



Abstract
Purpose: The goal of this paper is to evaluate the PEARL Network's satisfaction with training/support and assess the relationship between practice research coordinators (PRCs) involvement and study participation.
Methods: At the PEARL Network 2011 Annual Meeting, an evaluation form was completed by practitioner–investigators and PRCs who attended the annual meeting. Results from the paper evaluation form were entered into an Excel database, and analyzed using the statistical analysis software SPSS. The bivariate correlation test, Pearson Correlation, was conducted, and results were considered significant if p<0.05.
Results: During a program evaluation among 84 network respondents, a positive correlation (p=0.004) was found between the number of PRCs and the number of studies in which a site participates. In addition, there was a positive correlation between satisfaction with the training, support and involvement of PRCs in organizing study activities (p=0.008). There was also positive correlation between satisfaction with training/support and the number of PRCs utilized by the office (p=0.039).
Conclusion: Practice research coordinators are key members of the research team, and they are important to conducting clinical studies in everyday practice.
Introduction
Practice based research networks (PBRNs) are designed to answer questions about everyday practice, and they have the potential to change and improve the practice of dentistry. Office based research requires the participation of the dentist, termed the Practitioner–Investigator (P–I) and a staff member designated as the practice research coordinator (PRC), who is often a dental hygienist. The Practitioners Engaged in Applied Research and Learning (PEARL) Network defines a PBRN as “collaboration between an academic health science center(s) and community practitioners conducting primarily clinical studies of mutual interest that would benefit and enhance patient care, delivery, cost, and health care policy.”1 PBRNs require an infrastructure to conduct studies and include: P–Is, PRCs, clinical research associates (CRAs), a data coordinating center, personnel to analyze results and administrators. PEARL can serve as the basis of an infrastructure to support “big science.”2 The vision of big science is that by pooling resources researchers can learn more together than from independent observations outside of organized science. An example of big science outside of health care is the large Hadron Collider near Geneva, Switzerland organized by the European Organization for Nuclear Research (CERN), which involve large numbers of investigators from many countries.3 The advantage of big science in dentistry is that it allows researchers to evaluate practice and procedures systematically.
The Role of the PBRN in Dentistry
The PEARL Network is ideally positioned to evaluate and disseminate precise and accurate definitions related to diagnosis codes, disease states and risk factors for use in dentistry. “This may have the potential to create real–time evaluation of new advancements in medications, products, and procedures in dentistry that are relevant, practical, and applicable to everyday practice.”4 The PBRN initiative has the potential to impact the future of dentistry in many ways: it increases the knowledge base of the profession, it provides a place to find answers to questions related to clinical care, it creates a resource for providers to continue learning throughout their career and it builds connections between providers to enhance professional development. Providers report a sense of ownership of the results because they reported the data first hand.5 PEARL provides the opportunity to increase the adoption of knowledge and transfer of information into practice thereby closing the translational gap.
The Role of the PRC in a PBRN
In many ways PRCs are essential to the success of practice based research teams, and their contributions are recognized. Dental hygienists are formally educated members of the dental team. They are well suited to present the informed consent prior to treatment, and can interpret and translate the protocol for the patient, once trained in the principles of good clinical practice. Good clinical practice “is an international ethical and scientific quality standard for designing, conducting, recording, and reporting trials that involve the participation of human subjects.”6 Some of the common strengths of PRCs include organizational expertise, communication skills and attention to detail. Dental hygienists who engage in clinical research may experience career growth and professional development. Some PRCs in the PEARL Network have commented anecdotally about greater job satisfaction through participation in research and contributing to the knowledge base of the profession. Learning skills needed to conduct standard of care studies in accordance with good clinical practice also prepares dental hygienists as teachers or educators,7 or as research industry professionals. Through participation, PEARL Network research studies provide Network dental sites with a method to objectively measure and benchmark what is happening in the office. An example is the PEARL analgesic study and communication discrepancies reported between patients and providers in that study.8–10 The PEARL Network found in the analgesic study that there was significant variation between the providers documented recommendation and patients perceptions for analgesics used for pain control.
Comparative Effectiveness Research (CER) and the PBRN
In oral health research, the PBRN provides the opportunity to conduct comparative effectiveness research. This type of research compares patient outcomes for various treatments and procedures looking at effectiveness, efficiency and cost data. Some policy makers believe comparative effectiveness research may have the potential to align payments with evidence based care.11 The PEARL Network shares values with other well intentioned international health research organizations. PEARL “provide(s) answers to the complex and difficult questions that decision makers face when designing policies that affect health and health care.”12 In 2005, a major investment in the future of dentistry was made by the National Institute of Health's National Institute of Dental and Craniofacial Research (NIH/NIDCR) with the development of the PBRN program for dentistry.13 A 7 year award was given to initiate 3 PBRNs with a focus on oral health. Starting in 2012 there will be a single PBRN in dentistry, the National Network. The NIDCR would like to grow the organization significantly during the next 7 year phase of this initiative.14
The PEARL Network
The PEARL Network's administrative headquarters are located at New York University in New York, and are comprised of 3 cores: the protocol development and training core, information dissemination core and the recruitment, retention and clinical operations core. The clinical operations department is staffed with a team of CRAs who work to ensure compliance under good clinical practice requirements and data integrity. The PEARL Network strongly recommends each site have a PRC. The next iteration of the grant defines PBRN P–Is as dentists, dental hygienists and other dental professionals who are engaged in the daily practice of dentistry.15
The goal of this paper is to evaluate a PBRN, the PEARL Network's satisfaction with training/support and assess the relationship between PRCs involvement and study participation.
Methods and Materials
At the PEARL Network 2011 Annual Meeting held in New York, an evaluation form was completed by 130 network respondents (P–Is and PRCs who attended the meeting). The form was developed by PEARL Network staff and was not tested prior to being administered. Of the network respondents, there were 74 P-Is and 56 PRCs. The evaluation form asked questions about how involved PRCs are in coordinating study activities, how many PRCs each site utilizes and the satisfaction with training and support. The evaluation form also measured how many clinical studies the respondent participated in. The PEARL Network Program Evaluation was not classified as human subject research, because it was not a systematic investigation and no identifying personal information was collected. Results from the paper evaluation form were entered into an excel database, and analyzed using the statistical analysis software SPSS. The bivariate correlation test, Pearson Correlation, was conducted, and results were considered significant if p<0.05.
Results
Eighty four participants completed the evaluation and returned it to the Network staff. The evaluation form did not differentiate between P–Is and PRCs, or ask respondents their role in the dental team. The network respondents answered positively to the overall evaluation of how satisfied they are with the training and support they have received from the PEARL Network throughout their participation, and they reported positive levels of satisfaction with using PEARL's electronic data capture system, Advantage EDCSM.

PEARL Network PRC Involvement and Evaluation of Training
A statistically significant correlation (p=0.004) was found between the number of PRCs at a site and the number of studies in which the site participated. The level of involvement of the PRCs in coordinating study activities was rated: 0=not applicable (not performed by a PRC), 1=low, 2=medium, 3=high and the number of studies participated in captured. Ratings for PRC satisfaction with training and Advantage EDCSM were: 1=poor, 2=fair, 3=good and 4=excellent. In addition, there was a correlation between satisfaction with the training/support and the involvement of PRCs in organizing study activities (p=0.008), and a correlation between satisfaction with training/support and the number of PRCs utilized by the office (p=0.039). From our interaction with the PRCs during monthly PRC calls, the CRA team expected to see a relationship between the number of PRCs and overall satisfaction. Feedback from CRAs supports that when the practice has motivated people to help conduct research it is easier for the office to participate. PRCs have also reported a sense of pride with certification, and a sense of accomplishment when the CITI tutorial is completed. Another reported benefit of participation is that providers feel more connected to the results, and report that they have a greater sense of buy in because the results are generated in their practice.
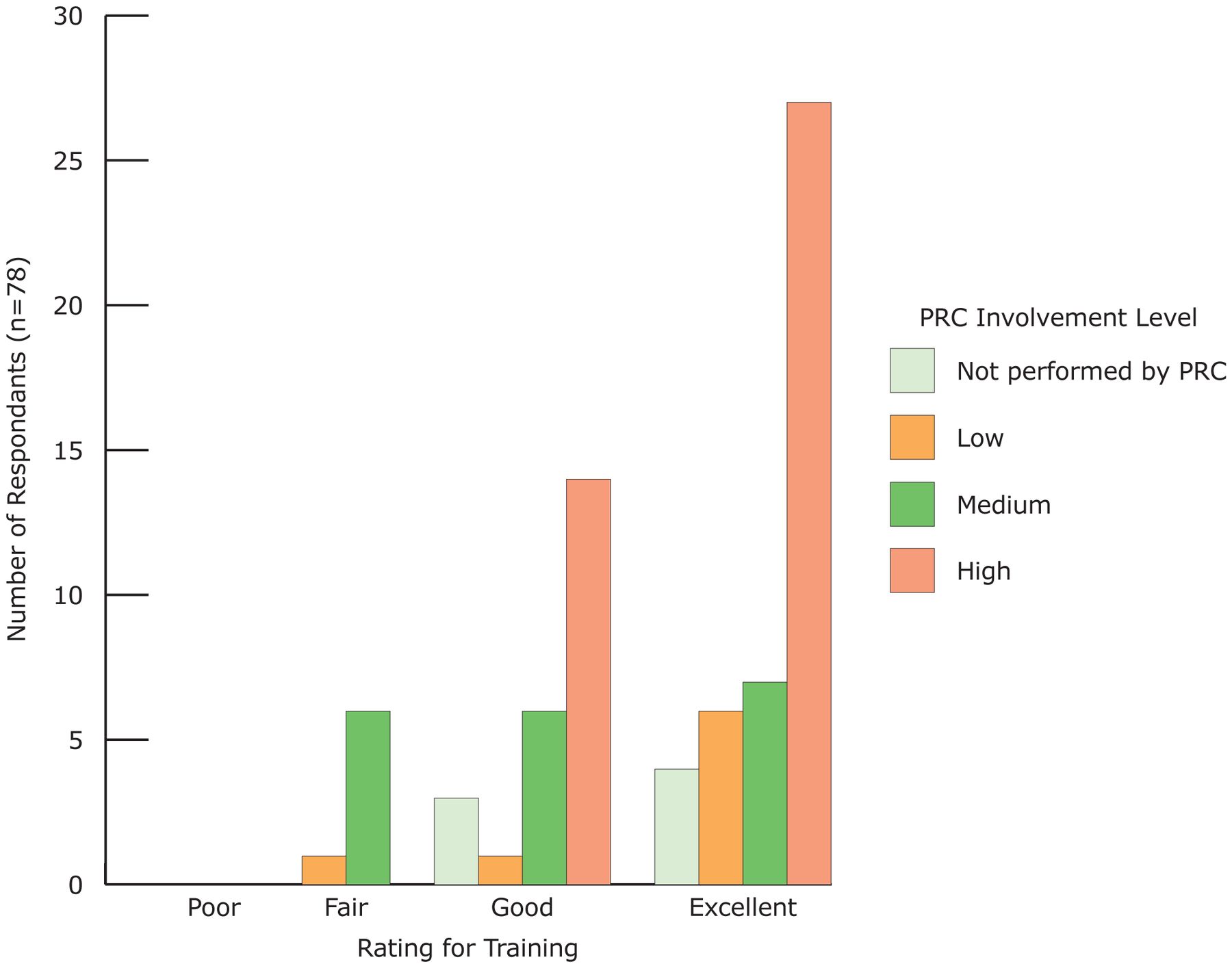
Figure 1 shows the frequency number of respondents who rated the PRC involvement (not performed by PRC, low, medium or high) by the rating for the training (poor, fair, good or excellent). There was a statistically significant positive correlation between the rating of training and the level of PRC involvement (p=0.008). This was another relationship that was identified by the CRAs during the PRC teleconference calls. The CRA team observed that offices with increased PRC personnel participated more actively in the network. PEARL has a limited number of member dentists who have taken on the role of the research team. The CRA team has observed the offices ability to participate and enroll patients in multiple studies is dependent upon the participation and interest of the PRCs.
Discussion
To date, the studies in the PEARL Network have addressed issues that improve the evidence basis for patient care, such as providing real world outcomes data for dentin caries activity,16 root canal therapy at 3 to 5 years post treatment,17–21 reporting the risk factors for osteonecrosis of the jaw22 and presenting data about analgesic use effectiveness.8–10 In addition, the studies strive to improve patient centered care, by providing dentistry with a better understanding of the oral health impact of dental disease and treatment procedures on the patient's quality of life of patients.23 All patients who enroll in a study complete the Oral Health Impact Profile.24 Currently, the Network is preparing multiple publications related to the studies described above.
The results indicate that participation in the PEARL Network and the satisfaction with network training/support correlates with the number of PRCs at a dental PBRN site. This would suggest that the PBRN has a positive effect on dental practices with support staff, and that the ADA model for optimal efficiency in a dental practice corresponds to that of a dental practice based research site. We posit that additional PRCs provide a support mechanism at dental practices engaged in clinical research, and they have the ability of learning from one another, thereby supplementing the training provided by PEARL CRAs. More PRCs may reduce the burden of participation, possibly by distributing the workload between multiple individuals. In addition, provider satisfaction with communication and dissemination efforts should be evaluated, and the satisfaction during professional development can be made possible and facilitated through the Network. As the network grows, both national and regional differences in responses to the network evaluation should be analyzed to enhance dental care, facilitate quality, cost effectiveness and the ultimate goal of improving health and well–being.
Conclusion
Just as dental hygienists are key members of a dental practice, PRCs are key members of the PEARL Network PBRN clinical research team. The evaluation demonstrated the positive relationship between PRC involvement when conducting clinical studies in our dental PBRN. We found a correlation between the number of PRCs at a site and the number of studies in which a site participates. Further, the number of PRCs involved in organizing research activities at the site was found to be related to satisfaction with the training and support systems implemented by the PEARL administrative and clinical operative team. Future evaluations will look at additional information about how different types of providers (P–Is and PRCs) differ in their response to the evaluation forms.
Footnotes
-
Ashley Grill, RDH, BSDH, MPH, is a clinical assistant professor of dental hygiene at the New York City College of Technology. Joanne M. Johnson, RDH, is an associate in evidence based dentistry at the DentaQuest Oral Health Center. Damon Collie, BS, MSHS, is the project manager of the Data Coordinating Center for the PEARL Network at the EMMES Cooperation. Van P. Thompson, DDS, PhD, is the PEARL Network Director of Protocol Development and Training, Professor; Chairperson Biomaterials, King's College London Dental Institute. Ronald G. Craig, DMD, PhD, is the PEARL Network Director of Information Dissemination, Associate Professor; Basic Sciences and Craniofacial Biology, Department of Periodontology and Implant Dentistry, New York University College of Dentistry. Frederick A. Curro, DMD, PhD, is the PEARL Network Director of Recruitment, Retention and Operations, Director of Regulatory Affairs, Bluestone Center for Clinical Research, New York University College of Dentistry.
-
This study supports the NDHRA priority area, Health Services Research: Evaluate strategies that position and gain recognition of dental hygienists as a primary care providers in the health care delivery system.
- Copyright © 2013 The American Dental Hygienists’ Association





{kind=link}