



Abstract
Purpose: The purpose of this preliminary study was to examine the relationship of caries risk, salivary buffering capacity, salivary pH, salivary quality (flow, consistency) and levels of Streptococcus mutans in relation to cigarette smoking.
Methods: This clinical trial consisted of 53 volunteer patients receiving care in a university based dental hygiene clinic. Participants completed a questionnaire specific to their social history in regards to tobacco use, oral health and dietary history. Measurements of unstimulated saliva were collected followed by collection of stimulated saliva samples. These samples were used to measure salivary pH, buffering capacity and Streptococcus mutans levels.
Results: The subject's smoking status was significantly associated with caries risk (p= 0.001), with 25% of the variability of caries risk attributed to smoking. The smoking status was significantly associated with buffering capacity (p=0.025), with 9% of the variability of buffering status attributed to the smoking. Associations between smoking status and salivary pH were not statistically significant. The subject's caries risk was significantly associated with buffering capacity (p= 0.001), with 25% of the variability of caries risk attributed to the buffering capacity. The subject's caries risk was significantly associated with salivary pH (p= 0.031), with 9% of the variability of caries risk attributed to the salivary pH. The Streptococcus mutans test showed no statistical significance (p>0.05) possibly due to the number and low variance in the subjects.
Conclusion: A relationship between caries risk and smoking, buffering capacity and smoking, and stimulated salivary pH and smoking were concluded. No significance difference (p>0.05) between caries risk and salivary pH, salivary quality and smoking, S. mutans and smoking were noted from the preliminary results.
Introduction
Dental caries, a transmissible infectious disease of microbial origin, is mediated by modifiable risk factors. As a result, caries risk assessment is becoming the standard of care. In April of 2002, a consensus conference was held on the topic of Caries Management by Risk Assessment (CAMBRA).1 During the conference, an expert panel created a caries risk assessment tool based upon current literature regarding caries risk factors (disease indicators–bacterial tests, risk factors, protective factors–oral health regimen, supplements and saliva quantity and ability to buffer).1 This tool evaluates 9 risk factors (biological predisposing factors):2,3
Medium or high Streptococcus mutans (S. mutans) and Lactobacilli counts
Visible heavy plaque biofilm on teeth
Frequent snacking between meals
Deep pits and fissures
Recreational drug use
Inadequate salivary flow by observation or measurement
Saliva–reducing factors
Exposed roots
Orthodontic appliances
The tool also assesses saliva in terms of pH (stimulated and unstimulated), consistency and buffering capacity as risk factors for dental caries. The caries risk tool ultimately assists dental professionals in determining low, moderate, high or extreme high caries risk. One factor not recognized as a risk factor for caries, in the CAMBRA model, is cigarette smoking.
There is reasonable evidence that cigarette smoking increases individual's risk for developing caries,4–11 leading some oral health providers to modify the CAMBRA tool to include cigarette smoking as a risk factor.12 Several studies examined the relationship between early childhood caries and parental smoking and concluded there is an association between environmental tobacco smoke and risk of caries among children and adolescents.3,9,13,14 Studies in young adults revealed an association between cigarette smoking and tooth loss resulting from dental caries and plaque scores, and decayed, missing, filled teeth (DMFT) scores were significantly higher in smokers than non–smokers.5,9 Bartoloni examined dental caries in Air Force personnel and reported tobacco use had an elevated risk of developing caries.15 Iida used 1999 to 2004 data from the National Health and Nutrition Examination to examine the oral health status of U.S. women of childbearing age and concluded current smoking was a strong independent risk factor for untreated caries, periodontitis and, to a lesser extent, decayed, missing, filled surfaces (DMFS), and the odds of having poor oral health among previous smokers was slightly higher than in women who had never smoked.7 Lastly, Aguilar–Zinser examined the relationship of smoking of professional truck drivers and reported that, as the number of cigarettes increased, so did the number of large caries.16 These findings were statistically significant.4 Collectively, the evidence suggests smoking is a possible risk factor for caries.
Most of the aforementioned studies examined tobacco use in a narrow group of subjects already at moderate to high risk for developing caries, such as the elderly,8 the U.S. Air Force,15 professional truck drivers in Mexico16 and women of childbearing age.7 Several of the authors used tooth loss, decayed, missing and filled (DMF), DMFS and/or DMFT as the dependent variable,4–9 which is problematic because the point in time when tooth loss or decay occurred cannot be established. Additionally, the severity of periodontal disease was not documented. Therefore, one cannot assume a casual association between smoking and tooth loss, DMF, DMFS and/or DMFT. Prior studies were conducted primarily outside of the U.S. and do not adequately control for external variables that could influence the development of caries.4,6,17 Only 2 recent studies were conducted in the U.S.7,15 Fluoride status was not documented in any of the studies.4–11,15 Additionally, several authors concluded that caries risk status was influenced by co–founding factors such as the socioeconomic status of the subjects,9,15 poor oral hygiene in smokers,5,9,15 younger subjects placing less value on general health,15 mal–distribution of smokers4,6 and having Medicaid or no insurance.7 The pH of saliva has been cited as a likely variable affecting caries risk, reporting an increase of pH while smoking and decrease after smoking.4,17,18 Over long periods of time, smokers have a lower pH in stimulated saliva.19 Buffering capacity was also found to be lower in smokers.20,21
The literature is lacking studies in the U.S. that examine smoking in relation to caries using biologic dependent variables while controlling for co–founding factors. The purpose of this preliminary study was to examine the relationship of caries risk, salivary buffering capacity, salivary pH, salivary quality (flow rate and consistency) and Streptococcus mutans (bacteria associated with dental caries) in relation to cigarette smoking in a sample of adults that had limited co–founding factors.
Methods and Materials
This study was approved by the University of Missouri–Kansas City (UMKC) Adult Health Science institutional review board. This cross–sectional clinical trial used a convenience sample of 53 patients of record seeking dental hygiene care at UMKC School of Dentistry. All 53 subjects voluntarily chose to participate in the study. A total of 77% of subjects were female and 23% were male. The sample was intentionally homogenous to minimize the effects of co–founding variables. None of the subjects were taking medications, had a systemic disease or had undergone radiation treatments that would alter their salivary function. Demographics of the sample are illustrated in Table I. Smoking status in relation to age and insurance status is described in Table II. Smoking status in relation to plaque index and caries protective factors is described in Table III.
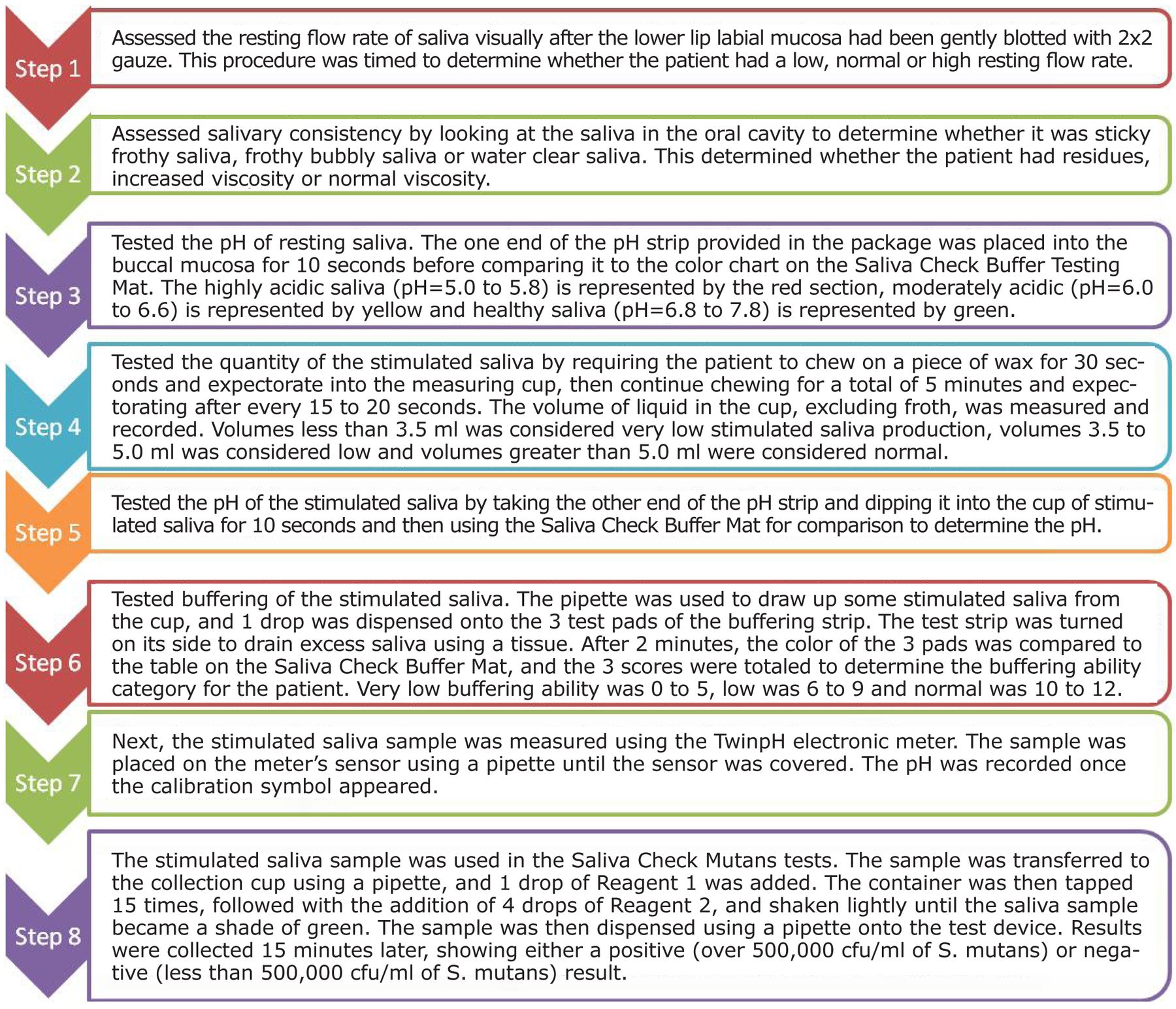
Data regarding each subject's medical history and dental history was assembled from the electronic patient record. Additional data was collected through a written questionnaire focusing on smoking status, the Oral Health Related Quality of Life questionnaire22 and CAMBRA tool. Smoking status was classified as: current smokers, previous smokers, nonsmokers and second hand smoke exposure. The presence of caries was determined during the dental exam by 1 dentist throughout the study. Data was collected by calibrated dental hygiene student clinicians during scheduled clinic sessions as part of the dental hygiene process of care. Saliva quality was determined by examining salivary flow and consistency. Figure 1 outlines the saliva collection procedures. The Saliva–Check Buffer system (GC America, Inc., Alsip, Il) was used to measure stimulated and unstimulated saliva. The Saliva–Check Buffer system was packaged with the following: pH paper strip, measuring cup, dropper, wax and buffer test strip. Saliva–Check Mutans (GC America, Inc., Alsip, Il) was used to measure the presence of S. mutans. The Saliva–Check Mutans system was packaged with the following: wax, dropper, mixing container, reagent 1 and 2, and mutans test device. Accuracy of the Saliva–Check Buffer system was established by using a calibrated electronic pH meter. Both measurements of pH were comparable, therefore validating the Saliva–Check Buffer system.
Demographics (Ethnicity, Age, Insurance Status and Smoking Status)
Smoking Status in Relation to Age and Insurance
Smoking Status in Relationship to Average PI and Daily Fluoride Exposure and Daily Xylitol Exposure
Data was entered into an Excel Spreadsheet and converted to SPSS. Data was analyzed by using the Spearman RHO correlation coefficient. The independent variable was the smoking status. The present study used buffering capacity, salivary pH, flow rate, consistency and Streptococcus mutans as the dependent variables, which provides an accurate picture of the relationship between smoking and caries risk.
Results
Table IV outlines the buffering capacity, salivary pH and salivary quality in terms of individual smoking statuses. Regardless of a subjects smoking status, the pH of stimulated and uanstimulated saliva remained within the healthy range of 6.8 to 7.8. Data revealed nearly all of the non–smokers had normal or high resting flow rates. Data revealed the saliva consistency and saliva quantity was very similar between smoking statuses. There was a variance in buffering capacity depending on the subject's smoking status with smokers having between very low to low status where the non–smokers were between low and normal status.

Saliva Testing Steps
Table V describes the relationship of smoking status with caries risk, buffering capacity and stimulated saliva pH. Data revealed that the subject's smoking status was significantly associated with caries risk (p= 0.001), with 25% of the variability of caries risk attributed to smoking. The smoking status was significantly associated with buffering capacity (p=0.025), with 9% of the variability of buffering status attributed to the smoking. The smoking status and salivary pH were not statistically significant (p>0.05).
Table VI describes the relationship of caries risk with buffering capacity and salivary pH. Data revealed the subject's caries risk was significantly associated with the buffering capacity (p= 0.001), with 25% of the variability of caries risk attributed to the buffering capacity. The subject's caries risk was significantly associated with salivary pH (p= 0.031), with 9% of the variability of caries risk attributed to the salivary pH. The Streptococcus mutans test showed no statistical significance (p>0.05).
Discussion
This appears to be the first study that examines the relationship between biological variables and smoking. The means by which tobacco modifies the caries process and its relationship with availability of saliva in the mouth is still unclear.4,23 Some studies have suggested tobacco leads to transient decline in the availability of saliva in the mouth,4,24 while other studies show that salivary flow actually increases during tobacco use.4,17,25 Saliva pH changes have been cited as variables for modifying caries risk.4 Reports suggest that pH transiently increases while smoking and decreases after smoking, but in some cases it stays at lower levels.4,17 Liede et al indicated that tobacco smokers implicated in dental/oral conditions, such as increased Lactobacilli4,26,27 or Candida albicans and Streptococcus mutans,4,23,25 demonstrated reduced buffering capacity.4 The preliminary results from the present study revealed a relationship between caries risk and smoking as well as caries risk and buffering capacity.
Percentage of salivary quality, buffering capacity and average salivary pH per smoking status
Smoking Status in Relationship with Caries Risk, Buffering Capacity and Stimulated Salivary pH
The validity and reliability of caries assessment tools evaluating pH and buffering capacity of saliva has been well established.28,29 The validity and reliability of chairside Saliva–Check mutans test has not been well established. This study agreed with previous studies regarding the validity and reliability of the Saliva–Check buffer pH readings by comparing with an electronic pH meter. Omori examined the detectability and operability of chairside bacteria testing kits and reported difficulties in accuracy regarding order of measure of the accurate number of bacteria and S. mutans.30 The present study revealed Saliva–Check Mutans system not being statistically significant (p>0.05). In fact, all data looked exactly the same (all negative results or the device did not indicate negative or positive for increase number of S. mutans).4 Investigators question whether or not the test was functioning properly. Further testing to determine the validity and reliability of this chairside test should be conducted by using a standard microbial lab test.
Caries Risk in Relationship with Buffering Capacity and Salivary pH
The present study accounted for the protective factors (fluoride and xylitol) and contributing factors (medications, radiation therapy and systemic disease) where other studies have not included this in the data collection.4,6,8,9,15 Fluoride exposure included toothpaste, mouthwash or living in a fluoridated community. The majority of the subjects exposed to fluoride were the non–smokers, and 4% of the subjects who used xylitol at least 4 times daily were past smokers and non–smokers. Non–smokers had a higher percentage of fluoride exposure compared to current and past smokers, either via toothpaste, mouthwash or living in a fluoridated community.
Regarding contributing factors, none of the subjects in the present study reported taking medications, systemic disease or undergoing radiation therapy that would alter salivary function; therefore, the results from the study were not affected by predisposed xerostomia. This could have impacted the results of the study if subjects did have these contributing factors that resulted in xerostomia due to caries risk for the subjects would be extremely high.2,31–33 A low percentage of non–smoking subjects in the present study reported experiencing dry mouth. None of the subjects who smoked reported experiencing dry mouth. Other components to consider as risk factors for caries include diet, poor oral hygiene care, genetics and socioeconomic status.15,32,34
The present study included plaque index data that revealed smokers had a lower plaque index percentage than non–smokers. This leads the investigators to believe that caries risk was not influenced by homecare. Bartoloni et al suggests caries risk status is probably influenced by the socioeconomic status.15 Graves and Stamm stated that socioeconomic status had a strong influence on the tendency of populations to seek care, with socioeconomic status inversely related to caries experience.15,35 The present study reported a lower percentage of current and past smokers had dental insurance which may be a factor whether a patient who smokes seeks dental care and the impact of the subjects overall oral condition (Table I, II). Future studies with a larger sample size should account for protective and contributing factors as well as oral hygiene regimens.
No significance (p>0.05) between caries risk and the salivary pH were noted from the preliminary results, which we expected due to the small sample size and large number of non–smokers. There have been studies regarding tobacco effects on caries risk, but the data collected from these studies have not utilized salivary pH as part of the assessment tools for determining caries risk.15 This maybe the first study that has collected data regarding salivary pH in relation to smoking and caries risk and if this study had a greater population of smokers the salivary pH may have been of statistical significance.
Determining the subjects smoking status through self–report was a limitation of this study. The investigators have no way of knowing whether or not subjects provided an accurate reflection of their daily habits. Continine is a major metabolite of nicotine and often used to measure the extent of tobacco use and the exposure to the environmental tobacco smoke. Utilization of the detection limit of 0.05 ng/mL in serum continine would have assisted in determining the status between exposure and non–exposure to tobacco smoke.7,36 Future studies should measure serum cotinine to assess smoking status. Another limitation to the study was using a convenience sampling where the majority of the subjects were Caucasian non–smokers. Further studies need to be conducted to encompass a larger subject pool that control for diverse subject population that smoke.
Dental caries is a complex, dynamic, multifactorial process and many factors (disease, risk, protective, contributing) are to be considered when determining a patient's risk factor for caries.2,31–33 There should be strong consideration to include smoking as one of the factors when conducting a CAMBRA due to the evidence presented within various studies which indicates smoking has an effect on the oral cavity.6–9,15
Conclusion
Within the limitations of the preliminary study on the relationship of buffering capacity, salivary pH, salivary quality and S. mutans in relation to cigarette smoking, the following can be concluded:
A relationship exists between caries risk and smoking.
A relationship exists between buffering capacity and smoking.
A relationship exists between stimulated salivary pH and smoking.
There is not a relationship between salivary quality and smoking.
There is not a relationship between smoking status and S. mutans.
Footnotes
-
Marsha A. Voelker, CDA, RDH, MS, is an assistant professor at the Division of Dental Hygiene University of Missouri–Kansas City School of Dentistry. Melanie Simmer–Beck, RDH, MS, is an associate professor at the Division of Dental Hygiene University of Missouri–Kansas City School of Dentistry. Molly E. Cole, RDH, BS, is a graduate of the Division of Dental Hygiene University of Missouri–Kansas City School of Dentistry. Erin Keeven, RDH, BS, is a graduate of the Division of Dental Hygiene University of Missouri–Kansas City School of Dentistry. Daniel Tira, PhD, is a retired professor from the University of Missouri–Kansas City School of Dentistry.
-
This study supports the NDHRA priority area, Clinical Dental Hygiene Care: Investigate how dental hygienists identify patients who are at–risk for oral disease.
- Copyright © 2013 The American Dental Hygienists’ Association





{kind=link}