



Abstract
Purpose: Dental caries is a non-communicable, preventable disease that disproportionately affects low-income children in the United States (US). The purpose of this systematic review was to describe oral health education and promotion activities designed to prevent early childhood caries (ECC) provided by Early Head Start (EHS) programs in the United States.
Methods: Five databases were searched including CINAHL, Dentistry & Oral Sciences Source through EBSCO, PubMed, Google Scholar, and the Wiley Online Library, to identify peer-reviewed quantitative studies published in English on oral health education and promotion activities within EHS programs from 2000 to 2019. Studies were assessed for eligibility using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram (PRISMA). Two researchers independently evaluated the included studies.
Results: The initial search yielded a total of 363 articles. Following the screening process, five studies met the inclusion criteria (observational, n=2; quasi-experimental, n=3). The main outcome measures included oral health knowledge, attitudes and behaviors, oral health education, oral health promotion, and oral health activities. Three studies investigated the effectiveness of oral health education and promotion interventions among EHS staff and parents. Two studies examined oral health activities such as education, toothbrushing instructions, toothpaste use, dietary education, and dental assessment.
Conclusion: Studies that focused on increasing pediatric oral health knowledge and practice behaviors among both EHS staff members and parents reflected positive outcomes. Ongoing research is needed to examine the effectiveness of oral health education and promotion activities as they relate to the oral health outcomes of children enrolled in EHS programs.
Introduction
Early childhood education programs in the United States (US) are supported with grants and services, such as educational planning, development, evaluation, and quality assurance from the US Department of Education in partnership with the US Department of Health and Human Services.1 Early childhood prevention programs, such as Head Start (HS), Early Head Start (EHS), Women, Infants, and Children (WIC), and home visiting provide a variety of oral health promotion and education activities for families and children, and provide assistance in navigating health and dental services.2,3 In addition, HS/EHS programs introduce children to school through the implementation of a goal oriented approach to enhance positive outcomes for children and families.4 Head Start programs are federally funded and provide education, health, and family well-being services for low-income children age 4 to 5 years.5 Children from birth to age 3 years and pregnant women from low-income families are served by EHS programs.6 In the year 2000, there were 1700 HS/EHS programs that provided services via the HS center-base, home-base, or family child care model.5
Oral health policies and standards for the HS/EHS programs are provided through the US Department of Health and Human Services, Office of Head Start, with the assistance of partnerships from professional oral health organizations.6 Oral health performance standards include regulations related to tooth brushing, feeding practices, fluoride use, first dental visit, and oral health education and promotion activities.6 In 2018-2019, a total of 166,693 children were enrolled in EHS programs across the US.7 Data collected from an inner-city childcare center in New York (2004-2006) showed that 43% of the children enrolled in EHS (n=162) had at least one carious lesion.8 Further, data collected during 2011-2014 showed that 9.14% of children in the US aged 0-5 years had untreated dental caries.9 In general, children enrolled in EHS programs8 and those from families with parental poverty and low health literacy, tend to have a higher risk for dental caries.10
Dental caries is a preventable disease that disproportionately affects low-income children.10,11 Specifically, early childhood caries (ECC) involves children <6 years old with a dental caries experience.11 Organizations such as the American Academy of Pediatrics (AAP), American Academy of Pediatric Dentistry (AAPD), American Dental Association (ADA), and American Dental Hygienists’ Association (ADHA) emphasize the importance of oral health education to improve oral health status and overall quality of life for children.12-15 It is important to understand the oral health education and promotion activities EHS programs are implementing resulting from the recommended oral health standards. Examples of oral health education may include incorporating learning activities within the classroom and providing oral health information to parents and caregivers. Oral health promotion activities may include integrating toothbrushing and dental screenings within EHS programs.6 Early Head Start staff members have been shown to value children’s oral health and exhibit interest in providing learning activities; however, inadequate oral health knowledge has been shown to minimize their confidence to develop preventive activities.16,17 The purpose of this systematic review was to address the question, “What oral health education and promotion activities are performed in EHS programs for staff, children, and caregivers in the United States?”
Methods
Search strategy
An initial search was conducted February 2019 by the primary investigator using five data bases: CINAHL Plus with Full Text, Dentistry & Oral Sciences Source through EBSCO, Medline through PubMed, Google Scholar, and the Wiley Online Library. Various combinations of keywords were used in the search. Search terms included: [oral health OR dental health OR oral hygiene OR dental hygiene AND education OR promotion OR activities OR tooth brushing AND Early Head Start AND Early Childhood Caries OR dental caries OR tooth decay OR cavities]. Other keywords included specific oral health activities for children, among them: “mouth cleaning, fluoride use, bottle use, first dental visit, and dental referral.” The specific population reference words included: “staff, directors, children, and parents.” Once the database search was completed, an individual search was performed utilizing the reference lists of the included studies. After the search was conducted, a second investigator screened the list of search terms and article returns based on the research question. A reference management software program (Mendeley version 1.19.3; London, UK) was used to identify duplicates, and to organize abstracts.
Eligibility criteria
Inclusion criteria for the systematic review were quantitative peer-reviewed experimental and observational studies, conducted in the US, and written in English between 2000-2019. Specifically, studies that examined oral health activities, oral health education, and oral health promotion in Early Head Start programs were included in the search strategy. Studies were excluded if they were qualitative, letters to the editor, case reports, personal communications, or narrative reviews.
Study selection
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart was used for the systematic review.18 In the first step, duplicate studies were removed, and the remaining studies were screened by titles and abstracts independently by the primary and secondary reviewers. Second, full text articles were assessed for eligibility. Lastly, articles that met the inclusion criteria were reviewed by the primary reviewer followed by the second reviewer.
Risk of bias in individual studies
The quality of included studies was assessed by two reviewers, who independently evaluated the quality of studies using the Effective Public Health Practice Project’s Quality Assessment Tool.19 The tool consists of eight components that evaluate selection bias, study design, confounding variables, blinding, data collection methods, withdrawals and dropouts, intervention integrity, and analyses.19 Each of the eight components have questions with multiple choice answers that are scored according to a specific criteria and described as good, fair, or poor. Next, an overall global rating was developed for each component to include strong, moderate, and weak. At the end of the article review, a rating was determined for the overall quality of the study. Rating criteria were strong (the article received no weak ratings), moderate (one weak rating), or weak (two or more weak ratings). If there was a discrepancy with an article rating due to an oversight or differences in interpretation of criteria, the reviewers discussed the article to reach a consensus. The five articles were summarized according to the author and year, study location, research design, population, outcome measure, and significant results.
Results
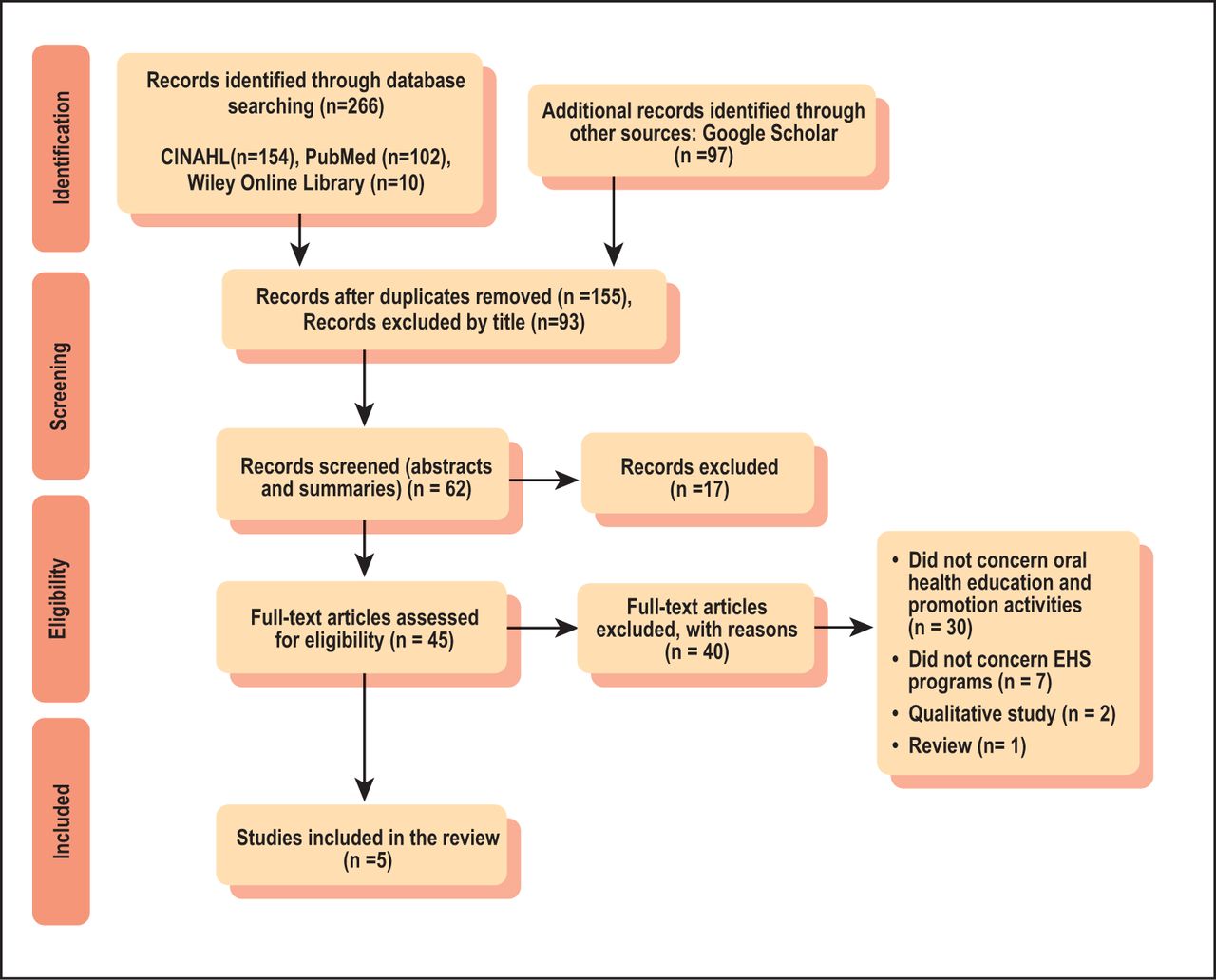
A total of 363 search results were obtained from the electronic database search. After duplicates were removed, 155 articles remained and of those, 93 were excluded based on the titles, 17 were excluded after screening the abstracts. The remaining 45 articles were included in full-text screenings; of these, 40 were removed based on the exclusion criteria. A total of five articles met the inclusion criteria for this review. Ratings for the five articles were as follows: high (n=1), moderate (n=3) and weak (n=1). The PRISMA flow-chart is shown in Figure 1.

Four-phase preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow-chart of identified articles18 (n=266)
Study characteristics
The five articles included were observational studies (cross-sectional, n=2; quasi-experimental n=3). Two studies were conducted in North Carolina, one in New York, one on the Hawaiian island of O’ahu, and one in Wisconsin. Study participants included EHS directors, teachers, and health coordinators (n= 485),17 Migrant and Migrant Seasonal Head Start Program (MSHS) staff (n=401),20 and EHS staff members who interacted directly with children and parents (n=71),21 parents of children enrolled in EHS programs (n= 91),23 and EHS home visitors (n=118).22 Outcome measures used within the five studies included: oral health knowledge and attitudes, oral health activities, self-efficacy, readiness to perform oral health promotion, and promotion of dental care use. For this systematic review, the outcome measures were organized into three categories: oral health knowledge, oral health promotion, and oral health activities. A summary of the included studies is shown in Table I.
Summary and characteristics of included studies (n=5)
Oral health knowledge
Glatt et al.,22 Kranz et al.,17,20 and Wilson et al.23 examined oral health knowledge of EHS home visitors, parents, and staff members (program directors, teachers, and health coordinators) using self-administered questionnaires. Two of these studies used interventions, educational videos and motivational interviewing, with the aim to increase knowledge of the participants.22,23 Glatt et al. demonstrated improvement in oral health knowledge of EHS staff members,22 while Kranz et al. noted a gap in the oral health knowledge of EHS teachers.17,20 Wilson et al. revealed improved knowledge among parents after receiving oral health education videos intervention, as demonstrated by increased correct answers from baseline (72%) to posttest (81%).23
Glatt et al. focused on home visitors (n=118) who received a 3 hour educational session including a video that provided motivational interviewing techniques.22 The short-term impacts of the intervention increased home visitors’ oral health knowledge by 7-29% on 5 out of 14 questions (p<0.05).22 Kranz et al. examined pediatric oral health knowledge and activities of EHS staff members (e.g. directors, teachers, and health coordinators) in two studies.17,20 A dental visit for children by age one is emphasized by the Head Start Early Childhood Learning and Knowledge resource center.24 However, 47.69% of EHS teachers (n=260) reported knowing about the recommended dental visit by age one compared to 61.11% of EHS program directors (n=18), and over 50% of health coordinators (n=18).17 Over 80% of EHS teachers reported knowing that low-income children have an increased risk for tooth decay.17 Kranz et al. (2012) compared oral health knowledge and activities of EHS and Migrant and Seasonal Head Start (MSHS) programs staff members.20 Of these, 79.6% of EHS teachers (n=329) and 70.8% of MSHS teachers (n=72) reported knowing that low-income children have an increased risk for tooth decay.20
Unlike the previous studies that focused on EHS staff members, Wilson et al. focused on the oral health knowledge of parents (n=91).23 The researchers used two intervention approaches and randomly assigned parents and caregivers to one or two video groups: didactic in a lecture format or family-centered in a personal interview format.23 Participants’ overall mean oral health knowledge score increased significantly by 1.79 points (before intervention M=15.19, SD=3.43; after intervention M=16.98, SD=3.42).23 However, there was no statistically significant difference between the groups in post-test knowledge scores based on the type of video received (didactic versus family centered).23
Oral health activities
Of all the studies reviewed, only two examined oral health activities in EHS program.17,20 These studies assessed the numbers of oral health activities performed by EHS and MSHS teachers, using self-administered questionnaires.17,20 Activities were divided into two categories, according to whether they were directed towards children or parents.17,20 Children activities included toothbrushing, toothpaste use, and classroom education.17,20 Parents’ activities included oral health education and promotion in addition to assessing children’s’ dental needs and parents’ oral health.17,20 The studies also assessed perceived oral health self-efficacy and barriers to performing oral health activities by staff members.17,20
One study compared oral health activities performed by EHS teachers with those performed by MSHS teachers.20 Fewer than half of EHS teachers (n = 260) were engaged in parent-focused activities as compared to more than 60% of MSHS teachers (n=72).20 Children-focused activities were highly reported for both EHS and MSHS programs with higher percentages of brushing related activities in MSHS program compared to EHS program.17,20 Both EHS and MSHS teachers were more likely to report the children brushing their teeth independently compared to assisting the children with toothbrushing.20 The results also indicated that 74% of MSHS teachers provided classroom oral health education compared to 45.2% of EHS teachers.20
Among barriers cited for performing parent activities, EHS teachers demonstrated the highest lack of knowledge regarding fluoride use.17 The most frequent barriers reported by EHS teachers for performing children activities included inadequate oral health education resources and knowledge regarding oral health activities.17 For EHS directors and health coordinators, difficulty in locating dental professionals willing to provide dental services for children younger than three and accepting Medicaid insurance reimbursement, were the most frequently cited barriers for performing oral health activities.17
Oral health promotion
Chinn evaluated the effectiveness of an oral health promotion intervention program on oral health knowledge and confidence of HS/EHS staff using a self-administered survey before and after the implementation of the Columbia Head Start Oral Health Program (C-HSOHP).21 The intervention program consisted of oral health education and training to include dental screenings and assistance with referrals to dental services.21 Chinn found that a majority of the staff members (n=61) believed that oral health training and dental screenings were effective in improving children’s oral health.21 In addition, HS/EHS staff members’ perceived self-confidence in communicating with parents and oral health professionals regarding children’s oral health both increased from pre- to post- surveys by 15% and 20%, respectively.21 Furthermore, dental referrals among staff members improved after the C-HSOHP by 20%, however there were no significant differences in identifying oral health issues, dental pain, and the overall oral health status of children.21
Discussion
Early Head Start children are considered high risk for developing ECC due to familial and environmental factors.10 Preventive oral health activities within EHS programs can be beneficial in providing education and promoting healthy oral habits for children and their families.25 Effective oral health education programs that target children, parents, and caregivers have improved oral health knowledge and reduced the disease prevalence among children.26 Literature demonstrates that it is more effective to provide oral health education through promotional activities for preventing oral diseases.25,26
To the best of the authors’ knowledge, this is the first systematic review to examine oral health education and promotion activities within EHS programs. The review revealed only five studies that examined oral health education and promotion activities in EHS programs and these studies were observational or quasi-experimental.17,20-23 Three of the five studies focused on evaluating oral health education and promotion interventions,21-23 while two studies directly assessed oral health activities in EHS.17,20 In most studies, researchers controlled for confounders, such as participants’ level of education and oral health knowledge.17,20-23
Evidence on the effectiveness of oral health education interventions was demonstrated in two studies that received a strong or moderate overall quality scores by the raters.22,23 In spite of the limitations with these studies, including small sample sizes and lack of follow-up of long-term effects, the results revealed that oral health education interventions in EHS are effective in increasing pediatric oral health knowledge among both staff and parents.22,23 Oral health activities were assessed in two studies with moderate overall quality scores and revealed a low number of oral health activities within EHS programs.17,20 In the Head Start Oral Health Project evaluation report of 2001 – 2008, it was recommended that more oral health educational resources be made available to all HS programs and more importantly that collaboration with dental hygienists is needed to support oral health activities within EHS.25
Oral health promotion was investigated in one study that utilized a community oral health training grant program in HS/EHS to improve pediatric oral health knowledge of staff members and parents.21 In addition, the program provided children with dental screenings and assisted with dental referrals.21 Although, the results demonstrated significant differences in pediatric oral health knowledge and competence among HS/EHS staff members, data was not presented on the children’s oral health before and after the intervention program.21 The study received a weak overall quality score due to insufficient control of confounders, social desirability bias, and unclear validity of data collection instrument.21
Limitations of this systematic review include a small number of studies that met the inclusion criteria and there were no randomized control designs identified. Furthermore, none of the included studies provided data on children’s oral health outcomes resulting from the interventions implemented among EHS program directors, teachers, health coordinators, and parents.17,20-23 Despite these limitations, this review provides information on oral health education and promotion activities within EHS programs that resulted in improved oral health knowledge among parents, and EHS directors, teachers, and staff members. These studies can be used as a framework to develop and evaluate future oral health education and promotion activities for EHS programs. Furthermore, the need is recognized for investigating and reporting oral health outcomes of EHS enrolled children as a future research direction.21
Dental hygiene implications
The American Dental Hygienists’ Association (ADHA) encourages the promotion of oral health among low-income children and families through expanding the dental hygiene scope of practice to include their participation in community oral health programs.27 Head start and EHS programs provide an opportunity for oral health care professionals to conduct education programs and promote interventions in to reduce the risk of ECC among young children.23 Results of the studies included in this literature review revealed improved oral health knowledge of EHS staff members, parents and caregivers resulting from oral health education and promotion interventions.22,23 Dental hygienists have a key role to play in promoting oral health and preventing ECC among children participating in EHS.2 The Dental Hygienist Liaison Project (DHL), a partnership between the National Center on Early Childhood Health and Wellness and the ADHA, was formed to promote oral health among HS enrolled children, parents and staff members.29 The project provides oral health education and increases children’s access to dental services by connecting the HS community with dental hygiene education programs and dental professionals.29 However, only a limited number of dental hygiene education programs have partnered with HS/EHS to provide dental hygiene services for children.30,31 Dental hygiene education programs that have collaborated with HS/EHS programs have provided dental screenings and prophylaxis for children in addition to oral health education for children and parents.30,31
In addition to working with HS/EHS programs, there are opportunities for dental hygiene students to provide oral health education and dental hygiene care for pre-school aged children through community outreach and service-learning endeavors. Claiborne et al. implemented an innovative, collaborative service-learning activity that was provided by dental hygiene and primary care nurse practitioner students, with a focus on oral health education and dental screenings for pre-school aged children.32 The program demonstrated a positive experience for the pre-school aged children and provided an interprofessional education experience for dental hygiene and primary care nurse practitioner students.32 Dental hygiene education programs and practicing professionals who collaborate with HS/EHS programs can provide essential dental hygiene services to children and increase access to oral health care.30,31
Conclusion
A limited number of studies have examined oral health education and promotion activities for EHS staff members and parents. Studies that focused on increasing pediatric oral health knowledge and practice behaviors among EHS staff members and parents revealed improved oral health knowledge and behaviors. Ongoing studies are needed to examine the effectiveness of oral health education and promotion interventions within EHS programs. Impacts of oral health education and promotion interventions on children’s oral health also warrant examination in EHS programs. Collaboration with dental hygienists and dental hygiene education programs can support the oral health education and promotion activities of EHS programs and positively impact pediatric oral health and access to oral care.
Footnotes
This manuscript supports the NDHRA priority area, Population level: Health services (Community health interventions).
- Received August 17, 2020.
- Accepted January 29, 2021.
- Copyright © 2021 The American Dental Hygienists’ Association





{kind=link}