



Abstract
Purpose: Gingival enlargement, also synonymous with the terms gingival hyperplasia or hypertrophy, is defined as an abnormal overgrowth of gingival tissues. A case of a 19–year–old male presenting with maxillary and mandibular chronic inflammatory gingival enlargement associated with prolonged orthodontic therapy is reported here. Surgical therapy was carried out to provide a good aesthetic outcome. No recurrence was reported at the end of 1 year. The importance of patient motivation and compliance during and after therapy as a critical factor in the success of treatment has also been highlighted through this case report.
Introduction
Gingival enlargement, a globally accepted terminology for an increase in the size of the gingiva, is a general feature of gingival diseases. It is a multifactorial condition that develops in response to various stimuli and interactions between the host and the environment. It may be plaque–induced or associated with systemic hormonal disturbances. It also occurs as a manifestation associated with several blood dyscrasias, such as leukemia, thrombocytopenia or thrombocytopathy. A rare variant, idiopathic gingival fibromatosis, with a familial inheritance, has also been reported.1 Based on the extent and severity, these enlargements may lead to functional disturbances like altered speech, difficulty in mastication and aesthetic and psychological problems.
Inflammatory gingival enlargement may be categorized as acute or chronic, wherein chronic changes are much more common.1 The ability to perform oral hygiene measures is compromised in some patients with gingival enlargements, which may be further complicated by the presence of prosthesis and fixed orthodontic appliances. This may lead to more inflammation and further plaque accumulation perpetuating this vicious cycle. Thus, there is a transformation of the gingival sulcus into a periodontal pocket creating an area where plaque removal becomes impossible.
One of the most important determinants of treatment outcomes is patient compliance. The willingness to perform adequate oral hygiene measures and receive timely periodic recalls and treatment are deemed essential for a successful outcome. The therapeutic approaches related to gingival enlargement are based on the underlying etiology and the subsequent changes it manifests on the tissues. The prime treatment modalities involve obtaining a detailed medical history and non–surgical periodontal therapy, followed by surgical excision to retain esthetical and functional demands.
This case report presents a case of chronic gingival enlargement associated with prolonged orthodontic therapy.
Case Report
A 19–year–old male patient reported to the Department of Periodontology, Manipal College of Dental Sciences, Manipal, India. The patient complained of swelling of the upper and lower gums in the front tooth region. The patient had noticed the swelling 3 years prior and reported that it had not increased in size since then. He also complained of bleeding from the gums while brushing. The patient revealed that he had undergone incomplete orthodontic treatment which was initiated 6 years prior. There was no other relevant medical, dental or family history.
Consistent with the history of incomplete orthodontic treatment, intraoral inspection revealed orthodontic molar bands and brackets on all teeth except the maxillary left central incisor. On clinical examination, marginal and papillary gingiva appeared red and enlarged in the maxillary and mandibular arches, which was more prominent in the anterior sextants and also more pronounced on the right side as compared to the left (Figures 1, 2 and 3). Further soft tissue assessment revealed soft and edematous consistency and bleeding on probing on all teeth.
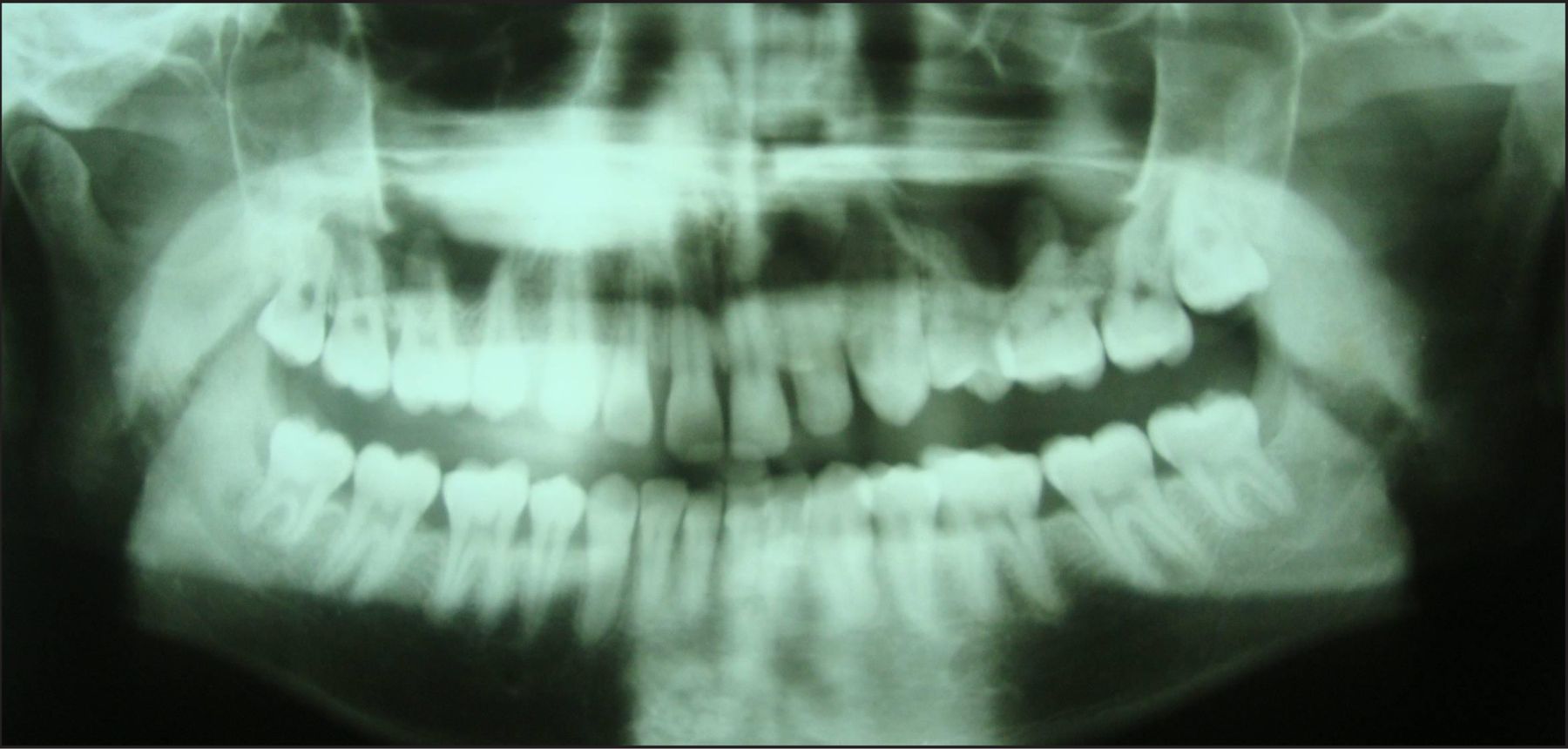
A treatment plan consisting of initial periodontal therapy followed by a gingivectomy procedure was planned to improve aesthetics and function. The initial periodontal therapy comprising supragingival and subgingival scaling was performed. Oral hygiene instructions were given and the use of chlorhexidine mouthwash (0.2% Clohex™, Dr. Reddy's Laboratories Ltd., India) twice a day for one week was advised. At the next visit, in spite of use of the prescribed medicated mouthwash, the gingival enlargement did not show considerable reduction in size, but the tissues appeared to be firm in consistency. At this stage, radiographs were taken and complete blood count investigations (RBC, WBC and platelet counts, ESR, bleeding time, clotting time, prothrombin time) were carried out (Figure 4).
Results
These investigations were non–contributory. An internal bevel gingivectomy was performed for the maxillary sextant. The excised tissue was sent for histopathological examination. Following this, the patient failed to report for subsequent recall appointments.
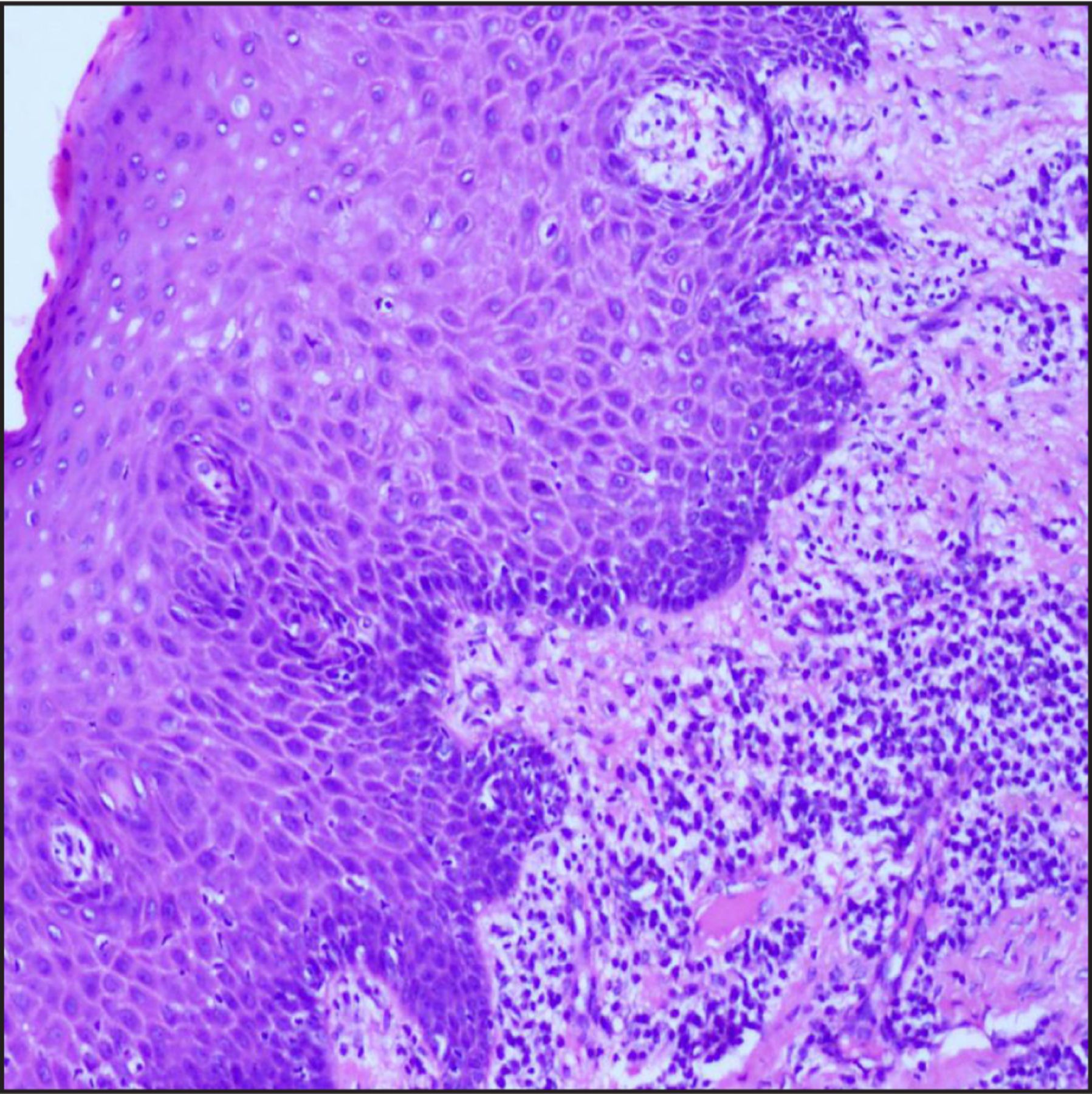
The histopathological examination revealed a hyperplastic parakeratinized epithelium overlying inflamed connective tissue. The underlying stromal tissue showed numerous proliferating young fibroblasts admixed with focal aggregates of chronic inflammatory cells. Few fibroblasts appeared stellate, with numerous nuclei distributed in a collagenized stroma. At places the stromal tissue exhibited myxoid degeneration. A histopathological diagnosis suggestive of inflammatory fibrous hyperplasia was given (Figure 5).
One year later, the patient reported back to the clinic. At this stage, the patient also expressed the unwillingness to continue the orthodontic therapy. Intraoral examination revealed that the maxillary surgical site had healed satisfactorily. There was no recurrence of the gingival enlargement in the maxillary anterior sextant (Figure 6). However, enlargements in the untreated areas persisted. Initial periodontal therapy was performed again and oral hygiene instructions were reinforced. To further improve plaque control measures, the orthodontic appliances were removed at this stage by the orthodontist. The patient was also counseled regarding the importance of follow up and maintenance with special emphasis on motivation.

Intra–oral pre–operative right lateral view

Intra–oral pre–operative frontal view

Intra–oral pre–operative left lateral view

Orthopantomograph
Following this, gingivectomy was performed in the mandibular anterior sextant (Figure 7) and maxillary right posterior sextant at different scheduled appointments. Then the patient was reviewed and healing was found to be satisfactory.
Discussion
Gingival overgrowth varies from mild enlargement of isolated interdental papillae to segmental or uniform and marked enlargement affecting 1 or both of the jaws with a diverse etiopathogenesis.2
Here, we report a case of chronic inflammatory gingival enlargement. These enlargements are often associated with a long–standing bacterial plaque accumulation. Regular professional oral prophylaxis and good patient compliance are required in the management of such cases. In this case, patient compliance was lacking as evidenced by the history of incomplete orthodontic treatment and the failure to report for regular recall appointments. Also, the presence of the appliances may have further compromised the maintenance of adequate oral hygiene. This reflects the importance of patient education, motivation and compliance during and after dental treatment. Reinforcement of effective oral hygiene is essential, since patients have a tendency to revert to their original behavior. The patient must be placed into a maintenance schedule to preserve a healthy dentition.
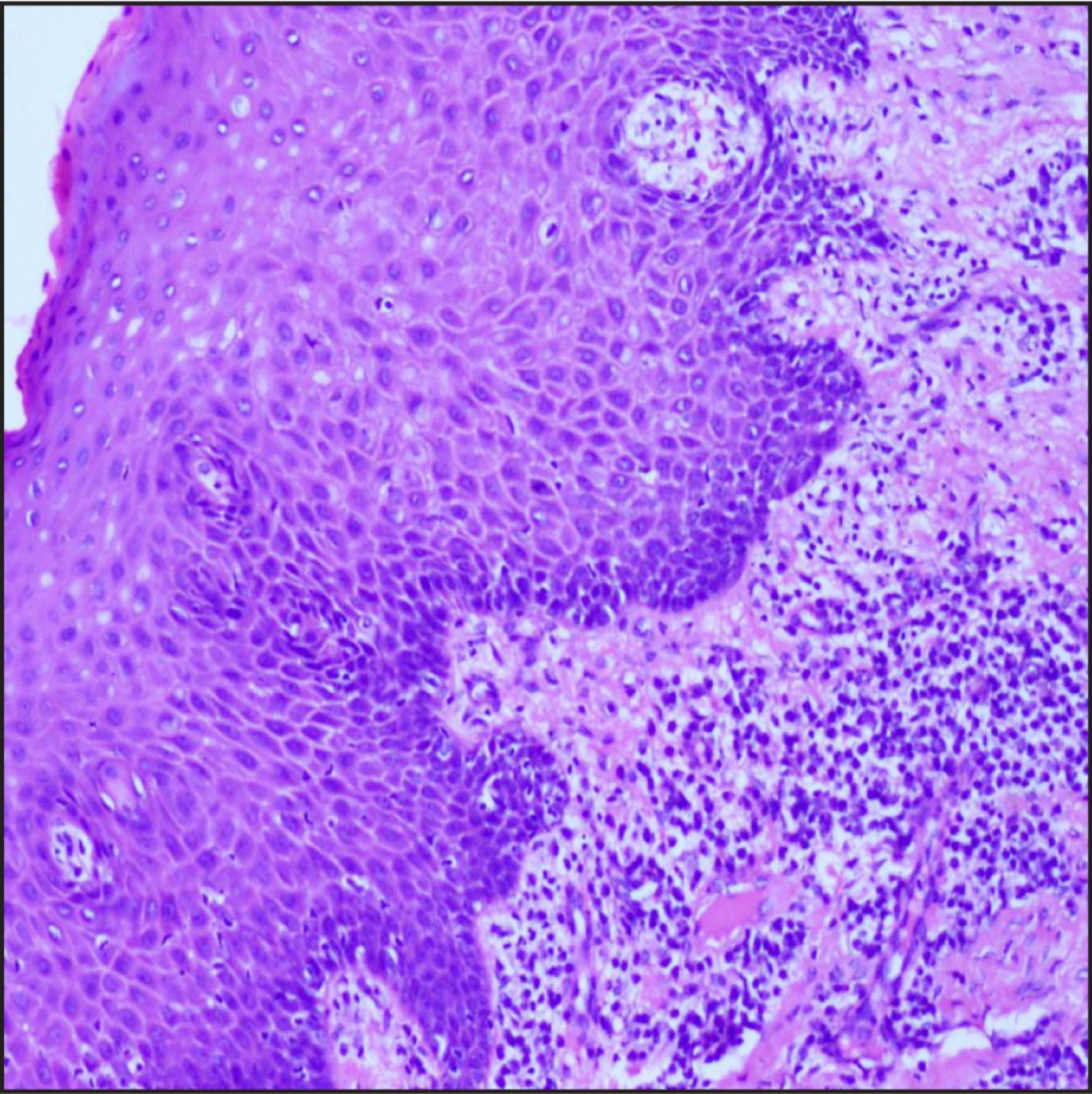
Histological section showing hyperplastic parakeratinized epithelium with fibro–collagenous connective tissue with chronic inflammatory cells (H&E 10X)
Consequently, it was noticed that once the appliances were removed and oral hygiene instructions were reinforced, the patient was able to maintain good oral hygiene. A study by Sallum et al showed significant impact of orthodontic appliance removal and professional prophylaxis on periodontal health.3

Maxillary arch 12 months postoperative view after gingivectomy
The patient was recommended to undergo complete blood investigations to rule out underlying systemic disease and allergies. Some authors have reported a possible allergic reaction to orthodontic metal which may cause gingival enlargement. Allergic contact stomatitis by dental metals, particularly nickel, has shown to cause gingival hyperplasia. Özkaya et al reported 2 cases with nickel–induced oral mucosal hyperplasia.4 Although extremely rare, a hyperplastic form has also been reported in single cases from nickel in dental appliances5,6 and from gold and palladium in a dental clasp.7
Orthodontic treatment–induced gingival overgrowth shows a specific fibrous and thickened gingival appearance, different from fragile gingiva with marginal gingival redness, which is seen in allergic or inflammatory gingival lesions. Histologically, inflammatory gingival hyperplasia is mainly observed as an increase and thickening of mature collagen bundles in the connective tissue stroma. Microscopic appearance of fibroblasts in the connective tissue stroma and chronic inflammatory cell component is suggestive of non–specific gingival enlargement. Fibrous gingival enlargements associated with fixed orthodontic appliances seem to be transitory, and it is generally thought that enlargement resolves after orthodontic therapy.1 However, there are also studies reporting that this resolution is not complete.8,9
When chronic inflammatory gingival enlargements include a significant fibrotic component that does not resolve completely after initial periodontal therapy or does not meet the aesthetic and functional demands of the patient, surgical removal is the treatment of choice. The most widely employed surgical approaches for the treatment of gingival enlargements is gingivectomy or the flap technique.

Mandibular arch 3 months postoperative view after gingivectomy
Conclusion
This report helps to highlight the importance of patient motivation and patient compliance in treatment planning. Oral hygiene education supplemented with positive motivation should be started at the initial stages of the treatment strategy in order to obtain predictable outcomes. At each recall visit, the patient should be notified about their ongoing dental condition and the effects of risk factors like poor oral hygiene, smoking and deleterious habits on the existing oral state. Even though revolutionary advances have taken place in dental specialties, these 2 factors still play a critical role in the success of a therapeutic program. An effective communication is, thus, vital in motivating and educating patients about their dental problems. As a consequence, successful treatment outcome is believed to relate to 2 sides of the same coin, necessitating the combined efforts of both the patient and the clinician.
Footnotes
-
Tanya Jadhav, MDS, is involved in Private practice at Pune, Maharashtra-India. K Mahalinga Bhat, MDS, is a professor at the Department of Periodontics, Manipal College of Dental Sciences. G Subraya Bhat, MDS, is the Head of Department at the Department of Periodontics, Manipal College of Dental Sciences. Jothi M Varghese, MDS, is an associate professor at the Department of Periodontics, Manipal College of Dental Sciences.
-
This study supports the NDHRA priority area, Clinical Dental Hygiene Care: Assess the use of evidence–based treatment recommendations in dental hygiene practice.
- Copyright © 2013 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}