



Abstract
Purpose: Objective Structured Clinical Examinations (OSCEs) have been established as a gold standard assessment for determining clinical competence. The Coalition for Dental Licensure Reform called for the acceptance of the Dental Licensure Objective Structured Clinical Examination (DLOSCE) to replace the live-patient examinations (LPE) for dental licensure, which are often viewed as biased, unreliable, and in some cases unethical. The purpose of this study was to assess dental hygiene program directors’ awareness of and attitudes toward the DLOSCE, whether their curricula included OSCEs, and perceived barriers to implementing OSCEs.
Methods: A nine-question electronic survey was developed, and pilot tested by five-dental hygiene program directors across three-dental hygiene institutions. The survey was emailed to the directors of all dental hygiene program directors in the United States (n=332). Descriptive statistics were used to analyze the data.
Results: A response rate of 36% (n=121) was achieved. Nearly 30% of respondents were unaware of the developing DLOSCE, however, the majority (80%) were in favor of the acceptance of the examination. Nearly three-quarters of the respondents considered OSCEs as valid assessments of clinical competence, however, over half of the respondents reported not currently utilizing OSCEs in their curricula. Barriers reported were time (22%), perceived lack of best practices (21%), and lack of resources (18%). Respondents who currently employed OSCEs were more likely to agree they were both valid and reliable assessments (p=0.05).
Conclusion: The majority of dental hygiene program directors were in favor of eliminating the single-encounter LPE in favor of an OSCE for licensure. However, more than half do not currently utilize OSCEs for clinical assessments. Further studies are needed to explore implementation of OSCEs in dental hygiene education, and how a potential dental hygiene licensure OSCE might impact the current curricula and licensure of dental hygienists in the United States.
- dental hygiene education
- clinical evaluations
- clinical competence
- Objective Structured Clinical Examinations
- live patient examinations
Introduction
The purpose of clinical licensure examinations is for clinicians to demonstrate their knowledge and competency prior to serving the public.1,2 However, debates surrounding the use of human subjects in dental and dental hygiene clinical licensure examinations have been discussed among dental communities for decades.2–5 While some argue that this clinical demonstration of competency necessitates the use of human subjects, others counter that live-patient examinations (LPE) assess a narrow range of clinical skills, and raise considerable ethical concerns for the patient, candidate, and profession.5 Alternative methods to assess the clinical competence of dental professionals have been explored across the United States (U.S.) however, LPE remain to be the most frequently used method in dentistry to date.6
The pathway for dental licensure was established in 1929 by the National Board of Dental Examiners (NBDE).7 The NBDE oversaw the development and administration of both the written and clinical portions of licensure examinations until 1937, when clinical licensure examinations were relinquished to individual state boards of dentistry. Subsequently, each state became the profession’s governing body, issuing dental licenses and ultimately limiting their portability. As a means to develop, calibrate and administer clinical examinations, state boards of dentistry grouped together to form regional boards.8 These boards rely on regional testing agencies to administer clinical licensure examinations. Although licensure requirements may vary from state-to-state due to differences in state laws, there are three standard national requirements for licensure: 1) a degree from an accredited program, 2) a passing score on the written national board examination, 3) a passing score on a regional/state clinical examination.
Currently, dentistry is the only health care profession that requires the use of human test-subjects for licensure examinations.9 Concerns surrounding the use of human test-subjects for licensure examination are well founded; by their nature, they may introduce potential harm to the patient during the delivery of irreversible care.10 Within the context of the examination, candidates are more likely to attend to the licensure examination requirements, rather than the patient’s primary oral health needs.2,4 This can lead to delaying care, resulting in the mistreatment of these patients.2,4 Mistreatment may also occur upon completion of the examination, due to lack of follow-up care, or failure to plan treatment for substandard care.2,4,5,10 Additional ethical concerns surround the financial exchanges that occur during patient recruitment which may be misconstrued as coercion or bribery.10
The American Dental Association (ADA), the American Dental Education Association (ADEA), and the American Student Dental Association (ASDA) formed the Task Force on Assessment of Readiness for Practice (TARP), in 2016 to resolve the issues surrounding LPE and licensure portability. In 2017, TARP issued a report recommending further development and pilot testing of alternative methods to measuring clinical competence for initial licensure. The TARP report called for the replacement of LPEs and the acceptance of valid alternatives such as Objective Structured Clinical Examinations (OSCEs) as a replacement. Currently, OSCEs are being used as measures of clinical competency for initial licensure by the U.S. Medical Licensing Examinations, the Medical Council of Canada Qualifying Examination, and the National Dental Examining Board (NDEB) of Canada OSCE.11–13 Considering the validated successes of the NDEB of Canada OSCE, the ADA Board of Trustees voted to adopt the Dental Licensure Objective Structured Clinical Licensure Examination (DLOSCE) as a replacement for LPE. Piloting of the DLOSCE began in November 2019 and will be launched in June 2020.14,15
In response to the TARP report, the Coalition for Modernizing Dental Licensure was formed to begin lobbying individual state dental boards to accept the DLOSCE for initial licensure. Considering the wide variations in state dental practice acts, obtaining approval for the DLOSCE may be a lengthy process. However, as the ADA stated in their April 6, 2020 press release, they have seen an increased demand from state dental boards for the DLOSCE as a means to better protect the public during the current COVID-19 pandemic.15
In 2019, the American Dental Hygienists’ Association’s (ADHA) application to join the Coalition for Modernizing Dental Licensure was approved. As members of this coalition, the profession of dental hygiene will need to develop and submit a similar LPE alternative to state boards of dentistry, as the DLOSCE was created for dental students. Additionally, ADEA has created the Compendium of Clinical Competency to assist in the development of LPE alternatives. The compendium contains two assessment rubrics for clinical competence: one for dentistry and one for dental hygiene. These working rubrics were created to serve as guides for clinical assessments in educational programs, in addition to professional associations to create their own OSCEs for initial licensure.
The purpose of an OSCE is to minimize patient and evaluator variations while standardizing the skills and knowledge assessed.16,18,19 Decades of evidence across a wide range of health care disciplines have confirmed the validity of OSCE assessments as the standard for determining clinical competence.16 Since the mid-1970’s, OSCEs have been universally recognized as the gold standard for the assessment of clinical competence of allied health and other professional students16
An OSCE is a station-based examination, designed to assess multiple students’ clinical performances over the same materials, at the same time. Stations are timed and create a simulated scenario with the use of examination mechanisms including standardized patients, typodonts, manikins, medical histories, radiographs, mouth models, and instruments. Stations are evaluated by calibrated proctors using standardized rubrics and checklists to assess clinical performance. OSCEs are resource intensive to develop and implement, as compared to other assessment tools, making feasibility a practical consideration. Time constraints and lack of resources are common barriers reported in literature.20-22 Despite the labor-intensive nature of OSCES, studies show that educators believe OSCEs are valid and reliable tools for the assessment of clinical performance of students.18-20,22-24 Furthermore, OSCEs have been incorporated in dental school curricula since the 1990’s to assess a variety of skill sets, including communications, patient education, clinical skills, and critical thinking.17,25,26
While OSCEs are widely recognized in dental education; research is limited regarding utilization trends of OSCEs in dental hygiene education. In 2009, Navickis, et al., surveyed dental hygiene program directors to explore the use of various standardized clinical examinations in dental hygiene curricula.20 At the time of the study, 59% of the respondents utilized OSCEs and 46% felt that OSCEs were effective tools for verifying clinical performance; however 37% cited time as a barrier for implementation.20 There is a gap in the literature regarding current OSCE utilization trends in U.S. dental hygiene program curricula, raising concerns as to how an OSCE for dental hygiene licensure might impact the profession. While this study was not conducted during the current pandemic, it is important to note the relevance of OSCE assessments in light of the barriers to live patient treatment and face-to-face teaching introduced in the last year. The purpose of this study was to assess dental hygiene program directors’ current utilization of OSCEs, the perceived barriers of OSCE utilization and attitudes and awareness of the developing DLOSCE for dental licensure.
Methods
The study was determined exempt from University of Michigan Institutional Review Board oversight (HUM00147564). A nine-question, anonymous electronic survey was developed for distribution using Qualtrics (Provo, UT) survey software. The survey was initially reviewed and edited by the University of Michigan (UM) Survey Research Center for content validity and reliability. Survey questions explored descriptive demographic information including years as program director, highest degree offered at the respective institution, questions related to OSCE utilization and barriers, and awareness of the developing DLOSCE. Five-point Likert-scale questions assessed the perceptions of program directors regarding support of replacing LPEs with an OSCE for licensure, and their perception of the validity and reliability of OSCEs to assess the clinical competence of dental hygiene students. The survey was pilot tested by five dental hygiene program directors across three-dental hygiene programs. Modifications were made based on feedback.
A list of U.S. dental hygiene program directors’ email addresses (n=332) was obtained from the American Dental Hygienists’ Association (ADHA) Entry-Level Dental Hygiene Program Directory. A recruitment email introducing the purpose of the study and informed consent was sent along with a link to the survey. The survey was open to participants for eight weeks; three reminder notifications were emailed at two- week intervals.
Data were collected and analyzed in Qualtrics Survey Software; SPSS, version 25 (IBM Corp. Armonk, NY) was used for further analysis. Descriptive statistics included frequency distributions, percentages, and standard deviations were calculated to provide a summary of the findings. Inferential statistics such as ANOVA and Welch’s two-Samples t-tests were sought to provide inferences about the sample population. Significance was set at (p<0.05.)
Results
Of the 332 electronic surveys sent, 129 program directors initiated the survey and 121 completed the survey, for a response rate of 36%. The majority of respondents (60%) had served as a dental hygiene program director for ten years or less, and the majority (69%) reported the highest dental hygiene degree offered at their learning institution as an Associate Degree. Demographic frequencies types of degrees awarded at the institution are shown in Table I and reflect the national trend in dental hygiene education programs. Fewer than half of the respondents (49%, n=59) reported incorporating OSCEs in program curricula (Table II).
Demographics (n=121)
OSCE utilization in dental hygiene program (n=120)
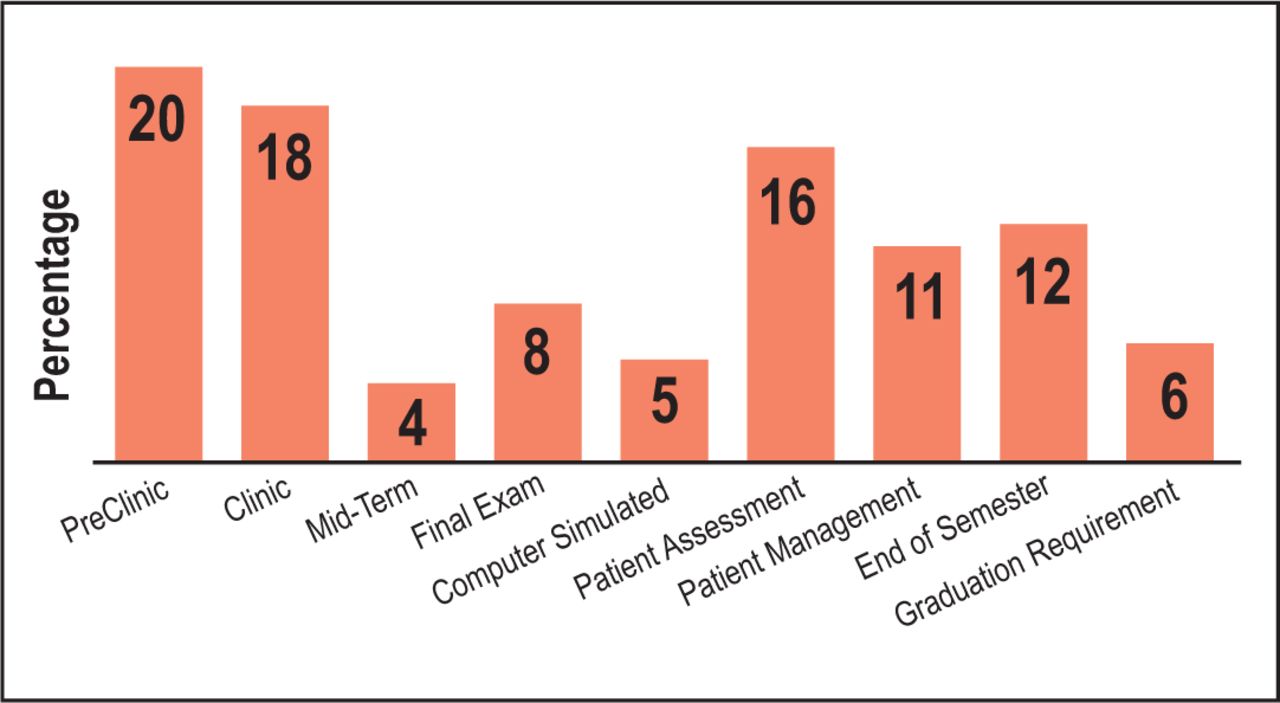
Figure 1 illustrates how and/or when OSCEs are used to assess clinical performance in the dental hygiene curricula. Of the respondents utilizing OSCEs, 20% reported their use in pre-clinic while 18% reported their use in clinic to assess competencies, test cases, and proficiencies. Only 6% of pro-gram directors reported using an OSCE as a require-ment for graduation. More than one-half of the respondents reported not incorporating OSCEs in their dental hygiene curricula (51%, n=61). Lack of time (22%), lack of evidence-based development processes (21%), and lack of resources (18%) were cited as barriers to implementation, while 9% reported that they were unfamiliar with OSCEs (Figure 2).
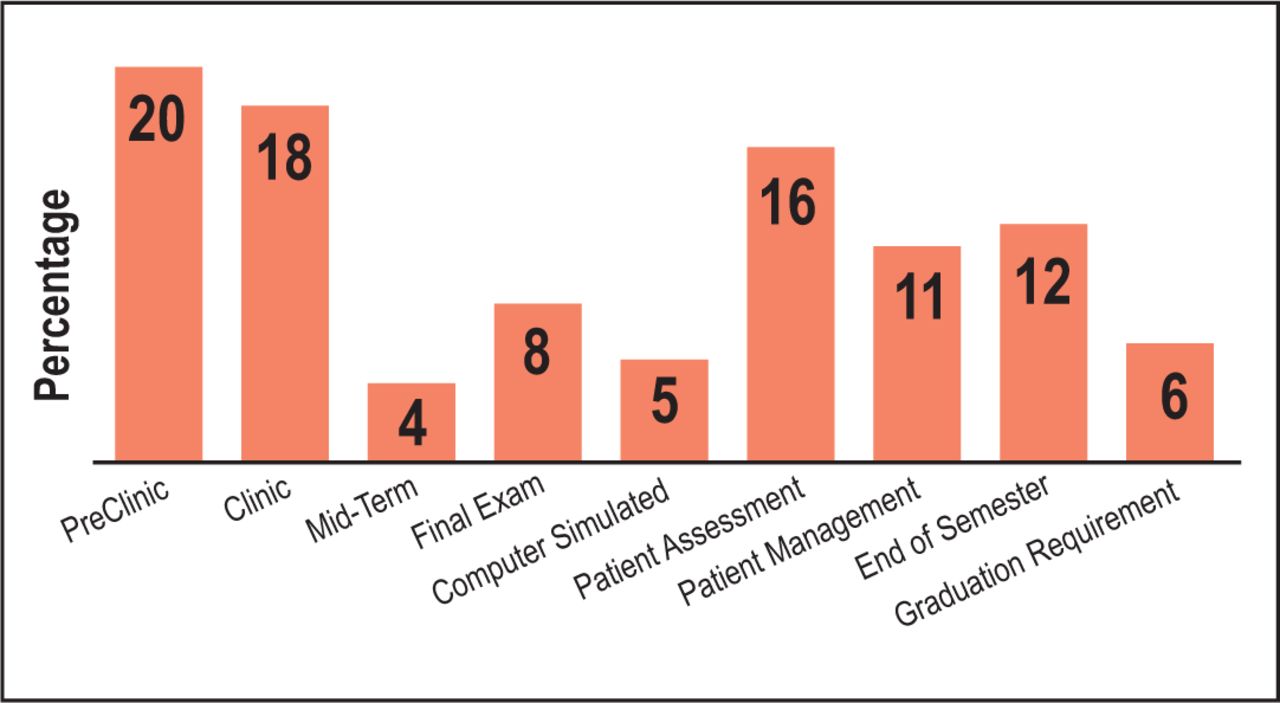
Types of OSCE utilization (n=59)

Perceived barriers (n=61)
Nearly one third of program directors were unaware of the development of the DLOSCE for dental licensure. However, the majority of respondents (80%) indicated they were in favor of the DLOSCE as a replacement of the LPE (Figure 3). Furthermore, nearly three quarters (72%) of respondents felt OSCEs were a reliable and valid methods for evaluating the clinical competence of dental hygiene students.
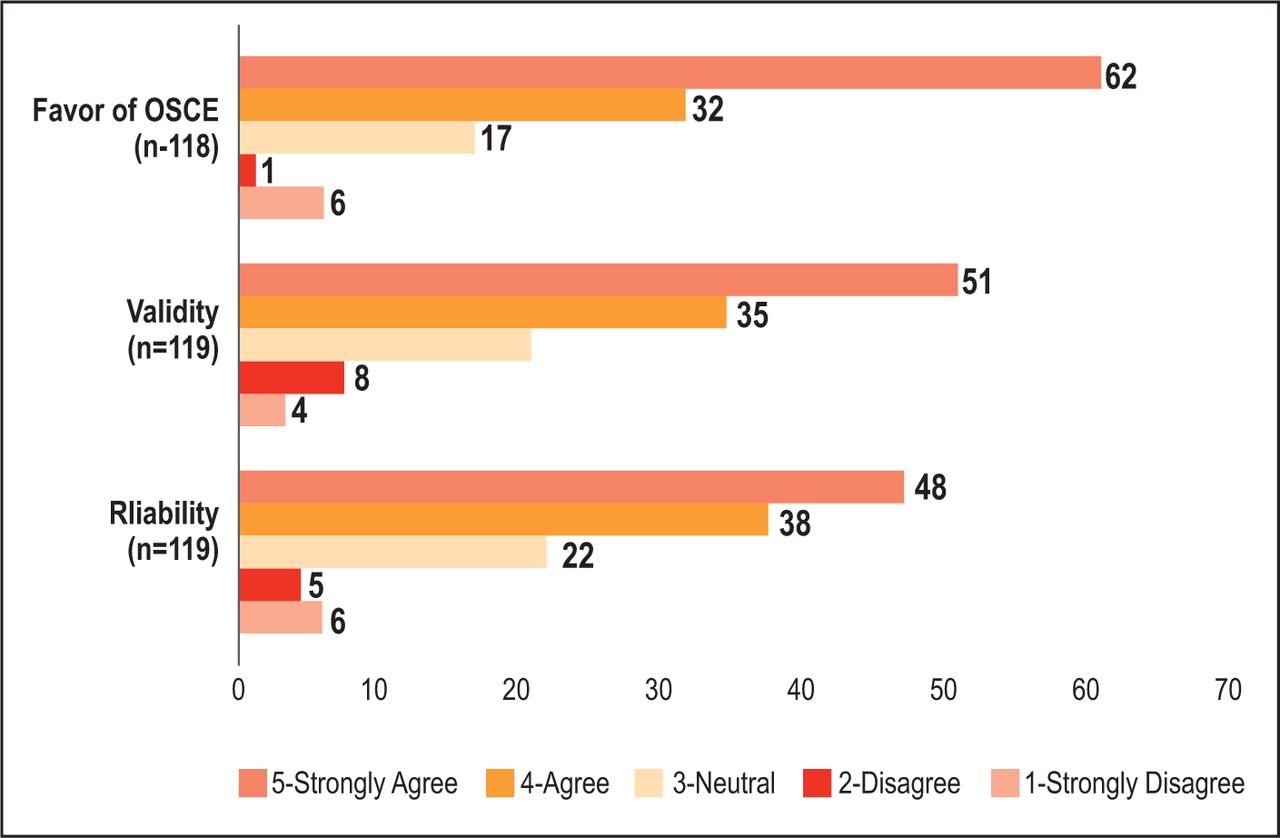
Respondents’ attitudes of OSCEs
Three Welch’s two sample t-tests were calculated to compare mean ratings of attitudes regarding favorability, validity, and reliability between respondents who utilized OSCEs and those who did not (Table III). Regarding favorability, statistical significance was not observed between the average ratings of respondents who utilize OSCEs compared to those who did not (p=0.131) However, statistical significance was observed in beliefs that OSCEs are valid (p=0.006) and reliable (p=0.011) assessment measures in respondents who utilize OSCEs compared to those who did not.
Attitude comparisons between respondents not utilizing OSCEs
An ANOVA test was conducted to compare whether the number of years as program director affected favorability of replacing LPE with an OSCE. No significant difference between the average favorability rating among respondents based on ranges of years of service was observed (f (5,12)=0.336, p=0.890).
Discussion
OSCEs have been a valid assessment measure of clinical competence of dental students for decades.25 This study was developed to assess the utilization of OSCEs in dental hygiene programs in the U.S. and the current attitudes of dental hygiene program directors towards the replacement of the single-encounter, LPE and the subsequent development of the DLOSCE by the ADA. It is of note, that this study was conducted prior to the COVID-19 pandemic and the current constraints on all face-to-face encounters are not reflected in the survey or study results.
In this study, nearly half of program directors reported utilizing OSCEs in their curricula. This is were lower than those of Navickis, et al., who reported that 59% of program directors surveyed, utilized OSCEs in their dental hygiene curricula.20 While the findings of the current study cannot confirm a decrease in OSCE utilization nationally, there does not appear to be a positive trend in the growth of OSCE utilization over the past decade. Both studies reported time constraints as their greatest barrier to OSCE utilization. However, when exploring attitudes; 72% of respondents in this study believed that OSCEs are a valid assessment tool, compared to 46% in the Navickis, et al. study. This growth rate in attitudes towards validity may be attributed to an increased awareness of OSCEs across healthcare education or increased understanding due to the recent efforts in dental education to change initial dental licensure pathways. Furthermore, results from this study demonstrated that dental hygiene program directors who currently utilized OSCE assessments in their curricula had a statistically significant higher levels of belief towards OSCEs as a valid and reliable means to assess clinical performance in dental hygiene students, as compared to those who did not utilize OSCE assessments in their curricula.
Between 2011 and 2016, over 400 articles have been published regarding the validity of OSCEs.25 Despite this evidence, more than half of program directors in this study reported not utilizing OSCEs within their curricula, with one-fifth reporting there was not enough evidence to support best practices in the development of OSCE assessments. The design of an OSCE is crucial to its validity as an assessment instrument, and the desire for an understanding of OSCE best practices is a valid concern. Furthermore, with approximately 9% of the program directors in this study unsure of what an OSCE is, it may be worthwhile to explore the ways dental hygiene program directors obtain information and stay current regarding trends in dental hygiene education such as the use of OSCE or other alternative clinical competency assessment strategies.
Interestingly, even though half of the respondents do not use OSCEs in their curriculum, 80% are in favor of replacing LPEs with OSCEs for licensure. These results are reflective of a 2016 survey of ADEA Allied Dental Program Directors, which noted that 78% of respondents did not feel the LPE adequately assessed clinical competence, with the vast majority (86%) supporting the elimination of the LPE.23
The decision to develop the DLOSCE for dental licensure is based on the consistent evidence that OSCEs are the gold standard among clinical assessments based on their ability to expose clinical and didactic strengths and weaknesses, in addition to enriching student learning.1, 5, 27 This evidence contradicts the argument that a LPE is the only valid way to determine competency for clinical practice in dentistry. By the same rationale, it disputes the question of the validity the current assessment strategies of student performance in clinical education settings. Student clinical assessments are dependent on the often-unknown patient presenting and the faculty member performing the assessment, which introduces a host of variability and subjectivity issues across the assessment process. Alternatively, OSCE assessments remove the often unpre-dictable and unreliable variables of standard clinical patient-based graded assessments.16
With the projected implementation of the DLOSCE as early as June 2020, licensure change is likely on the horizon for the dental hygiene profession. Therefore, it is crucial to consider standardizing the use of OSCE assessments in all dental hygiene programs. Implementing OSCEs throughout a student’s dental hygiene education can be an effective, valid, and reliable way to not only accurately assess clinical performance but also prepare dental hygiene education programs for these potential changes to licensure. As the ADHA supported Coalition for Reform in Dental Licensure prepares to lobby state boards of dentistry for alternatives to LPE for initial dental licensure, dental hygiene educators must be prepared to actively pursue viable future LPE alternatives for dental hygiene students.
This study had limitations. The 9-item survey instrument was intentionally brief to increase compliance; however, it restricted the breadth of the data collected. Self-reporting was another limitation as it increases the risk for biased responses and the results may not be representative of all dental hygiene programs. Limitations also existed surrounding the data analysis of dental hygiene directors’ perceived barriers of OSCE utilization in dental hygiene curricula. When asked to identify which barriers existed, the option resources were not explicit, making interpretation of the responses subjective.
Future studies should explore the potential impact of an OSCE-based dental hygiene licensure exam would have on an inadequately prepared dental hygiene education system, as well as current resources to prepare educators for such a change. Future research should also explore the awareness, knowledge acquisition and implementation of OSCE assessments by dental hygiene programs currently utilizing them for clinical competency assessment. Lastly, since nearly one-third of dental hygiene program directors in this study were unaware of the efforts to eliminate LPE for initial dental licensure or the subsequent DLOSCE, future studies should explore the attitudes and barriers that contribute to these knowledge gaps.
Conclusion
A majority of dental hygiene program directors in the U.S. were in favor of eliminating the single-encounter, LPE and favored assessments such as the DLOSCE, for initial dental hygiene licensure. However, nearly half of all program directors surveyed do not utilize OSCEs in their programs, suggesting that dental hygiene education programs may be unprepared to institute the development and integration of OSCEs into their curricula. Dental hygiene education programs may need additional resources and support regarding OSCE development, integration and best practices to help overcome barriers and increase utilization. Future studies are warranted to assess best practices of OSCEs in dental hygiene education and how the implementation of an OSCE for dental hygiene licensure may impact dental hygiene education in the U.S.
Footnotes
This manuscript supports the NDHRA priority area: Professional development: Education (educational models).
- Received February 17, 2020.
- Accepted June 1, 2020.
- Copyright © 2020 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}