



Abstract
Purpose: Accreditation standards require dental hygiene graduates to enter the profession with self-assessment skills and It is imperative for dental hygiene education to foster self-assessment skills throughout the curriculum. The purpose of this research was to evaluate the effect of self-assessment strategies on clinical competence in technical skill development and document student perspectives about the effects of participating in self-assessment activities.
Methods: All students enrolled in a pre-clinical course (n=50) attended a baseline lecture introducing self-assessment. Throughout the semester students performed self-assessment activities, which consisted of reviewing recordings of their hands while demonstrating instrumentation principles. Students used a self-assessment form to evaluate their performance and provide a plan to improve their self-identified deficiencies. Scores for all competency exams were analyzed using Chi-square tests to determine whether there was a significant relationship between self-assessment and clinical competency. Scores on the final competency evaluation were compared to those from the previous academic year (control group) using descriptive statistics. A qualitative survey including items about clinical performance, deficiencies, preparedness, ability to learn autonomously, self-confidence, critical thinking, and active engagement in learning, was distributed to students who successfully completed the course.
Results: Chi-square analysis determined no statistical significance (p =0.39) in the technical skill development between student groups that were (n=50) and were not exposed (n=56) to self-assessment strategies. A total of 21 participants (44%) completed the survey at the end of the course. Results revealed heightened self-awareness and confidence, enhanced skill development, the significance of self-assessment, increased student engagement, and the desire for instructor feedback.
Conclusion: While self-assessment did not impact clinical competency, it may be useful in fostering self-correction of instrumentation errors. Students felt participation in self-assessment activities helped to effectively evaluate their performance, improve skillset, increase engagement, and strengthen self-awareness, confidence, and critical thinking.
- dental hygiene education
- self-assessment
- clinical education
- clinical competency
- critical thinking
- active learning
Introduction
Dental hygienists are expected to enter the profession possessing the necessary skills to evaluate their performance and implement changes that will improve their clinical practices and patient care delivery. This concept is supported by the Commission on Dental Accreditation’s standard 2-21, “Graduates must be competent in the application of self-assessment skills to prepare them for life-long learning.”1 Dental hygiene education is responsible for meeting workforce demands, as well as accreditation standards. Implementing self-assessment activities in preclinical and clinical environments is proposed as a strategy to meet these requirements.
Self-assessment is defined as the process of developing an awareness of a personal learning experience. It is a best practice for actively engaging health science students in the learning process and develops the learner’s abilities to critically evaluate their clinical performance.2 The self-assessment learning process allows students to reflect on an experience and determine what actions should be taken to improve the outcome of the particular experience. The purpose of implementing this teaching strategy is to develop students’ critical thinking and problem-solving skill, ultimately leading to improved clinical performance.
The implementation of self-assessment strategies aligns itself with the long-established paradigm shift of active learning, transitioning from teacher-centered to student-centered environments, with the end goal of developing independent learners. Faculty members must still provide foundational information to ensure students have a clear understanding of concepts and skill criteria. However, in order for effective formative feedback to occur, learners need a strong working knowledge of task compliance, quality and the criteria used for evaluation.3 Once this is established, it then becomes the student’s responsibility to self-evaluate their performance, recognize whether or not they meet standards and criteria, and develop plans to address deficiencies.4-6 Learners are then engaged in the process of grasping the criteria for the clinical practices in their field and making effective decisions about their own skills.7
Literature suggests that higher-level thinking and complex learning must occur over time and be dialogic in nature.8 Students need to develop the ability to evaluate their own work and not be dependent on others.8 This can occur if higher education institutions foster students who have the ability to learn autonomously. Educators have been charged with developing and facilitating strategic plans to assist students in critically assessing their educational and life experiences.9
Dental hygiene educators are responsible for efficiently preparing students to possess self-assessment skills in order to maintain competency and quality assurance.1 To meet these demands, self-assessment strategies should be integrated into the dental hygiene curriculum, beginning with the first series of clinical courses. Learning how to evaluate one’s performance at an early stage is intended to assist students with identifying and improving weaknesses. Implementing self-assessment strategies in pre-clinical courses, followed by clinical courses, is logical given that learning is an evolving process. This methodology also provides learners with the opportunity to develop a realistic sense of their abilities.2 Additionally, if used as recommended as a means of formative assessment, students can use feedback provided to prepare for summative assessments.2 This is a crucial process, for students to become aware of their weaknesses. Additionally, learners will be able to enhance their familiarity with shortcomings and plans for improvement, thus applying theory to practice during clinic sessions. This awareness and practice can lead to improved performance.
Previous research has primarily focused on attitudes towards the self-assessment process, accuracy of self-assessment, the impact of self-assessment on ergonomics, and various methods of self-assessment.9-13 There is minimal research in dental hygiene education focusing on the association between the use of self-assessment strategies and clinical skill development. Furthermore, there is little research regarding students’ perspectives related to self-assessment activities. Investigating these correlations can be used to further develop teaching and learning opportunities in self-assessment. Placing greater emphasis on self-assessment activities within the education process can help develop future oral health care providers prepared to enter a workforce with the necessary skills to evaluate and improve their performance to ensure quality care. Understanding the impact self-assessment has on clinical skill development can assist dental hygiene educators incorporate or advance self-assessment strategies within the curriculum. Creating an educational environment that promotes critical thinking and problem-solving skills will position graduates for a positive transition from academia to the workforce. The purpose of this study was to evaluate the effectiveness of self-assessment strategies on clinical competence in technical skill development in a pre-clinical dental hygiene course and document student perspectives regarding the effects of participating in self-assessment activities.
Methods
The Institutional Review Board of Farmingdale State College approved this mixed methods study. Purposive and convenience sampling was used to select the study sample. The study population consisted of dental hygiene students enrolled in a pre-clinical course. This was the first course of a series of clinical courses required for graduation from the program as well as for certification to register and take the national board licensing examination. Students were invited to participate in the quantitative portion of the study by word of mouth on the first day of class during orientation and were provided with the research consent form, detailing the study. All students chose to participate in the study.
All students (n=50) attended a baseline lecture on self-assessment held during the course orientation and were required to participate in self-assessment sessions four times over the course of the semester. Self-assessment sessions consisted of videos, completion of a criteria-based rubric, and a faculty-student review and feedback. To ensure anonymity, only students’ hands were videotaped during instrumentation practice sessions. These sessions took place prior to the three competency exams and the comprehensive clinical final exam. Using a self-assessment form consisting of skill descriptors, students self-assessed their performance as either satisfactory or needs improvement in the application of the principles of instrumentation demonstrated in the recorded videos. Students then described their skill demonstration and plans for improvement to a faculty member to confirm accuracy.
Scores for the three competencies and final exam were analyzed using descriptive statistics. Chi-square tests were used to determine significant relationships between self-assessment and clinical competency. Scores on the clinical final exam were evaluated for successful learning outcomes as compared to percent distribution of scores from the control group (n=56), consisting of students from the previous academic year. Chi-square analysis on competency exams I, II, and III were also evaluated for successful learning outcomes between groups.
While the four self-assessments, three competency test scores, and the final exam were a required part of the course, participation in the research study was optional and did not have an impact on students’ standing. The informed consent forms were collected in an envelope, which were not opened until after the final course grades had been submitted. Ensuring confidentiality, participant information was de-identified at the point of collection. This also satisfied any concerns regarding coercion.
A qualitative survey assessing student perceptions regarding self-assessment was developed and administered via an online software program (SurveyMethods; Capterra Inc, Arlington, VA, USA) following completion of the pre-clinical course. Students were invited to complete the survey by means of an electronic mail containing a recruitment cover letter and a customized link containing the research consent form and study details, followed by the survey.
No identifying information was collected to maintain the anonymity and confidentiality. After the initial launch of the survey, two follow up emails were sent to non-responders to increase the response rate.
Concepts and theories that were detailed throughout the literature guided the development of survey questions. The survey consisted of seven open-ended questions assessing how participation in self-assessment activities affected students’ abilities to identify clinical strengths and weaknesses, improve deficiencies, evaluate their performance, prepare for competencies, and learn autonomously. Students’ self-confidence, critical thinking, and active engagement in the learning process as a result of self-assessment were also analyzed. Data were analyzed and coded through organization into categories. The process of coding was used to develop themes and patterns. Data theme identification techniques were performed manually.
Results
Quantitative Results
Fifty students performed self-assessment strategies four times throughout the semester prior to completing three pre-clinical instrumentation competencies and a final exam comprised the experimental group (n=50). Fifty-six students from the previous academic year, who had not been exposed to self-assessment strategies, comprised the control group (n=56).
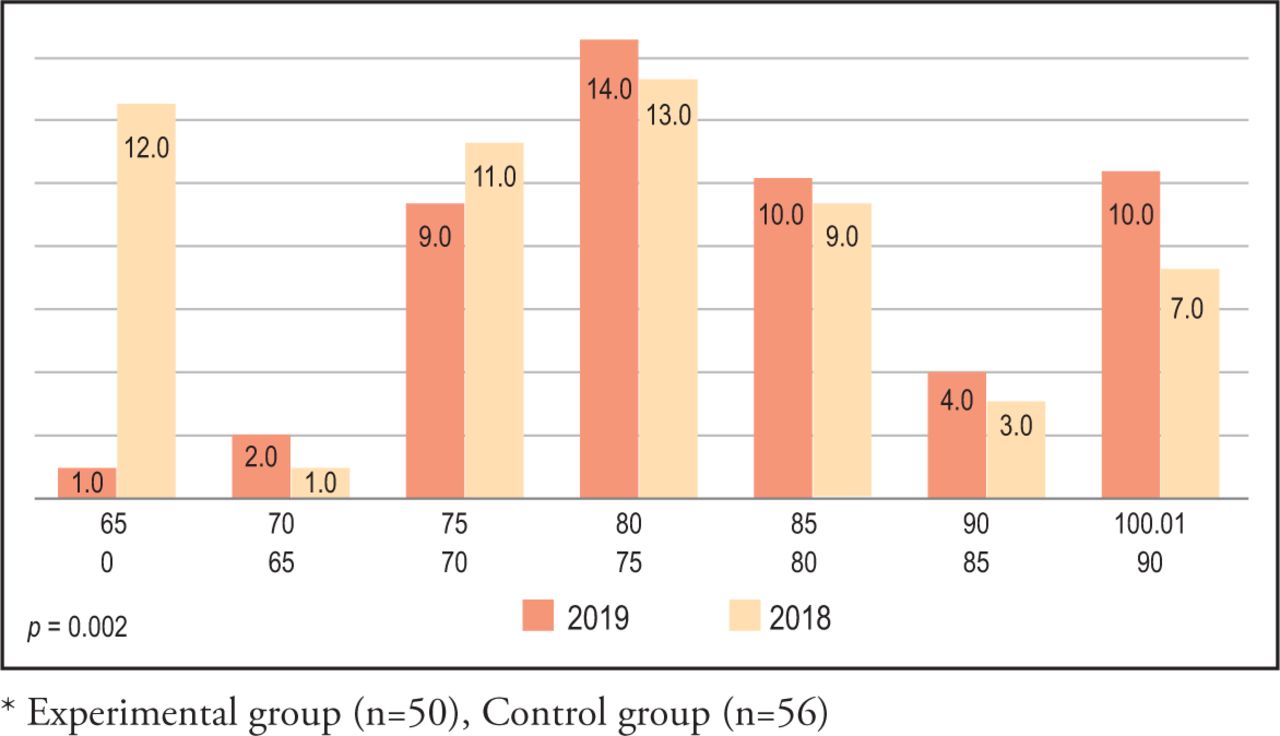
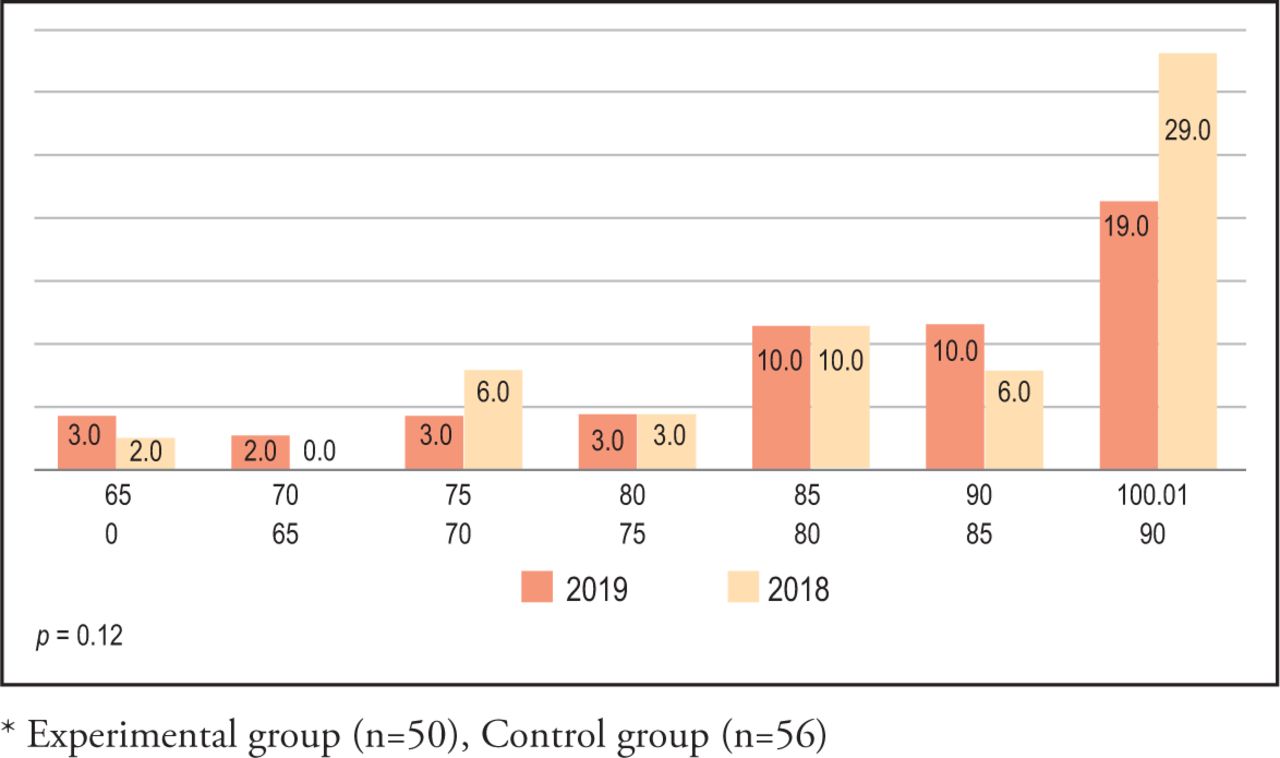
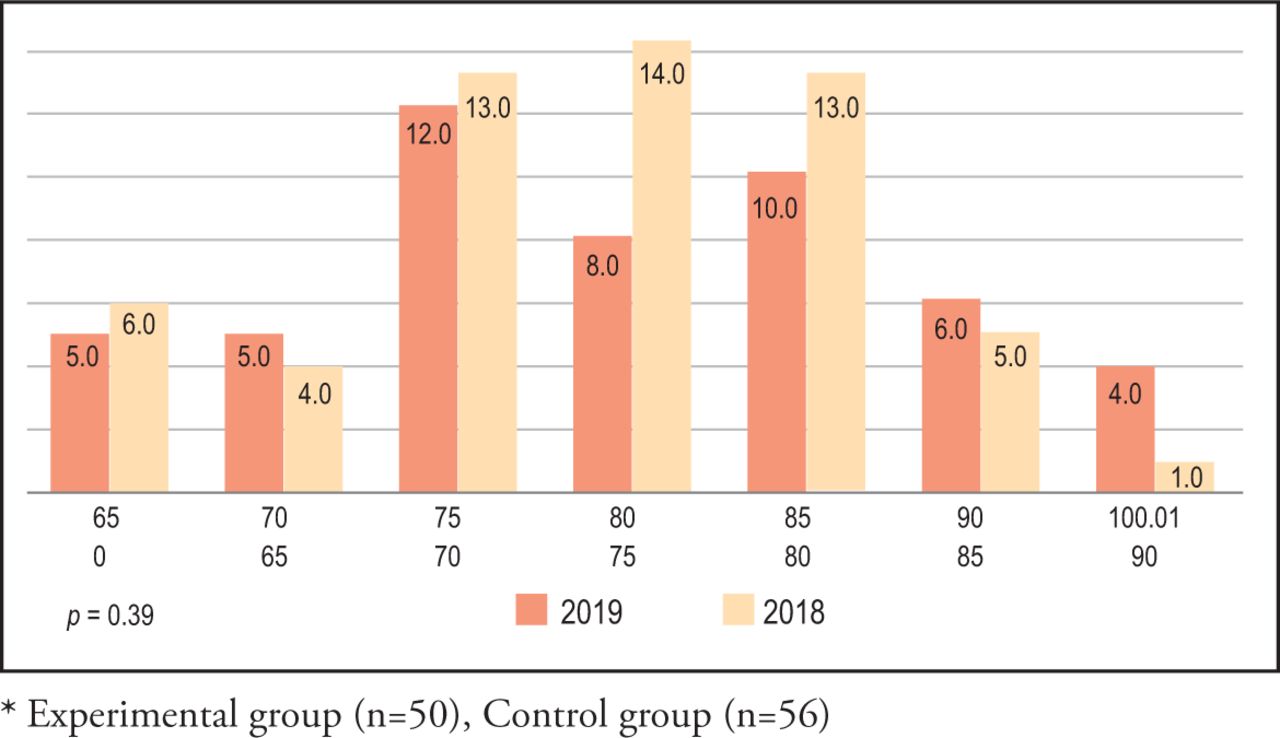
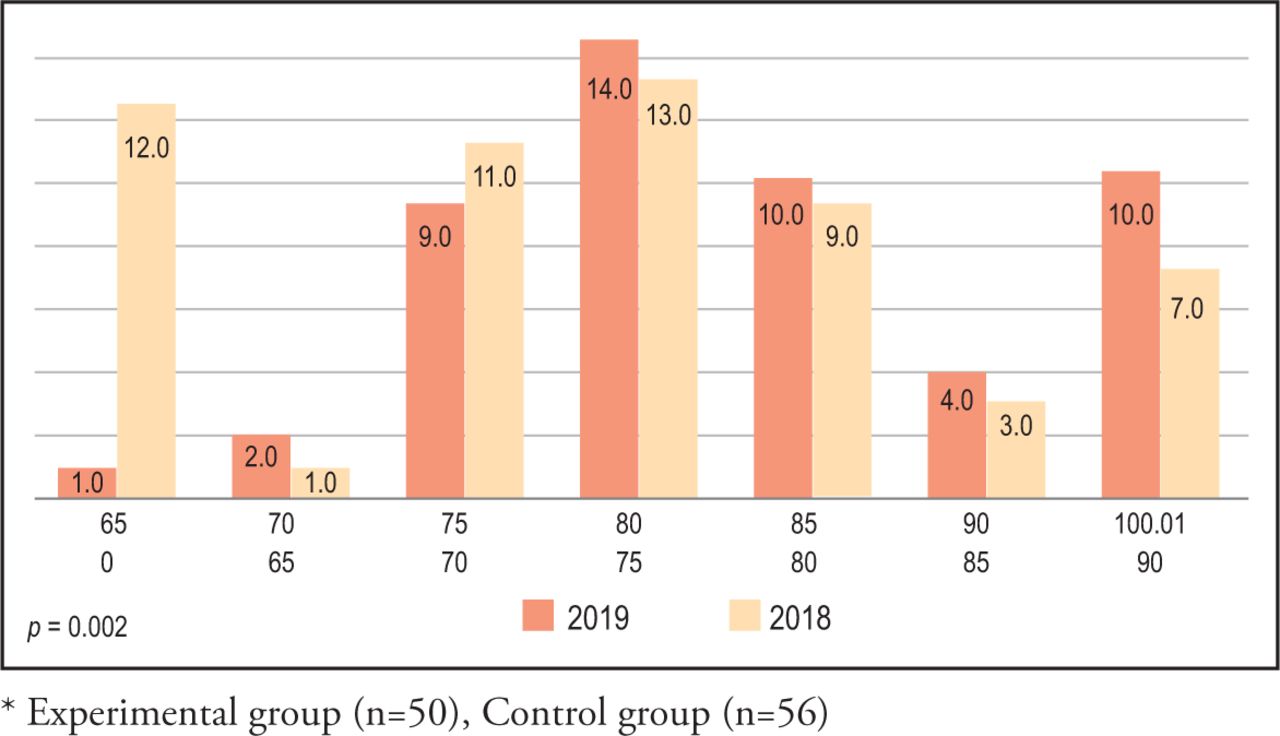
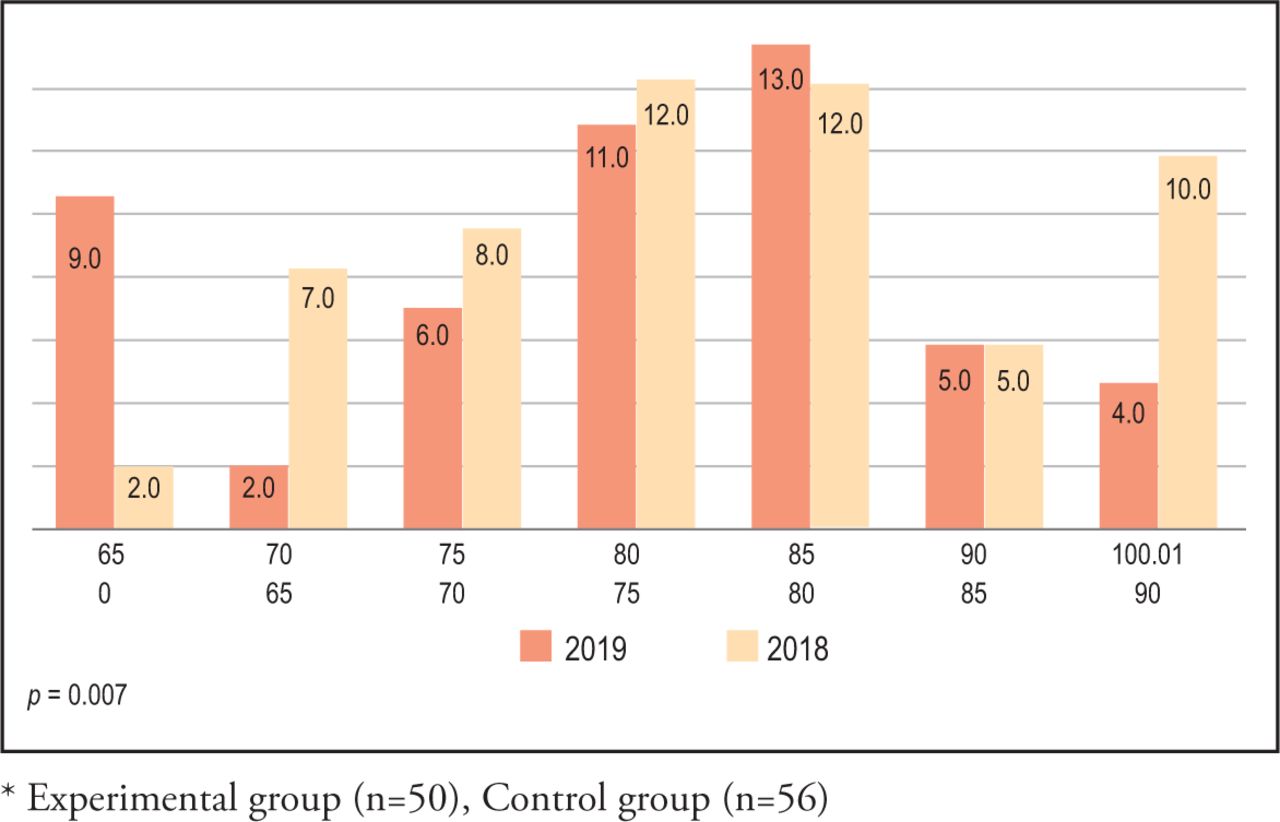
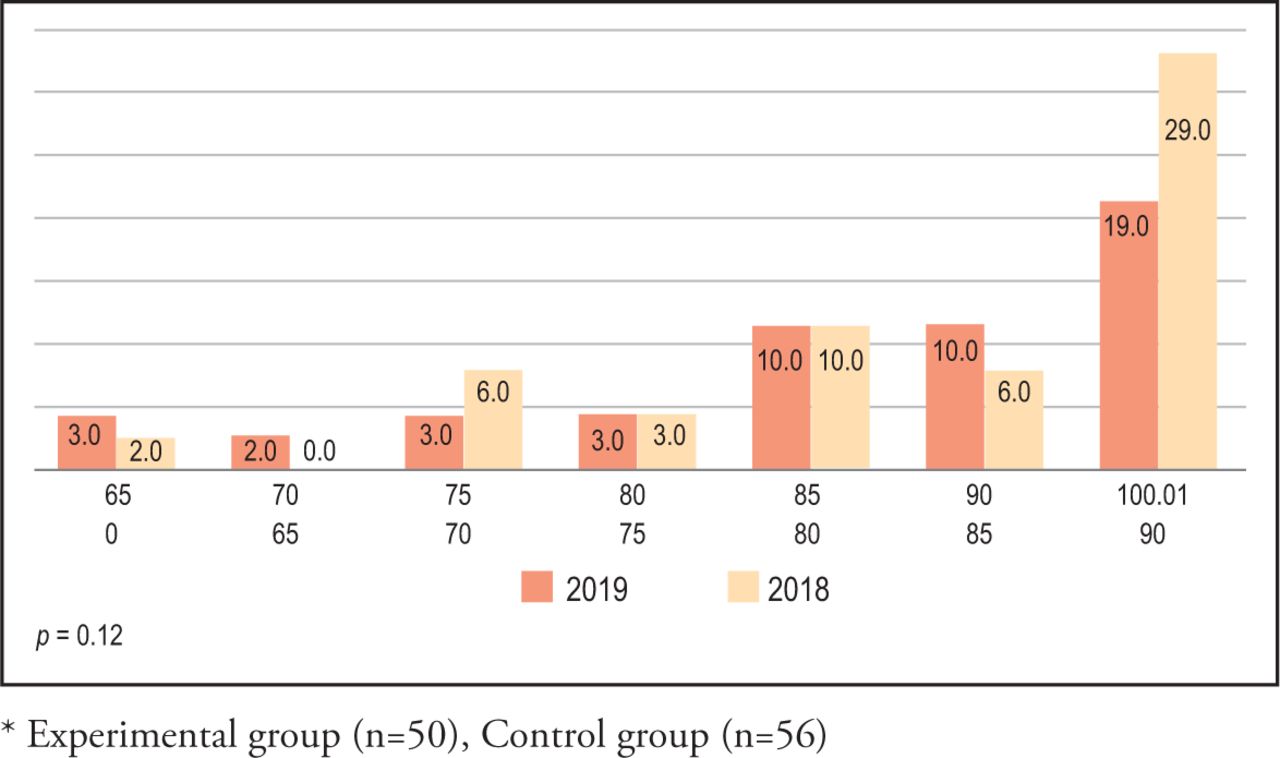
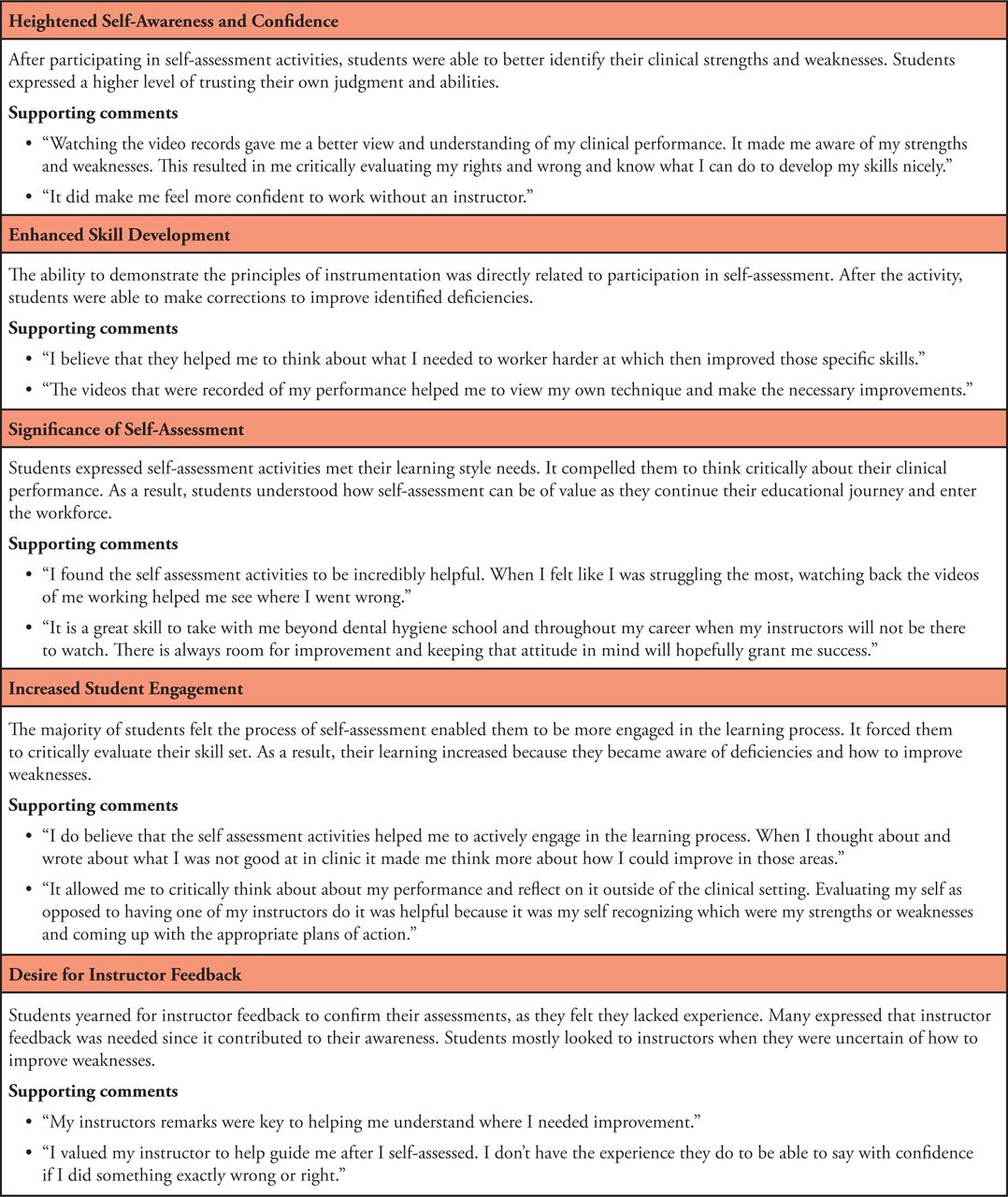
Chi-square analysis determined no statistical significance (p=0.39) in the technical skill development on the comprehensive final exam outcome scores between the experimental (n=50) and the control (n=56) groups (Figure 1). Competency exam I assessed students’ technical skill while performing the principles of instrumentation using a universal curette. Chi-square tests indicated a significant difference (p=0.002) between the experimental and control groups; the experimental group demonstrated higher successful learning outcomes on the use of the universal curette (Figure 2). Competency exams II and III assessed students’ technical skill while performing the principles of instrumentation using the Gracey 15/16 and Gracey 17/18 curettes, respectively. Chi-square tests revealed a significant difference (p=0.007) between the two groups. The control group without self-assessment strategies demonstrated higher successful learning outcome on competency exam II (Figure 3), indicating that self-assessment did not have any impact on competency development on the use of the Gracey 15/16 curette. Findings on Chi-square test for competency exam III revealed no significant difference (p=0.12) in the technical skill development between the groups on the use of the Gracey 17/18 curette (Figure 4).

Chi square analysis of final exam results*
* Experimental group (n=50), Control group (n=56)
Chi square analysis of competency exam I*
* Experimental group (n=50), Control group (n=56)

Chi square analysis of competency exam II*
* Experimental group (n=50), Control group (n=56)
Chi square analysis of competency exam III*
* Experimental group (n=50), Control group (n=56)
The final was a comprehensive clinic exam evaluating students’ technical skill development in performing the principles of instrumentation using all the calculus removal instruments within their cassettes. A passing grade of C or better was used to determine competency. Data indicated that there were no differences in skill levels between the groups. A majority (78%, n=50) of the experimental group were competent on the final exam, which was identical to the 78% of the control group (n=56).
Qualitative Results
All participants who successfully completed the course (n=48) were invited to take the survey with a response rate of 44% (n=21). Overall, respondents articulated sentiments of approval towards self-assessment. The following themes emerged from the qualitative data analysis: heightened self-awareness and confidence, enhanced skill development, the significance of self-assessment, increased student engagement, and the desire for instructor feedback. Participant perspectives for each theme are shown in Figure 5.
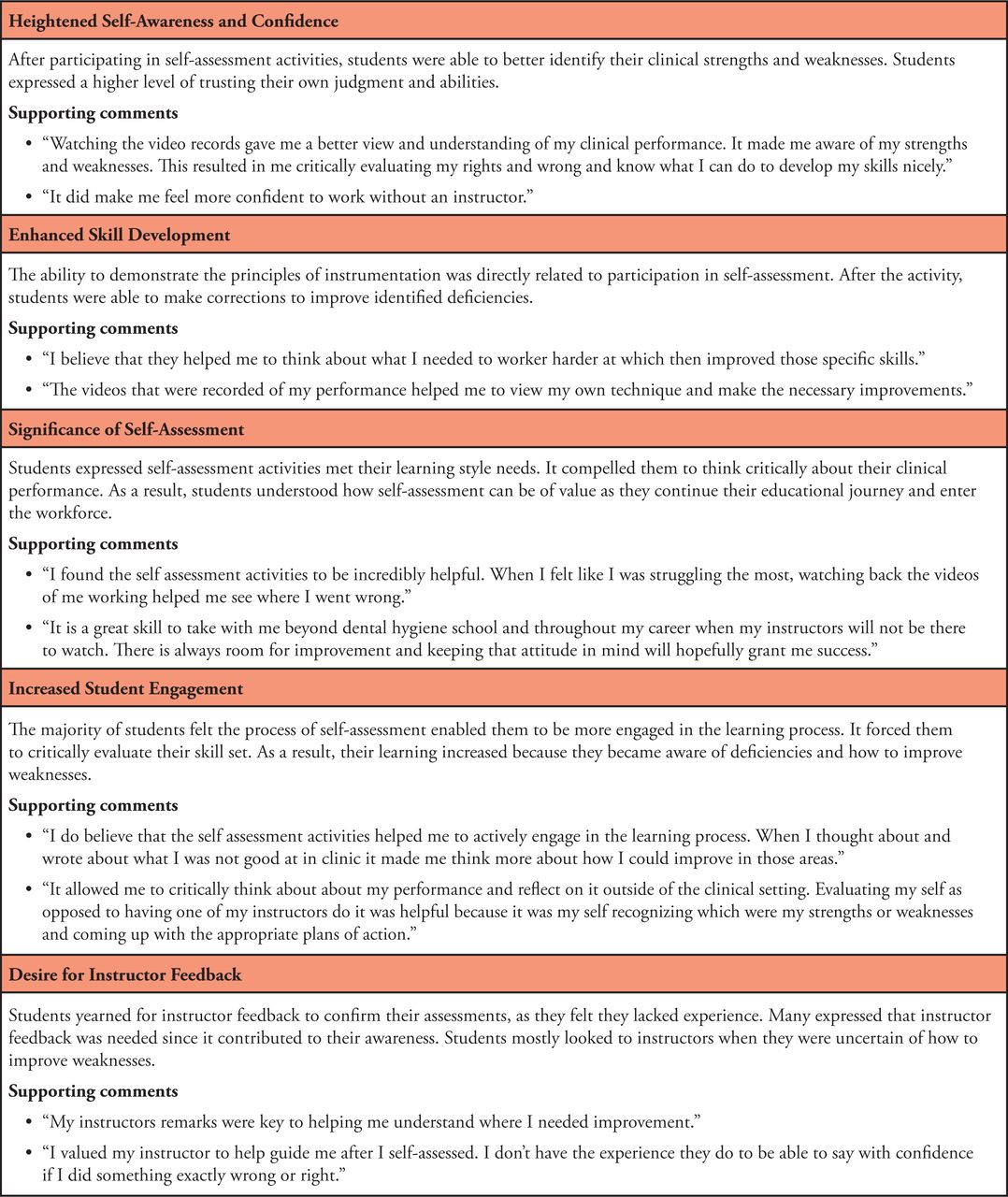
Emergent themes linked to participant perspectives (n=21)
Discussion
Clinical competence in dental hygiene education can be enhanced by the early development of an awareness of personal learning while promoting student engagement in the learning process. This can be realized by implementing self-assessment skills to foster higher-order thinking and problem-solving skills. Review of the literature demonstrates that self-assessment is utilized in varying levels of preclinical and clinical dental and dental hygiene education.2 Research findings also indicate that teaching self-assessment strategies, establishing consistent opportunities for students to self-assess, along with the addition of faculty feedback, provides students with multiple chances to improve their self-evaluation throughout the undergraduate curriculum.5 The addition of reflection within self-assessment seems to promote the development of critical self-reflective skills.5
In this study, self-assessment strategies in the preclinical dental hygiene course did not promote a significant difference in student learning outcomes in the technical skill development of the participants. However, it can be inferred from this investigation that student reflection and positive perceptions regarding the process were a beneficial outcome in providing a foundation for self-assessment measures to continue across the curriculum. In a national study of dental hygiene program directors, most (85%, n=125) most supported the utilization of self-assessment to evaluate clinical competence.14
Although the final competency exam scores in the current study did not demonstrate a significant difference between the experimental and the control groups, the participant voices on self-assessment days echoed their realization of a palpable “a-ha” moment in recognizing their errors when reviewing the videos. It was noticeable during these clinical sessions that students were receptive to the self-assessment strategies, and the visual aid of video recordings provided an opportunity to actually visualize their technique and see where improvement was needed. Students’ positive attitude of the use of self-assessment videos in their clinical experience underscores findings from parallel research demonstrating that the addition of instructional videos enhances the acquisition of psychomotor skills.15
Limitations of this study included general time constraints and calibrating students on how to self-assess. Although all students in the experimental group were exposed to a baseline lecture detailing the accreditation standard on self-assessment, the study design did not allow for adequate time to teach students “how” to self-assess. Time did not allow for teaching students the dynamic intricacies of how to self-assess. A systematic review of the literature of self-assessment in dental education supports the concept that providing students with the appropriate training to critically evaluate and differentiate between correct and erroneous technique could increase students’ potential in their ability to self-asses.2 The recording of student instrumentation videos was restricted to the two principal investigators only and did not include all faculty members in the pre-clinical course. Expanding the ability to make recordings would have provided more access to demonstrations of student skills.
Future research could include studies with a focus on evaluating the differences between student self-assessments versus faculty assessments of principles of instrumentation. Additionally, implementing a baseline tutorial on what a student should be looking for in a self-assessment of instrumentation principles would be beneficial to investigate. Studying the effects of self-assessment with increased faculty helping students understand how to critically evaluate their performance may yield different findings because of more time spent on active, student-centered learning activities. A long-term evaluation could incorporate an annual survey on student perspectives of the self-assessment measures implemented throughout their clinical courses.
Conclusion
While self-assessment did not impact clinical competency in this study, it may have been useful in fostering participants’ self-correction of instrumentation errors. Investigator observations of student attitudes during self-assessment included an increase in students’ abilities to recognize the application of the principles of instrumentation. Participants perceived self-assessment as a method to effectively evaluate clinical performance, improve skillset, increase engagement, and enhance self-awareness, confidence, and critical thinking. Perspectives from this study demonstrate the value of exposing students to self-assessment strategies early on in the curriculum.
Acknowledgements
This research study was funded by the Theresa Patnode Santmann Fund for Faculty Development. The authors would like to thank Douglas E. Johnston, PhD for his assistance with the statistical analysis.
Footnotes
This manuscript supports the NDHRA priority area, Professional development: Education (educational models).
- Received March 22, 2021.
- Accepted July 19, 2021.
- Copyright © 2022 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}