



Abstract
Purpose The goal of this study was to analyze transcription of audio recordings to determine health topics that emerged from brief-motivational interviewing (MI) compared to traditional oral hygiene instructions (OHI).
Methods Fifty-eight periodontal maintenance patients were randomized to a brief-MI or traditional OHI group for a longitudinal 1-year clinical trial. Both groups received four patient education sessions per their assigned group. Audio recordings were transcribed and coded. The overarching themes and subthemes emerged were quantified and reported as the number of instances per participant. Global scores and behavioral counts were compared across baseline, 4, 8, and 12-month research visits using mixed-effect models.
Results Of the six overarching themes, the brief-MI group evoked more topics toward total health. Oral home care behaviors (15 vs 10.2) and oral diseases/conditions (3.3 vs 1.9) were discussed more in the brief-MI group compared to the traditional OHI group. This positive outcome for the average number of times a health topic was discussed in the brief-MI group compared to the traditional OHI group continued for the remaining major themes: lifestyle behaviors (1.0 vs 0.4), nutrition (2.6 vs 0.8), emotional/mental health (1.8 vs 0.8) and general health (1.2 vs 0.4).
Conclusion This study identified that brief-MI was a more successful communication approach to increase discussions of oral home care behaviors, oral diseases/conditions, lifestyle behaviors, nutrition, emotional/mental health and general health compared to traditional OHI in individuals with periodontitis.
- motivational interviewing
- brief motivational interviewing
- oral hygiene instructions
- patient education
- health behaviors
INTRODUCTION
Patient education and oral hygiene instructions (OHI) are an instrumental part of the dental hygiene process of care to assist an individual in achieving oral health. Historically, advice giving, known as traditional OHI is the most frequently used communication to provide patient education. However, advice giving is not supportive of patient autonomy or behavior change to improve an individual’s oral hygiene.1–3 Motivational interviewing (MI) is a patient-centered collaborative counseling approach to support positive behavior change.3 Motivational interviewing aligns with the Transtheoretical Model (TTM), also known as the Stages of Change, indicating advice-giving methods will not sustain long-term positive behaviors.3,4 This model acknowledges that most individuals are indecisive about changing a behavior, it does not occur quickly, and some relapse to prior negative behaviors.4
Motivational interviewing strengthens an individual’s intrinsic motivation and helps overcome ambivalence towards a positive behavior change.1,2,5–9 Due to time constraints in the dental setting, brief-MI is used to assess motives, raise awareness, and support a behavior change.2,7,8 In individuals with periodontitis, brief-MI has been noted in the literature as an effective communication approach to improve oral hygiene and reduce clinical outcomes of disease.1,2,5,9–11 However, periodontitis is a multifactorial inflammatory disease and biofilm removal alone may not be enough to improve periodontal health or prevent disease progression. This idea is well supported by the mixed clinical outcomes in the literature to support brief-MI as a superior communication approach compared to traditional OHI to improve periodontal health.1,2,5,9–11
There has been a shift in the evidence by a few researchers that clinical outcomes alone are not optimal to measure the effectiveness of brief-MI. Arnett and colleagues reported the importance of the patient-provider relationship to support oral health behavior changes.2 In another study, they expanded that patient-provider rapport is established by building on an individual’s self-efficacy.6 Tellez and colleagues stated clinical outcomes do not measure the individual’s self-efficacy for behavior change.12 In addition to self-efficacy and oral hygiene behaviors influencing indicators of periodontal disease, there is also an impact of the individuals’ systemic health,13 mental/emotional health,14–16 and lifestyle behaviors17 that contribute to the inflammatory process of periodontitis.
To the authors’ knowledge, there is no evidence to determine health topics that emerge from brief-MI compared to traditional OHI to support behaviors to improve periodontal health or identify contributing lifestyle behaviors that influence periodontal disease. The goal of this study was to analyze transcription of audio recordings from a 1-year examiner-blinded randomized clinical trial to determine health topics that emerged from brief-MI compared to traditional OHI. The identification of health topics evoked during brief-MI compared to traditional OHI may provide insight on the communication approach that is optimal to support oral health, general health, and wellness. This is relevant evidence needed for MI and brief-MI research that has not been explored. This study’s outcomes are anticipated to identify the communication approach that focuses on the patient’s needs and interests regarding their total health instead of an emphasis on clinical outcomes. The research question was, “What health topics emerge from BMI compared to traditional OHI in individuals with periodontitis?”
METHODS
Experimental Design
Tertiary outcomes from a randomized, examiner-blinded, 1-year longitudinal single site clinical trial from September 2018 – September 2020 were used to determine the health topics that emerged from brief-MI compared to traditional OHI in individuals with periodontitis by transcription of audio recordings. This study was approved by the University of Minnesota (UMN) Institutional Review Board (STUDY00003697) and registered on ClinicalTrials.gov (NCT03571958). Participants in both groups received a periodontal maintenance and patient education per their assigned group at four time points over a 1-year period at the UMN School of Dentistry (SOD) Oral Health Clinical Research Center (OHCRC). The patient education sessions were audio recorded for both groups. To provide individualized patient education for both groups and simulate clinical practice, no scripts or repeat education sessions were used in this study. The traditional OHI group received the “tell-show-do” communication approach specific to their plaque score, bleeding on probing (BOP), and gingival index (GI). The brief-MI group were asked two standardized open-ended questions to gauge their interest in their plaque score and ask permission to proceed with behavior change strategies customized to their interest to reduce their plaque score, BOP, and GI. The brief-MI intervention framework was adapted by the Motivational Interviewing Treatment Integrity (MITI) coding manual version 4.2.1.18
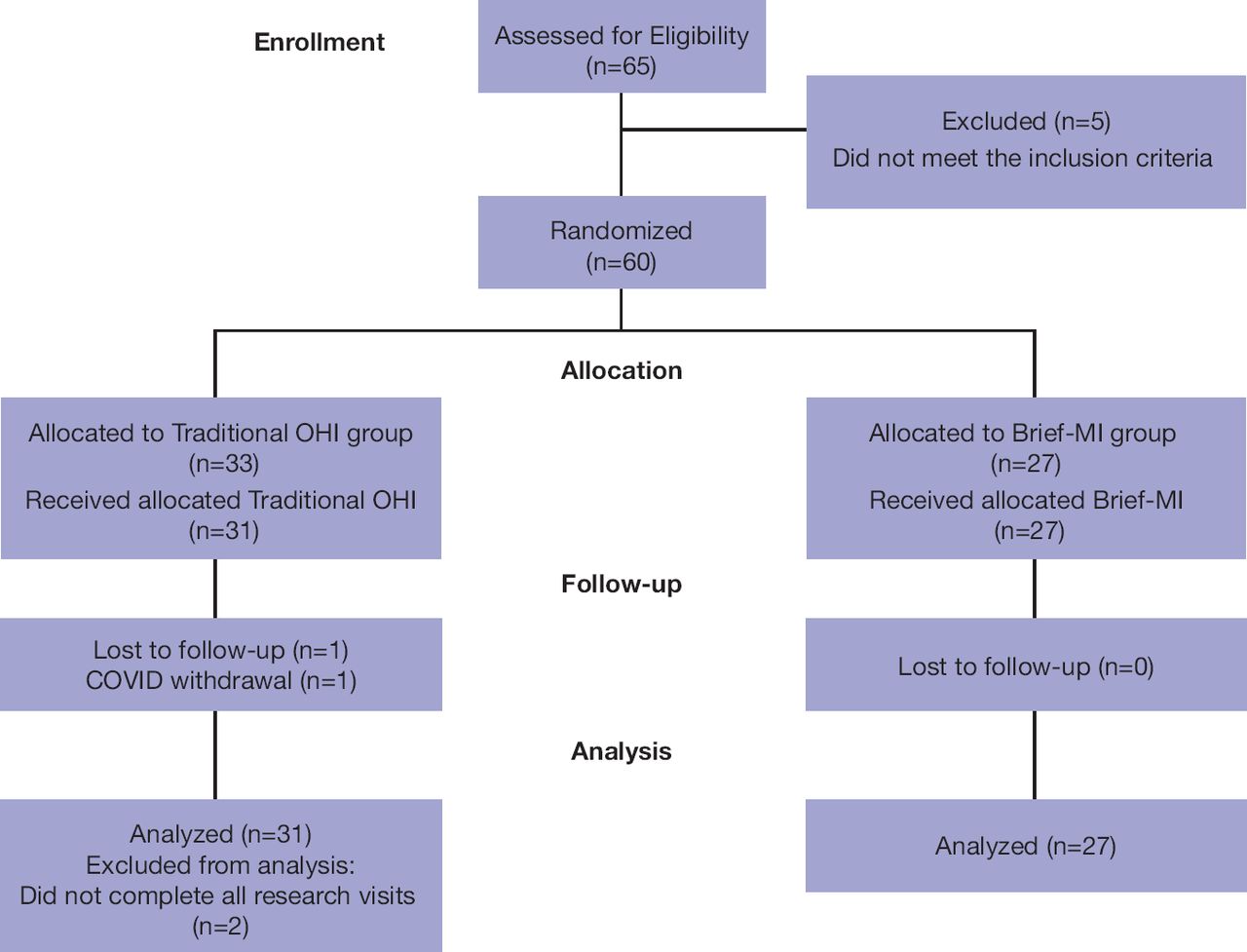
The principal investigator (PI) delivered patient education and completed the periodontal maintenances for both groups at four time points: baseline, 4-month, 8-month, and 12-month research visits over a 1-year period. The patient education sessions were approximately 6-12 minutes long and audio recorded with the PI and participant only. Incentives for participants to commit to four research visits over 1-year were: a no-charge periodontal maintenance and a prepaid parking pass at each study visit, a $50.00 gift card at the baseline, 4 and 8-month visits, and a $100.00 gift card at the 12-month visit. The participants had no prior relationship with the study team. All participants had the option to withdrawal at any time and were informed all patient education sessions were recorded. The PI was a female, master’s degree, licensed dental hygienist, educator, and researcher with extensive MI training from the University of Michigan (UM) SOD, UMN SOD, and had completed a 2-day training course with an MITI MI trainer; in addition to having a widespread MI teaching and research background. The characteristics and training of the PI were included in the Informed Consent Form for all participants. The protocol flow is provided in Figure I.

Protocol Flow
Sample Population
In the original clinical trial, a power analysis determined 60 participants, 30 per group, had an 80% power to detect an effect size of 0.74 using a two-group t-test at the 0.05 level of significance. Recruitment began in 2018 and included pre-screening of a dental software program (axiUm, Exan; Las Vegas, NV, USA) to identify candidates who met the inclusion criteria (Table I). Invitation letters were sent to individuals who met the inclusion and fliers were posted on each dental clinic floor of the UMN SOD. A convenience sample, consisting of 65 UMN SOD patients identified in the pre-screening process or volunteer candidates from the guided fliers who were in the periodontal maintenance phase of treatment and met the inclusion criteria of the clinical trial (Table I), was invited for an in-person screening visit. At the in-person screening visit, the PI completed the informed consent process. A total of five did not meet the inclusion criteria and the remaining 60 participants were enrolled and randomized using a statistical software program (SPSS; IBM, Armonk, NY, USA) to either the traditional OHI or brief-MI group (Figure I). All audio recordings from the original clinical trial of the PI and participants in both groups were included in this study.
Inclusion and exclusion criteria
MI Fidelity
The brief-MI intervention aligned with global scores and modified behavior counts to confirm MI fidelity of the PI.18 Global scores included: partnership; to understand change resides from the individual’s intrinsic motivation, empathy; to understand the individual’s ambivalence of change, change talk; to evoke the individual’s own ideas for behavior change, and sustain talk; to avoid reasons on not changing on a 5-point Likert-scale.18–20 Global scores measured the MI provider’s Spirit of MI.3 Behavior counts measured the number of times a MI-trained provider uses a specific brief-MI strategy.18,20 In this study, behavior counts were modified with permission to only include the MI guiding strategies of open questions, affirmations, reflections, and summaries (OARS), importance/confidence ruler, giving information with permission, and emphasizing autonomy.8,18,20–24
Two MI-trained licensed dental hygiene educators were calibrated MI-raters to confirm the PI’s MI fidelity in this study. The calibration included applying the clinical trial MI fidelity rubrics (global scores and behavior counts) to six UMN students MI Objective Structured Clinical Examination (OSCE) video recordings with a standard patient (SP) focusing on periodontal disease. The six student video recordings were reviewed and evaluated independently by each of the two MI-raters. Review of the clinical trial rubric evaluations were completed by the study team to determine discrepancies in global scores, or modified behavior counts. Revisions included operational definitions of the MI guiding strategies on the modified behavior count rubric. No changes were made to the global scores.
Outcome Measures
The recorded audios were transcribed for content analysis by one individual, the Associate Director and Manager of Survey Services at the UMN Office of Measurement Services (OMS). No field notes were provided to the transcriber. Data saturation was not discussed, and audio recordings were not provided to participants for comments or corrections. Approximately 31 hours of combined audio recording from the traditional OHI and brief-MI groups were transcribed for overarching themes and sub themes derived from data. A total of six overarching themes emerged: 1) oral home care behaviors, 2) oral diseases/conditions, 3) lifestyle behaviors (social and chemical), 4) nutrition, 5) emotional/mental health and 6) general health. The overarching themes were then transcribed to determine subthemes. The subthemes were as follows: 1) oral home care behaviors a) brushing, b) flossing, c) rinsing, d) interdental cleaning (water pik, proxy brush) and e) frequency of homecare behaviors (1-2x daily, 1-2x weekly). 2) Oral diseases/conditions a) caries, b) periodontal conditions (gingivitis and periodontitis), c) oral cancers, d) orthodontic care, and e) cosmetic dentistry (crowns, veneers, bleaching). 3) Lifestyle behaviors a) tobacco use (cigarettes, pipe, rolled tobacco, e-cigs, Juuls), b) marijuana/cannabis use, c) alcohol consumption, d) recreational drug use and e) occupational constraints impacting habits. 4) Nutrition a) diet, b) sugary acidic drinks (pop, sweeten coffee/tea), c) irregular eating habits (snacking, late night eating) and d) food choices. 5) Emotional/mental health a) stress (family, personal, or work stress), b) mental health conditions (self-reported diagnosed, undiagnosed or managed (i.e. depression, anxiety)), c) low self-efficacy (lack of self-esteem, lack of motivation). 6) General health a) cardiovascular health, b) obesity, c) pharmacological management (for any condition general health or mental health), d) sleep apnea, e) diabetes management, f) pulmonary conditions and g) other.
Global scores and behavior counts to measure the PI’s MI fidelity were also outcome variables.3,18,20 In this study, global scores measured the MI provider’s Spirit of MI and provided evidence of a quantified value on a 5-point Likert-scale to evoke health topics. The behavior counts were used to determine how many times and which MI strategies are the most useful to evoke health topics to support oral health, general health and wellness.
Data Analysis
Demographic characteristics were summarized using counts and rates or means (M) and standard deviations (SD). The overarching themes and subthemes were quantified on a per-group basis and reported as the mean number of instances per participant. Individual-level counts for themes and subthemes were not recorded so no statistical comparisons were performed. Brief-MI global scores18,20 on a 5-point Likert scale were compared across baseline, 4-month, 8-month, and 12-month research visits using linear mixed-effects models, with results reported as M with 95% confidence intervals. Brief-MI behavioral counts18,20 were modified with permission and were compared across visits using mixed-effects negative binomial models for count data and reported as M with 95% confidence intervals. Analyses were performed using R version 4.1.1.
RESULTS
Sixty participants were eligible and enrolled, 58 completed all study visits over the 1-year period for an attrition rate of only 3% (n=2). Figure I shows the participants enrolled and included in data analysis. The demographic information of the participants is provided in a prior publication.2 There was no significant difference in age, gender or ethnicity. The average age of participants was >60 years old and the majority of the participants were White males. The brief- MI group had an equal number of male and female participants (male n=14, female n=14), whereas there were more men compared to women (male n=20, female n=10) in the traditional OHI group.
Table II provides the average counts per overarching theme and subthemes. Of the six overarching themes, the brief-MI group was greater in the total number of times a specific major theme was discussed. Oral home care behaviors were discussed 15.0 times in the brief-MI group compared to 10.2 times in the traditional OHI group and oral diseases/conditions were discussed 3.3 times in the brief-MI group compared to 1.9 times in the traditional OHI group. This positive outcome for the increased average number of times a health topic was discussed per participant in the brief-MI group compared to the traditional OHI group continued for the remaining major themes: lifestyle behaviors (1.0 vs. 0.4 times), nutrition (2.6 vs. 0.8 times), emotional/mental health (1.8 vs. 0.8 times) and general health (1.2 vs. 0.4 times).
Average counts per participant for themes and subthemes‡
This positive trend for the brief-MI group was also identified in the subthemes that emerged. The most frequent average of subthemes that were discussed in the brief-MI group compared to the traditional OHI group were: oral home care behaviors, brushing (4.0 vs. 3.2), flossing (3.4 vs. 2.1), and rinsing (3.4 vs. 2.1 times); oral diseases/conditions, periodontal disease (2.4 vs. 1.5) and cosmetic dentistry (1.0 vs. 0.4 times); lifestyle behaviors, tobacco use (0.2 vs. 0 times); alcohol consumption (0.1 vs. 0 times); and occupational constraints impacting habits (0.7 vs. 0.2 times). The majority of subthemes for nutrition were discussed on average per participant more frequency in the brief-MI group compared to traditional OHI: diet (1.0 vs. 0.2 times), sugary acidic drinks (0.8 vs. 0.2 times), and irregular eating habits (0.3 vs. 0.1 times). For emotional/mental health, the most frequent subthemes on average per participant were stress (0.7 vs. 0.2 times) and mental health conditions (0.4 vs. 0.1 times). For general health, obesity (0.2 vs. 0 times), pharmacological management (0.3 vs. 0 time) and “other” (0.6 vs. 0.2 times) were most frequently discussed. The “other” subtheme in the general health overarching theme included, but was not limited to, topics such as neuropathy, brain injury, back pain, hip replacement, and difficulty sleeping.
Table III presents the results from a regression model (mixed-effects) as means with 95% confidence intervals of global scores and behavioral counts results. The average global scores on a 5-point Likert scale were high at baseline and gradually increased by the 12-month periodontal maintenance (partnership 4.14, 4.89; empathy 4.04, 4.68; change talk 4.00, 4.68; and sustain talk 4.36, 4.89). These results confirm the Spirit of MI was demonstrated by the PI. Statistical significance was achieved for partnership (0.0002), empathy (0.0005), change talk (0.0011) and sustain talk (0.0021) and suggest the reason for numerous themes and subthemes that emerged in the brief MI group compared to the traditional OHI group. The most frequent behavior count of MI strategies used by the PI overtime were affirmations (3.04, 3.82, 3.07, and 4.11) and reflective listening (3.52, 2.93, 3.04, and 3.50), followed by asking permission (2.66, 2.59, 2.24, and 2.34) and open questions (3.09, 3.20, 2.24, and 2.31). Summarizing was used 1.82 times at baseline and increased to 2.14 times at the 12-month periodontal maintenance. Statistical significance was achieved for open questions (0.04), and readiness ruler (<0.0001). These results highlight the most useful MI strategies to evoke health topics in patients with periodontitis are OARS.
Global Scores and Behavior Counts‡
DISCUSSION
Patient education and OHI are key interventions for periodontal therapy and an essential approach to ensure compliance over time. Historically, brief-MI research has focused on periodontal indicators of disease in the short-term and disregarded the complexity of individuals’ behaviors and contributing factors to obtain positive clinical outcomes. Periodontitis is a multifactorial inflammatory disease and raises the need for investigation to see if brief-MI taps into factors of oral health, general health, and well-being that may impact periodontal stability or the progression of the disease.
The theme for oral hygiene behaviors and oral diseases/conditions were the closest in ratio compared to other themes between groups. This is expected because traditional OHI focuses on improving oral hygiene behaviors to reduce oral diseases. However, discussing these topics more frequency does not measure if a behavior change will occur. Arnett and colleagues reported in the same group of participants, that brief-MI increased importance, interest, and self-efficacy of oral hygiene behaviors compared to traditional OHI.6 The evidence that brief-MI increases self-efficacy to move the patient through the TTM and ultimately to the maintenance stage for improved oral hygiene behavior to reduce periodontal disease indicators is promising.12,25–27 To determine if the increased frequency of discussing oral hygiene behaviors and oral diseases/conditions results in improved clinical outcomes, longitudinal research is needed.
It was not surprising that tobacco and alcohol use were frequently discussed in the brief-MI group compared to the traditional OHI. Motivational interviewing has been noted in the literature as a successful counseling approach dating back to the early 1980’s for addiction therapy and tobacco cessation.18 The alarming finding from this study was that tobacco and alcohol use were never discussed in the traditional OHI group. This demonstrates a major limitation of traditional OHI. These specific lifestyle behaviors may have never come up in the traditional OHI group because that approach to patient education focuses on oral hygiene only. Alternatively, traditional OHI advice-giving is not supportive or inclusive to allow the patient to share their lifestyle behaviors with a dental provider. Whereas brief-MI encompasses patient-provider rapport and trust in a non-judgmental demonstration to build a partnership that supports patients to share their lifestyle behaviors. Tobacco cessation is necessary for the management of periodontitis.28
Nutrition, specifically diet, was discussed more in the brief-MI group compared to the traditional OHI group. Many of the subthemes that emerged align more with caries prevention and not necessarily dietary counseling for the management of periodontitis. However, participants were more engaged and open to discussing their nutritional health in the brief-MI group. This may allow for nutritional counseling in the role of vitamins for the management and prevention of periodontitis. The inclusion of brief-MI to counsel periodontitis patients may bring awareness and motivation of nutrition to support periodontal health.
Emotional/mental health was discussed nearly double the amount of times in the brief-MI group compared to the traditional OHI group. The subthemes of stress and mental health conditions were discussed nearly triple the number of times compared to traditional OHI. Further, general health themes were also discussed nearly triple the number of times compared to traditional OHI. This provides evidence on the limitations of traditional OHI to support overall general health and wellness and promotes brief-MI as the optimal communication approach. This is critical evidence because dental hygienists are part of the comprehensive health care team and have the knowledge and skillset to educate patients and communicate with the health care team. It is well-known that many patients will frequently visit their dental home more often than a medical provider. This supports the important role of dental hygienists as health care team members to identify, educate and refer patients for systemic, emotional/mental health conditions, and lifestyle behaviors impacting their total health. This study is the first to identify that the application of brief-MI four times over a 1-year period evokes more total health discussions to promote oral health, general health, and well-being in patients with periodontitis.
Although individual-level counts were not collected to determine significance of themes or subthemes, this study filled a gap to determine health topics that emerged from brief-MI compared to traditional OHI discussions. Both groups’ discussions were focused on the participants’ plaque score, BOP, and GI and are reflected in the results for the theme of oral hygiene behaviors. Brief-MI allows for rapport, trust, and evocation of health topics that are most important to the patient. These findings are supported by the statistical significance of partnership and empathy of global scores. This study demonstrates the application of brief-MI for oral hygiene behaviors evokes the patient’s interests of health topics to support them in taking ownership of their own health to work toward total health. However, further research is needed to determine if the frequency of four brief-MI interventions result in a changed behavior toward total health measured with and without clinical outcomes. In addition to individual-level counts for themes and subthemes to determine statistical significance.
Another gap this study filled was the identification of which MI strategies are the most effective to use during a brief-MI session to evoke health topics. Open questions and affirmations were significantly used by the PI in this study. Further, reflective listening followed by summaries were the MI strategies most often used by the PI. For any provider to demonstrate these MI strategies, open questions are required. Therefore, the findings from this study indicated that the use of OARS are the most effective MI strategies during a brief-MI session at evoking health topics to support oral health, general health, and wellness in patients with periodontitis. The results of the most effective brief-MI strategies reported in this study, were also used in prior study with this same participant pool, to identify which strategies enhance interest, importance, and self-efficacy of oral hygiene behaviors.6 These results support prior evidence on the use of MI strategies for patients with periodontitis.1,2,5,6,9–11,23 It is noteworthy to acknowledge the chairside time for brief-MI compared to the traditional OHI group in this pool of participants that has beed reported in a prior study.2 The traditional OHI group averaged 6 minutes and brief-MI group averaged 9-12 minutes of patient education at each research visit.2 Despite the longer time for the brief-MI group, it is clear the collaborative counseling approach of brief-MI is the more successful communication approach.
Limitations and Future Research
Limitations include a sample of patients from a Midwest state dental school in the periodontal maintenance phase of treatment. The sample size and demographic characteristics of participants do not reflect the general population of periodontal patients in the United States (US). Individual-level counts for themes and subthemes were not recorded to determine statistical significance. Social determinants of health were not included as an outcome measure. Future research should include individual-level counts and investigate the themes identified in this study that are influenced by social determinant of health. Additionally, the literature is lacking identification of which oral health professional should be in charge of the mission to support behavior change through brief-MI interventions.2,9 Future research should investigate multiple MI-trained allied oral health providers compared to dentists, counselors, or psychologists to determine which health professional is the most effective at delivering brief-MI and who can achieve outcomes measured by self-efficacy and behavior change to positively influence oral health, general health, and well-being measured by patient reported outcomes.
CONCLUSION
This study identified that brief-MI was a more successful communication approach to increase discussions of oral home care behaviors, oral diseases/conditions, lifestyle behaviors, nutrition, emotional/mental health, and general health compared to traditional OHI in individuals with periodontitis. In this sample of participants, brief-MI raised awareness and evoked more topics of oral health, general health, and well-being compared to traditional OHI.
ACKNOWLEDGMENT
The authors would like to thank Professor Lisa Ahmann for her contributions to this study as a MI-rater.
Appendix 1: Global Scores Rubric‡
Footnotes
NDHRA priority area, Client level; Oral Health Care (health promotion: treatments, behaviors, products).
DISCLOSURES
This research was supported by the National Institutes of Health’s National Center for Advancing Translational Sciences, grant UL1TR002494. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health’s National Center for Advancing Translational Sciences.
This research was also funded by the Colgate CARE grant Contract #CON000000096101; Reference Award #A-2022-3509-OC.
The authors have no known conflict of interests associated with this research, and there was no financial support for this work that could have influenced its outcomes.
- Received April 26, 2023.
- Accepted August 20, 2023.
- Copyright © 2023 The American Dental Hygienists’ Association
This article is open access and may not be copied, distributed or modified without written permission from the American Dental Hygienists’ Association.





{kind=link}