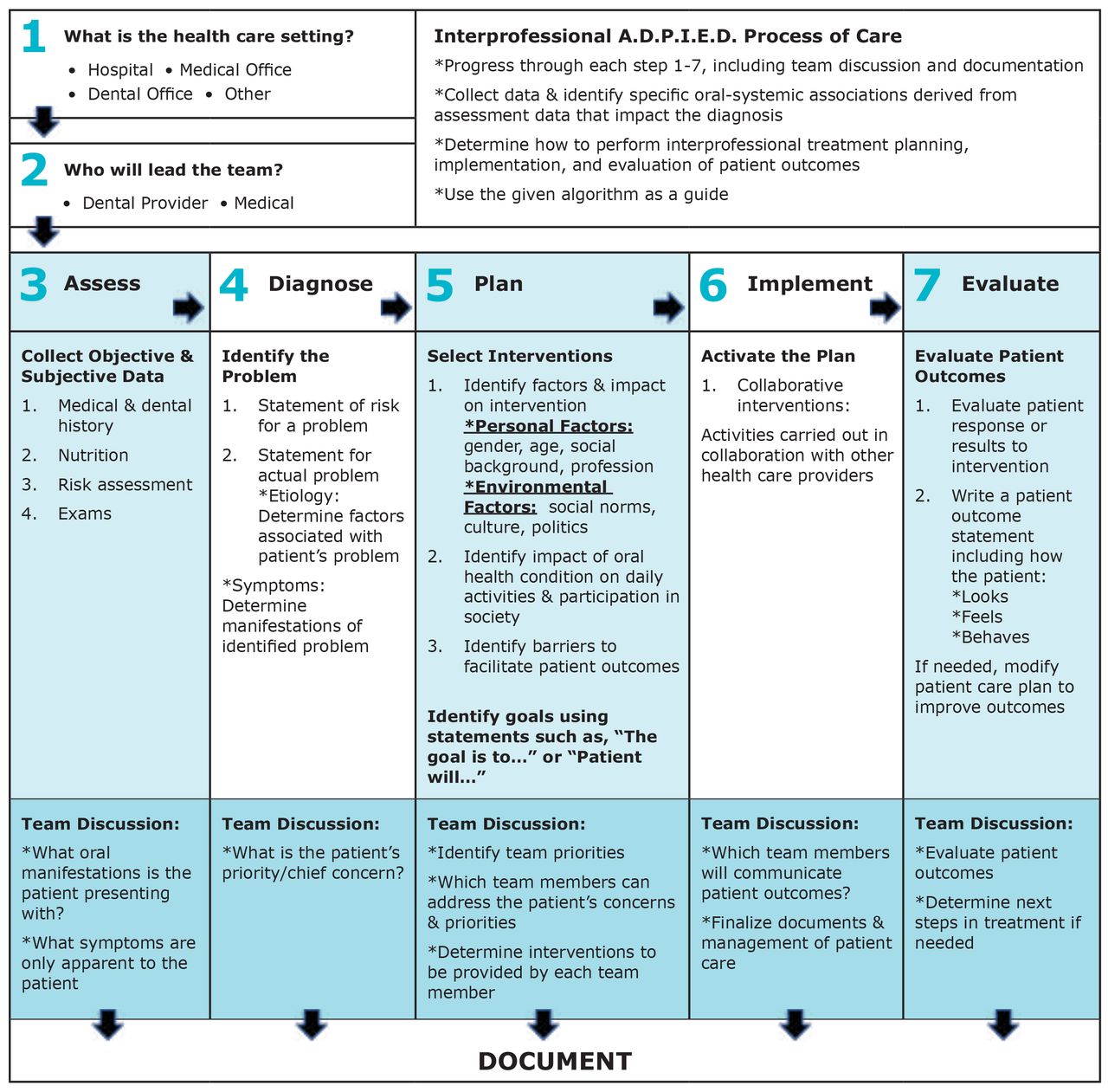
The three-hour workshop began with a demographic survey, menopause knowledge pretest, and a modified Readiness for Interprofessional Learning Survey (RIPLS)35,36 pretest. Upon completion of the baseline assessments, participants listened to a presentation regarding IPE followed by information on the oral manifestations of menopause. Participants were then randomly assigned to one of six heterogeneous interprofessional (IP) teams to create a patient care plan based on a given case study and pseudo-SP presentation. Participants were provided guidelines for management of the oral manifestations of menopause (Figure 1) and the IPE Assessment, Diagnosis, Planning, Implementation, Evaluation, and Documentation (A.D.P.I.E.D.) Process of Care Algorithm (Figure 2), both designed by the PI. All participants received the same educational slide presentation and case study. The same pseudo-SP was used throughout the workshop. Upon completion of the workshop, participants were given a menopause knowledge post-test, modified RIPLS posttest, and participated in a videotaped debriefing interview.
Case Study
The workshop utilized a single case study addressing xerostomia, periodontitis, and oral osteoporosis. The case study format and use of pseudo-SP encouraged participants to assess a multitude of factors, provide patient education and counseling, and develop a collaborative care plan as a team. Each IP team recorded findings, diagnosis, and treatment on a patient care plan worksheet used to collect qualitative data. The case study content was based on information from the literature review and represented a complex menopausal patient scenario requiring expertise from both DH and PA professionals for assessment, appropriate intervention and best outcomes.

Instruments
Instruments used in the current study included a demographic survey, modified RIPLS survey menopause knowledge pre- and post-test, patient care plan worksheet, and videotaped debriefing session. The demographic survey provided descriptive statistics of the sample regarding age, gender, race, professional discipline, years of clinical experience, and prior experiences. A multiple-choice pre- and post-test evaluated for changes in knowledge regarding oral manifestations of menopause and the oral systemic health connection. The knowledge test subsections included women's health and IPE, menopause systemic manifestations, oral manifestations, and oral health management in menopause.
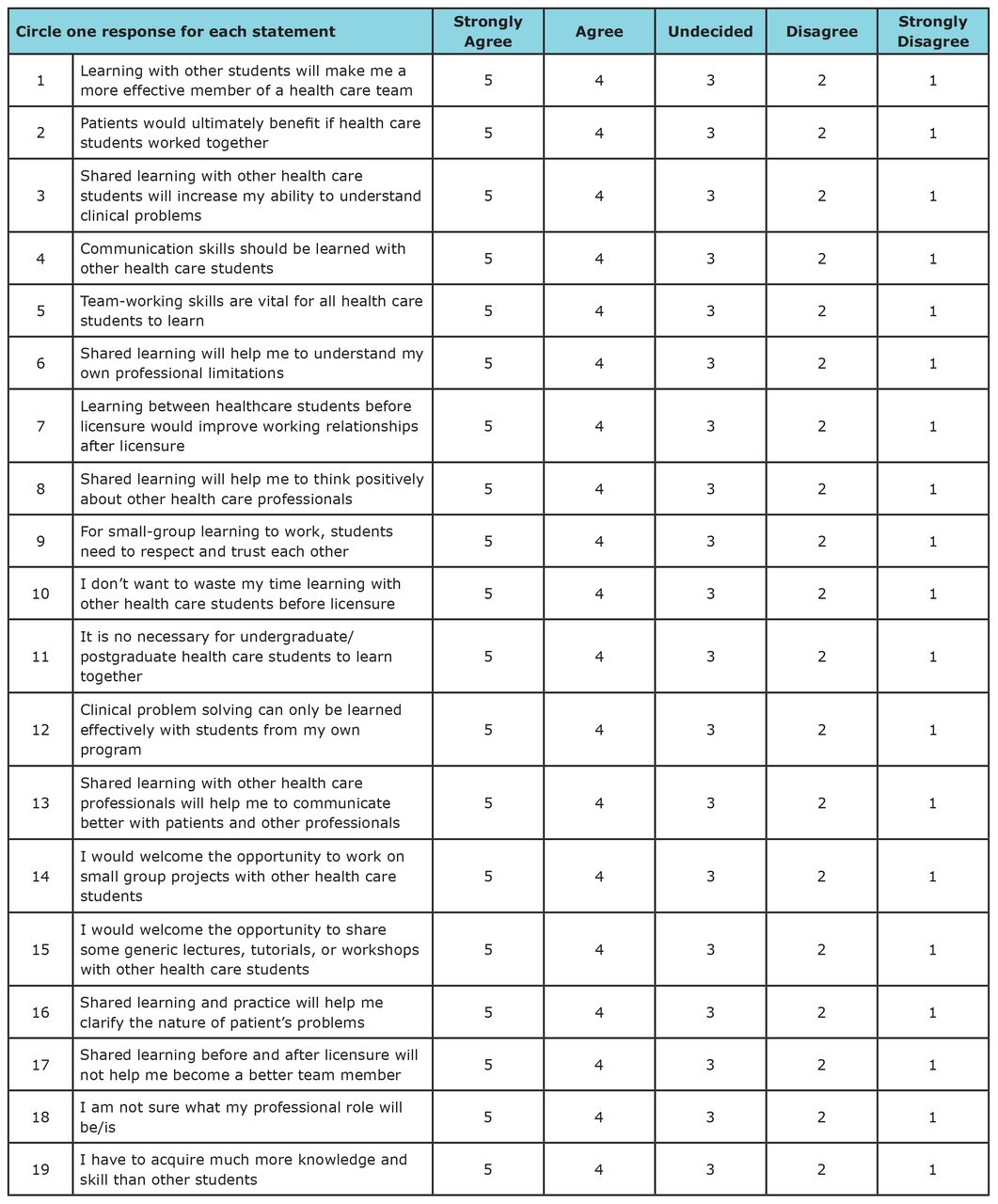
The modified RIPLS was employed as a pre- and post-test. The modified RIPLS, a valid and reliable tool for evaluating IPE, is a 19-item survey with four subscales, using a 5-point Likert scale ranging from strongly disagree (1) to strongly agree (5).35,36,37 This tool evaluated the influence of the educational intervention on participant's attitudes and perceptions of IPE. (Figure 3) The modified RIPLS collected data regarding two IPEC competencies, RR and CC, the foci of this study. The RR domain focuses on using the knowledge of one's own roles and those of other professions to appropriately assess and address the health care needs of the patients and populations served and the CC domain focuses on communicating with patients, families, communities, and other health professionals in a responsive and respon-sible manner that supports a team approach to the maintenance of health and the treatment of disease.2
A patient care plan worksheet was completed by each IP team using a IPE A.D.P.I.E.D. Process of Care Algorithm, synthesized by the PI from the Interprofessional Team Reasoning Framework (IPTRF) algorithm and A.D.P.I.E.D. process of care.38,39 The patient care plan worksheet assisted teams in their responsibilities of identifying oral problems through IP interaction, streamlined data entry, and provided qualitative data.40
Data was also collected via video recording of the participant's debriefing. The PI transcribed the videos to analyze for themes, measure participants' confidence in IP patient care regarding oral manifestations of menopause, likeliness to use knowledge gained from the current study in the future, and feelings about the use of pseudo-SP and CBL. Data was analyzed using SPSS® statistical software (version 23).

Results
The response data represents 69% (n=25) DH students and 31% (n=11) PA students. Sixty-nine percent of the study participants were from the DH program versus 31% of the participants from the PA, providing representative samples from the two programs. The majority of participants were female, Caucasian, DH students with an average age of 21 to 24 years. The PA students ranged in age from 25 to 54 years. One hundred percent of the respondents reported having had some experience with IPE. (Table I)
Descriptive statistics and a paired t-test compared change in knowledge of menopause and its oral manifestations from pre- to post-test in the DH and PA participants. Both groups demonstrated increased knowledge (p<0.05). Table II

The Wilcoxon signed-rank test analyzed pre- and posttest modified RIPLS scores to test the second hypothesis, “Can an IPE module on oral manifestations of menopause improve DH and PA student's attitudes and perceptions about IPE? Table III shows significant changes in perceptions of IPE were indicated in two of the four RIPLS subscales, teamwork and collaboration (p<0.05) and positive professional identity (p<0.05). The participants demonstrated improved perceptions regarding IPEC domains, RR (p<0.05 RR1, RR2, RR3, RR4) and CC (p<0.05 CC3, CC4, CC6) as shown in Table IV.
Demographic Characteristics
Descriptive Statistics for PI-Designed Menopause Knowledge pre/post-test
Data from the IP care plan exercise and debriefing answered the question, “Can an IPE workshop utilizing a pseudo-SP and CBL facili-tate gained confidence of participants in applying new skills related to the oral manifestations of menopause? To explore this hypothesis, participants worked in one of six teams to construct an IP care plan based on PI-designed guidelines for managing oral manifestations of menopause, a given case study, pseudo-SP interaction, and PI-designed IP A.D.P.I.E.D. Process of Care Algorithm. Correct responses included:
Oral Diagnoses: xerostomia, oral osteoporosis, and periodontitis.
Risk Factors for oral manifestations: menopause, nutrition, alcohol, smoking, caffeine, salt, stress, lack of sleep, infrequent dental/medical visits, and poor homecare.
Barriers to care: low medical/dental IQ, finances, and environmental factors.
Table V indicates all teams were able to successfully create an IP care plan using the case study information, PI-designed guidelines for management of the oral manifestations of menopause, and PI-designed IP A.D.P.I.E.D. Process of Care Algorithm. Table VI shows coded debriefing data indicating gained confidence in treatment of the oral manifestations of menopause.
Discussion
Wilcoxon Signed-rank Test Modified RIPLS Subscales Pretest/Posttest Comparison
This study explored the effects of an intervention consisting of a presentation and pseudo-SP case study on the oral manifestations of menopause. Results of the study suggest that the implementation of an IPE workshop for DH and PA students on oral manifestations of menopause imparts new knowledge, gives parti-cipants the opportunity to communicate in small groups and improve attitudes and perceptions toward IPE, and facilitates gained confi-dence of participants in applying new skills related to the oral manifestations of menopause.
This IPE university-based study pro-vided an opportunity to bring attention to the oral manifestations associated with menopause and their relationship to overall health. The results demonstrate an increase in participants' knowledge of oral health for the menopausal patient after completing this one-time workshop. These findings are consistent with those of Christenson demonstrating the positive effects of a single learning intervention.41 Results of the current study are also supported by research demonstrating that both PA and dental students benefit from interactions in IPE.42-44
Prior to participating in this study, the majority of participants demonstrated lack of awareness in the oral health manifestations and oral health management during menopause, as measured by the menopause knowledge pre-test. These findings were surprising given 84% of DH (n=21) and 38% of PA (n=3) in the current study reported experience in treating oral conditions in general.
Previous research suggests lack of specific training in oral health inhibits PAs from providing oral care services.6,7,45-47 Research conducted by Murray and Fried indicates that DHs also need more training regarding the oral manifestations of menopause.48 Therefore, it may be inferred that if PA are not trained to provide oral care services and DH are not trained to recognize and manage the oral manifestations of menopause, they may omit discussions about the oral manifestations of meno-pause when providing patient care. Results from this study support previous research indicating that oral health providers, including DHs, possess greater pot-ential for the detection, monitoring, and prevention of chronic conditions49 which in turn supports the impor-tance of integrating women's health content into the DH curriculum.
Communicating in small IP groups facilitated improved attitudes and perceptions toward IPE through learning about each other's roles and responsibilities. Utilizing the PI-designed IP A.D.P.I.E.D. Process of Care Algorithm and guidelines for management of oral manifestations of menopause, DH and PA students collaborated in teams to create a patient care plan and provide patient-centered care with a focus on assessing and treating oral manifestations of menopause.36,38 The modified RIPLS evaluated students' attitudes and perceptions regarding IPE.50-52 Measured aspects of students' attitudes and perceptions toward IPE showed significant improvement in IP teamwork and collaboration and positive professional identity. Overall, there were no significant changes in negative professional identity or RR domains. However, item number 17 in the RR domain was shown to be statistically significant.
Wakely et al. had similar findings to this study, reporting significant changes in all subscales except RR.53 The lack of significant change in negative professional identity and RR domains may be because initial scores were already high, or because this was a one-time study limited to a three-hour time allotment. Also, the study evaluated two IPEC competency domains, RR and CC. Pre- and post-test scores align with those of Christenson and demonstrate significant growth in CC and RR.41 This suggests implementation of IPE has the potential to help students improve their communication skills with other disciplines. This is particularly important for DH educators, because the Commission on Dental Accreditation (CODA) standards for dental hygiene programs require competence in comprehensive collection of patient care data (Standard 2-13), interprofessional communication and collaboration (Standard 2-15), and problem solving strategies related to comprehensive patient care and management (Standard 2-23).54
Wilcoxon Signed-rank Test Modified RIPLS Questions Determining Changes in IPEC Core Competency Domains Roles and Responsibilities (RR) and Interprofessional Communication (CC)*
Team Care Plan Descriptive Statistics
Use of a pseudo-SP and CBL promoted shared responsibility and the study participants gained confidence in the care of the menopausal patient thus further supporting Gibson-Howell's findings demonstrating that the application of students' knowledge increases learners' acquisition and retention of knowledge.55 The current study also supports results similar to Feely's et al. research demonstrating the value of utilizing a pseudo-SP for communication training and health education promotion.56 This study's results are further strengthened by research demonstrating that when students work collaboratively to solve a case study, they are required to develop skills needed in the real-world including critical thinking, problem-solving, prioritization, working with others, and appreciation of roles.56,58 Working on a case study can facilitate students' gained confidence in their knowledge of content, success in group work, and the ability to look at a problem from various viewpoints, process it, and use critical thinking to reach a solution.56,57 Collaboration with other disciplines encourages greater communication, improved access and overall quality of care.59
A primary goal of the pseudo-SP CBL exercise was for DH and PA students to participate actively in developing a care plan. The IP groups were also encouraged to use a presentation outline containing the PI-designed oral care guidelines for menopause. No comprehensive guidelines for oral care during menopause existed prior to the implementation of the current study.16 Data from the study's care plans revealed that the participants were able to function as a team, even with minimal familiarity with each other. Results support small group, CBL using a pseudo-SP enhances knowledge acquisition as well as confidence in application of new skills supports previous research findings demonstrating that SP and CBL positively impacts students' confidence, understanding, communication, and clinical skills.25,26,33 Use of pseudo-SP and CBL incorporating the PI-designed IP A.D.P.I.E.D. Process of Care Algorithm, triggered the required decision points in the care plan. Similar to previous research, the current study demonstrates the integration of oral manifestations of menopause into the A.D.P.I.E.D. process of care.60 Study results suggest that the IP A.D.P.I.E.D Process of Care Algorithm may be a useful tool for educators charged with developing IP experiences. Furthermore, incorporation of this tool in DH curricula may enhance IP skills and confidence needed as dental hygiene scope of practice expands to meet population needs.61
Although no IPE curricula currently exists between DH and PA programs, this study validates that improvements in IP communication and understanding of roles and responsibilities may enhance opportunities for collaborative practice.10 Debriefing data demonstrated that this workshop permeated some of the silos separating medicine and dentistry, providing hope that a new generation of practitioners will develop professional identities and categorizations that deconstruct traditional roles.
There were limitations to this study that should be noted. Data was collected from a one-time study of a small sample, thus limiting any broad generalizations. Due to the volunteer nature of the study and the IPE credit received for attending, participants may have been extrinsically motivated to participate in IPE. The effectiveness of the group work may also have been limited by student fatigue, a lack of knowledge regarding their respective examination standards and scope of practice as well as discomfort discussing certain women's health issues such as vaginal dryness. It should also be noted there was an unequal distribution of students representing the DH and PA professions in each team which may not have authentically represented the IP team dynamic in a real clinical setting. Team members also had varying levels of didactic and clinical experience.
Long-term studies are recommended to determine if the knowledge and skills gained from a one-time intervention regarding oral manifestations of menopause occurring as part of the education process, translates to incorporation into clinical practice. Future research is also recommended to identify evidence based oral care guidelines for menopause and to continue to evaluate the PI-designed, IP IPE A.D.P.I.E.D. Process of Care Algorithm. Future studies should include a larger more diverse group of students, and include other healthcare professions. It is also recommended that the variations in knowledge during the DH education process be evaluated to determine the ideal point for introducing IPE in the curriculum.
Conclusions
Patients experiencing meno-pause are susceptible to oral manifestations. Implementation of an IPE intervention demonstrated a correlation between an IPE experience and participants' knowledge, attitudes and confidence. Utilization of a process of care algorithm and guidelines for management of the oral manifestations of menopause promoted IP collaboration and comprehensive oral care management for the menopausal patient. Preparing students to meet the needs of menopausal women may ultimately decrease oral discomfort and improve overall quality of life. Additional IPE experiences, allowing DH and other health care disciplines to learn about, from and with each other has the potential to improve knowledge, perceptions, and confidence in patient care.
Footnotes
Windy L Rothmund, RDH, MSDH is a member of the dental hygiene faculty; Ann D O'Kelley-Wetmore, RDH, MSDH is an associate professor and department chair; Merri Jones, RDH, MSDH is an assistant professor; all in the Department of Dental Hygiene, Eastern Washington University, Spokane, WA.
Michael B Smith, DHEd, MPAS, PA-C is a lecturer and site director for the MedEx Northwest PA Program, University of Washington, Department of Family Medicine, Spokane, WA.
This manuscript supports the NDHRA priority area Professional development: Education (interprofessional education)
- Received June 26, 2017.
- Accepted October 16, 2017.
- Copyright © 2017 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}