



Abstract
Purpose: The objective of this study was to assess college students' behaviors, attitudes, and knowledge regarding hookah smoking.
Methods: A convenience sample of 200 students from various majors, including allied health and nursing students, was used to conduct this study at a university located in the Midwestern United States. Respondents were asked about any past, current, and future hookah smoking behaviors. Likert-scale questions were used to assess attitudes regarding hookah smoking. Respondents were also asked ten questions regarding the history of and health effects of hookah smoking. A knowledge score was calculated based on the number of questions answered correctly. Survey data were analyzed using independent sample t-tests and a one-way ANOVA test at a significance level of p<0.05.
Results: A total of 200 out of 204 surveys were returned, yielding an overall response rate of 98%. Sixty-eight percent of respondents reported having participated in hookah smoking, with time of first-time use ranging from 14 to 21 years of age. About one third of the respondents (32%) reported participating in hookah smoking in the previous 30 days. The majority (68%)of respondents estimated that they would not participate in hookah smoking in five years time. Over half of the respondents reported that it is socially acceptable to participate in hookah smoking and 43% reported that hookah smoking has relaxation benefits. The overall mean knowledge score regarding the health effects of hookah usage was 4.4 questions correct out of 10. There was a significant difference (p=.038) in the mean knowledge scores between hookah users (4.70) and non-users (3.81). When comparing the knowledge of allied health and nursing majors to all other majors, the allied health and nursing group scored significantly higher (p=.017) than the non-allied health and nursing majors, with mean scores of 4.80 and 3.81, respectively. Thirty-nine percent of the respondents were unaware that hookah tobacco and related smoke can cause oral cancer.
Conclusion: Based on the high rates of college student use and the low knowledge scores, this study supports need for more education about hookah smoking and its health consequences.
Introduction
Hookah smoking, commonly known as waterpipe smoking, has become a popular trend in recent years, especially among high school and college students.1-4 While many students find hookah smoking to be socially acceptable, they may not understand the negative impact it can have on general and oral health.5 Hookah smoking has recently been deemed a growing threat to public health due to its popularity and associated negative health effects.6, 7 An estimated 9,750 people in the United States (U.S.) will die from oropharyngeal cancer annually; many due to various forms of tobacco use, including hookah.8 Even with the harmful effects of hookah smoking coming to the attention of health experts, little research has been conducted on public knowledge about hookah smoking. Dental hygienists often spend 45-75 minutes with patients, placing them in a prime position to educate patients, particularly young people, about the dangers of hookah smoking.9
Hookah, or waterpipe smoking, is thought to have originated in the Middle East. It also has links to India and North Africa and is believed to have begun as a social tradition dating over 500 years ago.1, 6, 10, 11 Hookah smoking is also known as narghile, argileh, hubble-bubble, shisha, and goza, depending on the culture and country.12 Hookah continues to be common in the Middle East, while it is increasing in popularity in countries such as Britain, France, Russia, and the United States.1-4
The basic hookah waterpipe consists of four main parts: the head, body, water bowl, and hose connected to a mouthpiece. (Figure 1)1,12 Tobacco is placed in the head, which is often covered with perforated aluminum foil. Charcoal or burning embers are placed on top of the perforated foil to heat the tobacco. The user inhales through the hose that is connected to the mouthpiece, which in turn, draws air over the lit charcoal. The heated air then passes through the tobacco and produces the smoke which is drawn through the body of the waterpipe and is cooled as it passes through the water in the water bowl.11,13
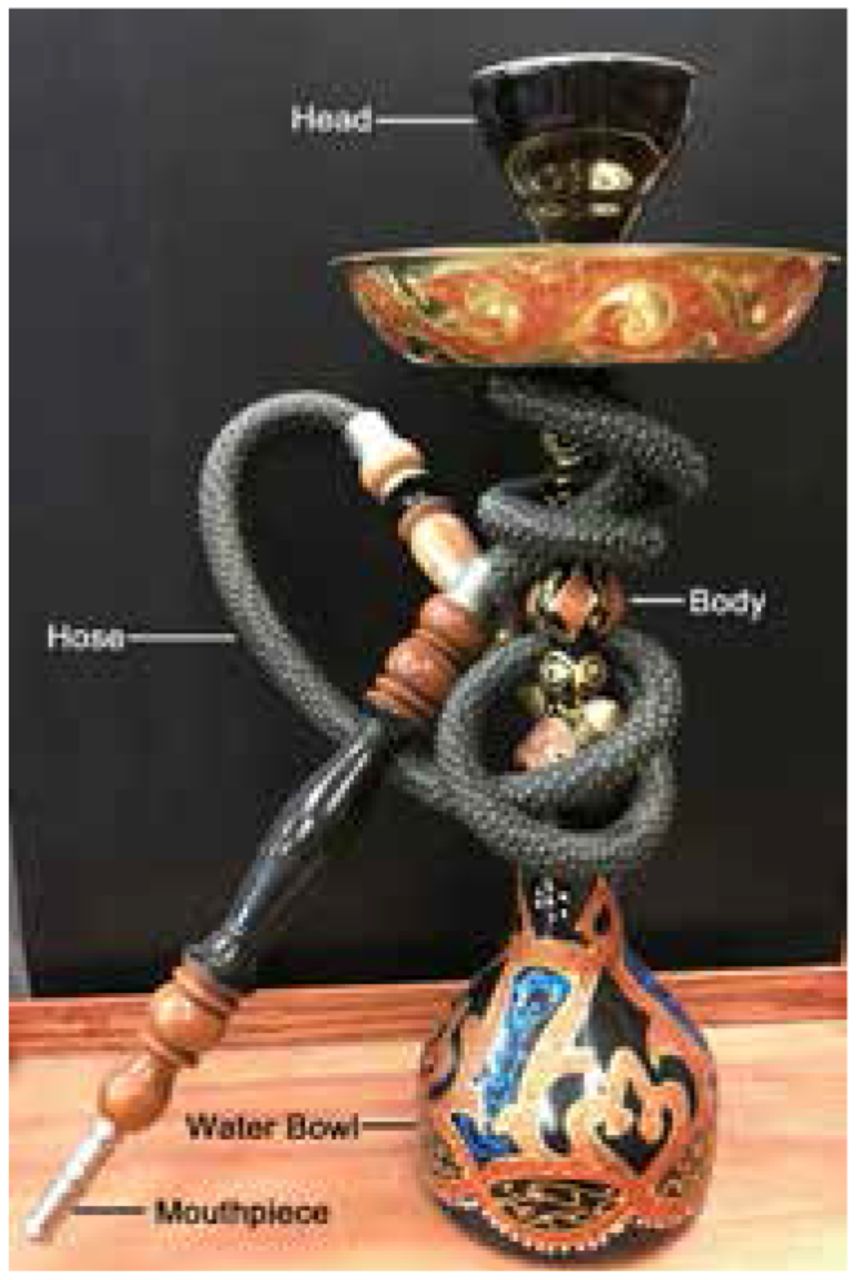
Basic Hookah Waterpipe
Tobacco used in hookahs is frequently moist and sticky and often contains molasses, honey, and other sweeteners and flavorings. Frequently used flavors include strawberry, cappuccino, toffee, cotton candy, orange, white grape, and chocolate mint.6, 14 The aromatic nature of the flavored smoke appeals to younger users and tends to mask the harshness of the tobacco.6, 11, 12 Hookahs have also been reported to be used for smoking other substances besides tobacco, including marijuana.15
Hookah tobacco smoke contains many of the same hazardous chemicals found in cigarette smoking including: nicotine, tar, and carbon monoxide (CO). In addition, hookah smoking produces the carcinogenic polycyclic aromatic hydrocarbons released from the burning of tobacco as well as from the coal used to heat the tobacco.16-18 The emissions produced from charcoal combustion create health concerns for both the users and bystanders.19 Volatile aldehydes (formaldehyde, acetaldehyde, acrolein propionaldehyde, and methacrolein) are toxicants known to cause pulmonary disease. Additional hazardous exposures include phenols and heavy metals, such as cobalt, arsenic, chromium, and lead.16-18
Studies have shown that hookah smoking contains 1.7 times higher concentration of metals, 6.5 times the amount of CO, and 46.4 times the amount of tar when compared to the equivalent nicotine dose found in cigarettes.7, 11 Because a hookah smoking session may last roughly 60 minutes, a hookah smoker may consume approximately 200 times more smoke during a hookah session as compared to a single cigarette.7, 12 In terms of inhalation of smoke volume, one 60-minute hookah session is considered the equivalent of smoking 60 to 100 cigarettes.18, 24 Additionally, the literature indicates that hookah use may serve as a gateway to other tobacco products such as cigarette smoking.3, 20 In light of these significant health risks, questions regarding hookah use should be part of the tobacco cessation and prevention conversations dental hygienists have with their patients on a regular basis.
Cigarette smoking has been linked to 480,000 deaths per year in the United States, including 42,000 deaths due to secondhand smoke exposure.21 A limited number of studies have been conducted on the health risks of hookah use, although existing research suggests that the health risks are similar to those of cigarette smoking including the noteworthy risk of tobacco addiction.6, 22 Hookah smokers inhale more smoke (including nicotine), in a single session compared to cigarette smokers, which increases their risk of addiction.2, 11 Other health consequences of long-term tobacco use include: esophageal squamous cell carcinoma, nasopharyngeal cancer, lip carcinoma, cardiovascular disease, lung cancer, bladder cancer, pancreatic cancer, respiratory disease (chronic bronchitis and air inflammation), elevated heart rate and blood pressure, elevated carboxyhemoglobin levels, infertility, and changes in voice and pitch.5, 16, 23, 24 Infectious diseases, acquired from sharing the hookah mouthpiece, include Mycobacterium tuberculosis, Hepatitis C, Helicobacter pylori, influenza, Epstein-Barr virus, herpes simplex virus and a variety of respiratory viruses.6, 23 In addition to oropharyngeal cancers, specific oral health effects of hookah smoking include increased risk of periodontal disease, acute osteitis, oral candidiasis, and stained teeth and restorations.7, 16
Although firsthand smoke inhaled by the smoker poses significant health risks, it is important to note that the inhalation of secondhand smoke poses similar health risks.23 Secondhand smoke from a hookah session is of particular concern since it contains smoke from the tobacco as well as the toxicants from the charcoal.12 Hookah smoke contributes to a higher level of indoor particulate matter as compared to cigarette smoke and it common for people to smoke hookah indoors.19 Over the last twenty years, approximately 200-300 hookah bars have opened in the United States, many are in university towns.19 Patrons frequenting these establishments are not always aware of the dangers of the particulate matter or secondhand smoke related to hookah use. Additionally, statewide smoke-free air laws vary and hookah bars or cafes, cigar bars, and smoke shops may be exempt or fall into loopholes that are not fully addressed by city and state ordinances.6, 22, 25
There are many misconceptions among youth who are either smoking hookah or exposed to hookah via secondhand smoke. Hookah smokers may have the perception that because these products are aromatic and sweet smelling, that they are less harmful than other forms of tobacco use.2 In addition, because smoke is cooled as it passes through water, it produces a less irritating experience making inhalation more enjoyable.22, 26 Other users have reported the erroneous belief that the water filters the toxins as the smoking session continues. Some hookah tobacco is marketed as “herbal tobacco,” which may lead consumers to believe that this is a healthier product than traditional tobacco. However, herbal and sweetened tobaccos, nonetheless, contain tar and carcinogens.10
Hookah use in the United States is a growing public health concern particularly in regards to college students, although differences have been reported in student gender, ethnicity as well as in the location and size of the university. A national survey completed over the fall of 2008 to the spring of 2009 (N=82,155) showed that 23% of college students reported smoking hookah.4 Several other studies demonstrate that males are more likely than females to smoke hookah,5, 27, 28 with students of Arab decent being more likely than non-Arab students to participate in hookah smoking.28 Jarrett et al. reported that the prevalence of hookah smoking was significantly higher in university towns with populations greater than 500,000, particularly in Northeastern or Western states;4 Midwestern states have been shown to have lower rates of hookah use.4, 5, 26, 27, 29
Despite increasing trends of hookah use and recognized oral health risks, little research has been published on hookah or waterpipe smoking in dental journals.24 The purpose of this study was to assess college students' behaviors, attitudes, and knowledge regarding hookah smoking and to examine the differences in knowledge between health care professional students and those in other disciplines as well as between those who engage in hookah smoking and those who do not.
Methods
Institutional Review Board approval was obtained from the Minnesota State University (MSU), Mankato for this survey research study. The survey instrument consisted of questions about a student's past, current, and future hookah smoking behaviors. Likert-scale questions were also used to assess attitudes regarding hookah smoking. Knowledge regarding the history and health effects of hookah smoking was also assessed. A researcher-developed series of ten true/false questions based on current hookah research was created and the survey items were reviewed by several experts in the health field. The survey was pilot-tested on 20 individuals with the purpose of testing the survey items for understandability and the appropriateness of the instrument design. The pilot test results demonstrated that items were understandable and the response option “I don't know” was added to the knowledge portion to eliminate respondents from simply guessing.
A convenience sample of MSU professors known to the primary investigator were emailed for permission to distribute the surveys during regularly scheduled class time. Professors from multiple disciplines agreed to allow the primary investigator to describe the study and distribute the surveys. Classes ranged in size from 15-30 students. The paper based paper surveys included the informed consent; students gave their implied consent by completing the anonymous survey, Only students enrolled at the university were invited to take the voluntary survey; there were no specific exclusion criteria. Surveys were distributed to a total of 204 students from various majors including allied health and nursing. Descriptive statistics, independent sample t-tests and a one way ANOVA test (p<0.05) were performed using SPSS version 21.
Results
A total of 200 out of 204 surveys were returned, yielding an overall response rate of 98%. (Table 1) The average age of participants was 21 years, with an age range of 18-36 years. Overall, 68% of the respondents were female, and 85% were Caucasian. (Table II)
Reported Academic College of Participants' Majors
Hookah Users
Descriptive summary statistics were generated to describe behaviors of hookah users including: use and exposure over a lifetime and during the last 30 days; where and with whom users smoke hookah; smoking session length; self-predicted future hookah use. In this study, 68% (n=136) reported they have participated in hookah smoking, with a very minimum of one or two puffs in their lifetime. The average age of first use was 17.9 years, with a range of 14-21 years. This study found 83% of males and 61% of females had smoked hookah. Usage rate in Caucasian students (68%) was similar to non-Caucasian students (64%). Thirty-two percent of participants indicated that they have participated in hookah smoking in the last 30 days. Of those who participated in the last 30 days, 93% stated they smoked hookah between 1-5 times. Two respondents stated they smoked hookah 6-10 times in the last 30 days, and one respondent stated he/she smoked hookah 16-20 times in the last thirty days.
Sex and Race/Ethnicity of Overall Participants, Users, and Non-users
Locales where hookah smoking occurs (n=136)
Length of hookah smoking session in previous 30 days (n=43)
Locales where hookah is smoked are described in Table III, with a friend's or acquaintance's home cited as the most common location (62%). In addition, 93% of students reported that they smoke with more than one friend in most instances. Few reported smoking with just one friend or with family members, and none reported smoking hookah alone.
Reported lengths of hookah smoking sessions ranged from under 10 minutes to greater than 90 minutes. (Table IV) The most common reported smoking session length was 31-50 minutes (35%). While the majority of users (68%) believed they will no longer be smoking hookah in five years, 28% believed they will smoke less than once per month, and 4% believed they will smoke monthly. None of the respondents reported believing that they will be smoking hookah on a daily or weekly basis in five years. Responses regarding exposure to secondhand hookah smoke included: no exposure (37%), annually (16%), monthly (33%), weekly (13%), and daily (2%).
Attitudes, Beliefs and Knowledge
In addition to hookah exposure and use, this study examined participants' familiarity, attitudes, beliefs, and knowledge regarding hookah. Seven percent of participants were not at all familiar, 74% were slightly-familiar to familiar, and 19% were very familiar with hookah smoking knowledge. The mean knowledge score for overall participants (N=200) was 4.4 questions correct out of 10; the “I don't know” response was calculated as an incorrect answer.
Over half of participants (54%) stated hookah smoking is socially acceptable, with 21% reporting positive social benefits. Almost half of participants (43%) believed hookah smoking has relaxation benefits. Users perceive greater positive social benefits from hookah smoking (25%) than non-users (11%). As expected, more users believe hookah smoking is socially acceptable (68%) than non-users (22%). However, the majority of both users (67%) and non-users (69%) stated that hookah use is increasing in popularity.
Response to knowledge questions for users (n=136) and non-users (n=64)
Knowledge scores among selected age groups (Bonferroni Post Hoc Test)
Knowledge scores among majors and users versus non-users (independent-samples t-test)
In order to compare any differences in knowledge regarding hookah smoking between three separate categories of students' ages, a one-way analysis of variance (ANOVA) on participants' knowledge scores was conducted. Data analysis revealed a signi-ficant difference in age g r o u p s, F (2, 1 9 0) = 3. 3 2, p=0.04. Bonferroni Post Hoc tests were performed to ascertain which specific age group comparisons were significant. The participant age group, 20-21 years, scored significantly higher in mean knowledge of hookah than the 18 -19 year olds. (p=0.04) There were no significant differences in knowledge scores (p=.08) between the 18-19 year old and the 22 and older age groups. (Table VI)
To examine the differences in knowledge regarding hookah smoking between allied health and nursing majors versus all other majors and the differences in users versus non-users, two independent sample t-tests were per-formed. Results indicated that allied health and nursing majors scored significantly higher than non-allied health and nursing majors(t(198)=2.41,p=0.02) and hookah users had significantly higher knowledge scores as compared to non-users. (t(199)=2.09,p=0.04) Knowledge scores among majors and users versus non-users are shown in Table VII.
Discussion
Results from this study suggest that hookah smoking continues to be a growing trend among college-aged students, with over half of the respondents (68%) reporting that they felt hookah smoking was gaining popularity. Approximately one third (32%) stated that they had participated in hookah smoking in the previous 30 days. In comparison, a 2008 national study of college students found that 10% of the students surveyed reported using hookah in the last 30 days.4 While a direct comparison between the two studies cannot be made due to variations in sampling and the regions (national versus Midwest) surveyed, it can be inferred that hookah use among college students is increasing.
Previous studies indicate that hookah use is lower in the Midwest, the location of the university population surveyed in this study, when compared to other regions in the U.S.4, 5, 26, 27, 29 Griffiths and Ford found that 6% of Midwestern college students reporting hookah use within the past 30 days,2 however, 32% of respondents in this study reported smoking hookah in the last 30 days. In addition, this study takes place in a moderate-sized university town (population 40, 641), and despite the fact that there are no hookah bars within 100 miles, students are still participating in this form of tobacco use, with fewer than 6% reporting smoking hookah primarily in a hookah café or bar. (Table III) Results from this study suggest that the increased hookah use is not limited to larger cities where hookah cafés or bars are more common. Hookah smoking is common in social gatherings; 93% of the respondents stated that they were using hookah in the presence of more than one friend. Peer influence is also suggested to play a role in hookah use,26 and results from this study indicate that students are smoking in residences, and size of the town or proximity to hookah bars may not be a critical factor.
In this study, 68% of Caucasian students reported ever smoking hookah, compared to 70% of non-Caucasian students. Similar studies have found that students of Arabic decent living in the U.S. were more likely than non-Arab students to participate in hookah smoking.28 Demographic statistics in this study suggest that hookah use is accepted across different races, ethnicities, and cultures. Additionally, this study found that usage among Caucasian students was much higher than previously reported, indicating that the usage may be increasing on this group. Although there were not many Arab students to draw from for this study, the numbers of Caucasian and non-Caucasian users were very close, which may indicate that race may not be a significant factor. However, it is also noteworthy that the majority of students in this study were Caucasian, which may not give a comparative sample. In regards to gender, this study found that more males than females smoke hookah, supporting the findings of similar studies. However, this study also found that, overall, hookah use for both males and females was higher than other studies have previously reported and the results reflect findings suggesting that hookah smoking is gaining popularity 4-7, 26-29
Students in this study claimed to be familiar with the risks of hookah smoking but the majority of the respondents answered fewer than half of the questions (average score 4.4 out of 10) correctly indicating limited knowledge on the overall impact of hookah smoking on general and oral health. Allied health and nursing majors had higher scores (4.80) on the knowledge-based questions as compared to students with non-allied health and nursing majors (3.81). This may be due to the fact that allied health and nursing students have had more exposure to health-related courses in disease prevention as compared to students from other majors. However, even the allied health and nursing students answered less than half the questions correctly, which may indicate that they have not learned specifically about hookah usage in their programs. In addition, hookah users scored higher (4.70) than non-users (3.81) on the knowledge based questions. Nevertheless, they also answered less than half the questions correctly. Further studies could investigate the reasons why hookah users continue to smoke despite the known harmful effects of hookah use. Overall, the research indicates a need for education on the ill effects of hookah use across all demographics.
The very nature of hookah smoking process may be the reason students believe it is less harmful than cigarettes: roughly half of the respondents incorrectly indicated the belief that water filtered out the harmful ingredients, and half incorrectly believed that hookah smoking was less harmful because the tobacco is sweetened. Half of respondents also thought there was less smoke inhalation involved with hookah use, while in fact a person actually inhales 200 times the amount of smoke during a hookah session as compared to smoking a cigarette.7, 12 In general, long-term tobacco use has been linked to cardiovascular disease; however, in this study, nearly half (46%) of the hookah users were not aware of this risk. In comparison to other knowledge questions, respondents had the highest awareness (60%) that hookah smoking caused oral cancer. Another concern was that while most students reported smoking hookah in a group, only 44% of the respondents believed that secondhand smoke from hookah is considered a health risk. Not understanding the dangers of first and secondhand hookah smoke may also indicate that hookah users may not realize their increased risks for cancer, cardiovascular, respiratory and infectious diseases.
Many students in this study reported predicting that they do not plan to be smoking hookah in 5 years. Yet 63% reported an unawareness that hookah smoking is considered to be equally addictive as cigarettes.23 In addition, 49% of the respondents were unaware that hookah tobacco contains nicotine which leads to dependence by altering brain chemistry.9 In addition, previous research has identified that nicotine dependence resulting from hookah smoking, may encourage the transition to cigarette smoking.3, 20 An unawareness of these nicotine qualities indicates, that students may actually become addicted to hookah smoking habit or possibly move on to other forms of tobacco.3, 20
Respondents in this study reported first-time hookah use occurred between 14-21 years of age, (17.9 years average) thus indicating the need for hookah usage to be included in tobacco education programs beginning in middle school and continuing through high school. Additionally, hookah smoking education should be incorporated into the dental and dental hygiene curricula, as well as inclusion in continuing education programs for all related health professions. Dental professionals are encouraged to participate in community health fairs, school education, and in public policy sessions promoting legislation restricting hookah smoking.30 Future research should be conducted to assess dental hygienists' knowledge regarding hookah smoking as well as their ability and willingness to provide education on this important health issue.
There are a few noteworthy limitations to this study. This was a small convenience sample from a Midwest university and may not be generalizable to all college students across the U.S. The primary investigator recruited the participating professors and students, administered the survey and collected the data forms. Future studies should use an assistant or neutral party to conduct these aspects of the study. In addition, the survey knowledge questions and scoring were designed by the authors and were not validated.
Conclusion
Tobacco is the leading cause of preventable death worldwide and is related to 5 million deaths annually. While significant research has been conducted regarding the harmful effects of cigarette usage, hookah smoking has generated little study. Results from this study indicate that hookah usage is increasing in popularity among college students. Furthermore, this study indicates a significant knowledge gap regarding the health effects of hookah smoking across all demographics of college majors, including allied health and nursing. This knowledge gap supports the critical need for incorporating the harmful effects of hookah smoking into the curricula of future health care professionals, especially dental hygienists. Incorporating information on the detrimental health effects of hookah use is links well with the overall tobacco education provided by dental hygienists on a regular basis, with the goal of educating future generations of students to the harmful effects of tobacco use regardless of the delivery.
Footnotes
Trisha M. Krenik-Matejcek, RDH, MS is an assistant professor; Angela L. Monson, RDH, PhD is a professor; Brigette R. Cooper, RDH, MS is a professor; all in the Department of Dental Hygiene, Minnesota State University, Mankato, MN.
This manuscript supports the NDHRA priority area Client level: Oral health care (health promotion: treatments, behaviors, products).
- Received July 18, 2016.
- Accepted May 18, 2017.
- Copyright © 2017 The American Dental Hygienists’ Association





{kind=link}