



Abstract
Purpose: Dental professionals suffer from a high prevalence of work-related musculoskeletal disorders (MSD). Dental hygienists in particular have a high prevalence of pain in the forearms and hands. The objective of this study was to compare 1 cordless handpiece to 2 corded handpieces during simulated tooth polishing in terms of the muscle loads (recorded as electromyography (EMG) activity), duration of polishing procedure, and dental hygienist opinion about ease of use.
Methods: EMG was used to quantify muscle electrical activity of 4 forearm muscles during simulated dental polishing with 2 corded handpieces (HP-A and HP-B) and 1 cordless handpiece (HP-C). A convenience sample of 30 dental hygienists (23 to 57 years of age) with 1 to 20+ years of clinical practice experience completed the study. Each participant spent approximately 5 minutes polishing 3 predetermined teeth in each of the 4 quadrants. The sequence of the handpieces was randomly assigned. At the end of the study, participants completed a subjective end user evaluation of handpiece preference.
Results: Muscle activity levels of 10th, 50th and 90th percentiles did not differ significantly between the 3 handpieces tested (p>0.05). However, total muscle workload (integrated EMG) was lowest for the cordless handpiece (HP-C), but this was only significantly less than HP-A (p<0.05). Polishing using the cordless handpiece (HP-C) (M=257 seconds, SD=112 seconds) took significantly less time than either the HP-A corded (M=290 seconds, SD=137 seconds) or HP-B corded handpiece (M=290 seconds, SD=126 seconds) (p<0.05). Overall, 50% of the study participants preferred the cordless handpiece, 37% preferred HP-A and 13% preferred HP-B (p<0.05).
Conclusion: Use of the cordless handpiece reduced the duration of polishing, which in turn led to less total muscle activity, but not muscle intensity. Overall, dental hygienists preferred the cordless handpiece.
Introduction
Musculoskeletal disorders (MSD) are a significant problem for the dental profession.1,2 A high prevalence (64 to 96%) of dental professionals report having musculoskeletal pain or discomfort in a 12 month period, indicating that much of these MSD are work related.3-7 General practice dentists commonly experience pain in the back (35 to 60%), wrists and hands (34 to 54%), neck (20 to 57%) and shoulders (21 to 53%).8-11 Dental hygienists often demonstrate higher prevalence for these same regions: wrists and hands (64 to 70%), shoulder (60 to 68%), neck (54 to 69%) and back (24 to 67%).4,6,8 Variation in these reported rates between studies may result from different data collection techniques or different occupational responsibilities around the world.1,2 Of particular focus is the finding of a high prevalence of pain in the wrists and hands of dental hygienists. Previous research has revealed that dental hygienists have one of the greatest risks of developing the MSD carpal tunnel syndrome (CTS) compared with other professions,12 with 7 to 8.4% receiving the clinical diagnosis of CTS and 44.2% displaying at least one symptom of CTS.4,13,14 Evidence shows that CTS and other MSD cause significant impact on dental hygienists and may lead to reduced productivity or performance, or even to decreased working hours and change of profession.5,13
The incidence and location of pain match findings of a recent study which recorded significant physical workload in the neck, shoulders and wrists/hands of dental hygienists performing their regular duties.15 Holding instruments at a patient's mouth and far from the dental hygienist's own body places large force moments at the shoulders, while leaning the head or torso away from a neutral position increases force moments at the neck and back, respectively. These force moments can be minimized by appropriate body postures. However, the repetitive procedures of hand scaling and tooth polishing for approximately 21 minutes of an average 50 minute appointment places a large load on the muscles and tendons of the wrists and hands.16 Precise movements require dental hygienists to hold body positions and accurately control the location and force application of different instruments. Ergonomic design improvements to instruments hold the promise of reducing the workload on wrist and hands, but research is needed to determine whether dental instruments achieve these goals.
Currently, the most accurate technique to quantify muscle workload of operating a dental instrument is to record the electrical activity of muscles through electromyography (EMG).15,17 Electrodes placed on the surface of the skin over the belly of a muscle detect a summation of the action potentials (small voltages produced when muscles are activated). The greater the voltage the more the underlying muscle is being activated to generate force. Intensity, duration and frequency of activity are all important considerations for the potential development of MSD.17 Recording EMG during a procedure allows the intensity of muscle workload to be determined and the duration can also be readily measured. The total muscle activity is determined by intensity x duration. By quantifying and comparing the intensity and duration of electrical activity between dental tools with different design characteristics, researchers can determine which instruments cause the greatest or lowest muscle load. Frequency of a procedure would be expected to remain constant. Researchers have begun to determine the relevant ergonomic factors in dental instruments by using EMG to measure activity of muscles in the forearm which control movements at the wrist, fingers and thumb.18 Research has revealed that mirrors, which are lightweight and have soft and wider diameter handles, reduce muscle loads.19 Scaling instruments with a handle diameter of at least 10 mm, a mass of 15 g or possibly less, and a round and tapered shape lead to the lowest activity of muscles of the forearm.20,21 However, there is still much research and development of equipment needed to provide optimum instruments to minimize work related MSD in the dental profession.
One ergonomic concern is with the use of handpieces that require hoses or cords. Hoses or cords add weight to an instrument. They also create cord drag where additional resistance to motion is likely to increase muscle workloads. While development of the swivel hose mechanism has greatly improved handpiece ergonomics, the ideal handpiece would have the ability to easily rotate and move effortlessly while performing the intended function. Recent technological advances have allowed for the development of cordless handpieces. Therefore, the objective of this study was to compare 1 cordless handpiece to 2 corded handpieces during simulated tooth polishing in terms of the muscle loads (recorded as EMG activity), time involved to complete standard procedures and dental hygienist opinion about ease of use. Studies such as this provide a scientific approach to determining which ergonomic factors reduce muscle loads and have the potential for reducing the incidence of work related MSD in the dental profession.
Methods and Materials
Practicing dental hygienists (n=30) of varying ages and length of employment participated in an institutional review board approved controlled clinical trial. Participants were recruited by distribution of an invitation letter sent to licensed dental hygienists in the Hampton Roads region. An initial phone screening of interested individuals was conducted to determine eligibility. In order to control for certain limitations, individuals with a dominant left hand were excluded, as well as individuals with history of surgery, injury or disability of the working hand, wrist, forearm or shoulder, or diagnosis of CTS. Strenuous arm muscle activity such as tennis and chopping wood were prohibited for 2 days prior to data collection to control for muscle strains. No attempt was made to control for variations in forearm muscle size among participants. Each participant served as their own control. Data was collected in one visit (lasting approximately 45 minutes) at the Dental Hygiene Research Center on the campus of Old Dominion University.
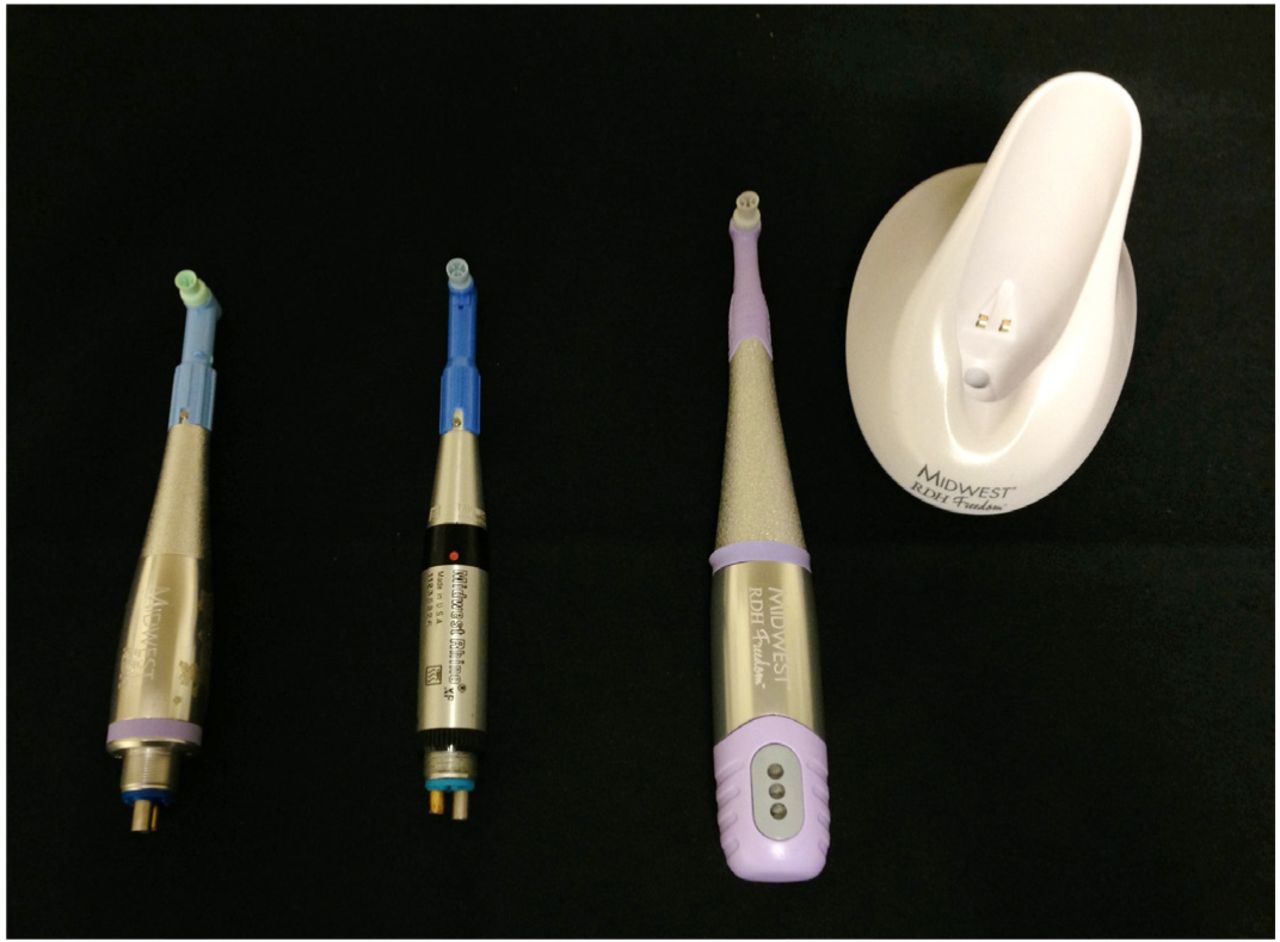
In a simulated oral polishing setting, 3 low speed handpieces were evaluated on forearm muscle activity that reflected load or force on the lower portion of the arm and hand. The handpieces tested were as follows: HP-A (corded), HP-B (corded) and HP-C (cordless) (Figure 1). The model names, handpiece masses and grip diameters are presented in Table I.
After informed consent was obtained and EMG equipment was connected, each individual polished selected teeth using all 3 handpieces, in the order determined through simple randomization. Dental chair-mounted typodonts (Kilgore International, Inc) equipped with an artificial face were used to simulate the oral cavity (Figure 2). For each handpiece a typodont, dpa and prophy paste was provided. Each typodont had artificial brown stain placed on the facial and lingual surfaces of 3 predetermined teeth in each quadrant (3, 4, 7, 11, 12, 15, 19, 20, 24, 25, 29, 30). This experimental set-up provided a simulated polishing experience in all areas of the mouth and maintained consistency across the handpieces tested.

Experimental Handpieces
From left to right: Corded HP-A; Corded HP-B; Cordless HP-C (Dentsply, International, York, Penn.)

Simulated Polishing Set Up
Pictured: Mannequin, typodont and participant with EMG electrodes attached to skin over 4 muscle sites for recording electrical activity of muscles.
Handpiece Specifications
Prior to study initiation, participants were familiarized with both the EMG and polishing equipment. To standardize polishing procedures, participants were provided with written and oral instructions for neutral body positioning and were instructed to polish all surfaces of assigned teeth utilizing their normal polishing procedures, thus applying typical pressure and techniques. Each individual spent approximately 5 minutes polishing with each handpiece, although no time limits were placed on participants. To minimize the effects of fatigue, participants were allowed to rest for 1 to 2 minutes in between polishing sequences.
At the completion of the polishing sessions, participants completed an evaluation of handpiece diameter grip, balance, maneuverability, weight and noise level, utilizing a 5-point Likert scale (not comfortable to very comfortable), as well as responded to 5 opened ended questions related to handpiece preference.
EMG Procedure
EMG was used to record the electrical activity of 4 muscles (Figure 2) involved in high pinch forces and studied in previous dental research: flexor digitorum superficialis, flexor pollicis longus, extensor digitorum communis and extensor carpi radialis brevis.20,21 Participants washed their right forearm with regular soap and warm water to remove skin oils and lotions. The location for placement of the electrodes was determined using standard procedures and then these areas were wiped with alcohol and allowed to dry.22 Noraxon dual Ag/AgCl snap electrodes (Scottsdale, AZ), with 1 cm active areas and 2 cm inter-electrode distance, were placed over the belly of each muscle in parallel with the direction of the muscle fibers. A ground electrode was placed on the lateral epicondyle of the right arm. The action potentials produced by the muscles create voltages across the surface electrodes which flow along cables to a telemetry unit which then transmits the signal at 1,500 Hz to a Noraxon TeleMyo 2400T G2 wireless data acquisition system (Scottsdale, AZ). The location of the electrodes was checked with muscle function tests and changes were made if necessary. The electrodes and cables between the electrodes and telemetry unit were fastened down with non-allergenic tape to avoid movement artifact. Once the EMG equipment was set up correctly, participants performed maximum voluntary isometric contractions for each muscle separately, which were recorded for 3 seconds each. For each handpiece, EMG was recorded from the beginning to the end of polishing. The time of the EMG record was the trial duration. The raw EMG signals were rectified and filtered using a second order Butterworth filter with 10 Hz high pass cutoff frequency. The EMG was integrated (area under the voltage-time curve) to obtain a measure of total muscle activity across a polishing trial. Data from the polishing trials was also normalized by determining its percentage of maximum voluntary isometric contractions before determining the 10th, 50th and 90th percentile of the EMG signal for each of the 3 handpiece trials.
Group Mean and Standard Deviations for 10th, 50th and 90th Percentile Levels of Activity for the Flexor Digitorum Superficialis, Flexor Pollicis Longus, Extensor Digitorum Communis and Extensor Carpi Radialis Brevis Muscles During Polishing With 3 Types of Handpiece
Data Analysis
EMG measures, trial duration and quantitative survey responses were entered into SPSS 19. EMG measures and trial duration were analyzed using repeated measures multivariate analysis of variance (RMANOVA) with 3 levels of handpiece. Planned simple contrasts compared the cordless handpiece with 2 corded handpieces. A chi-square test was employed to detect significant differences in preference between the handpieces. Survey ratings for handpiece properties of diameter, balance, maneuverability and weight were compared between the cordless and the corded handpieces using Wilcoxon signed-rank tests. The level of significance was set at p<0.05. Open ended questions in the survey were tabulated by recording the frequency of occurrence across the participants.
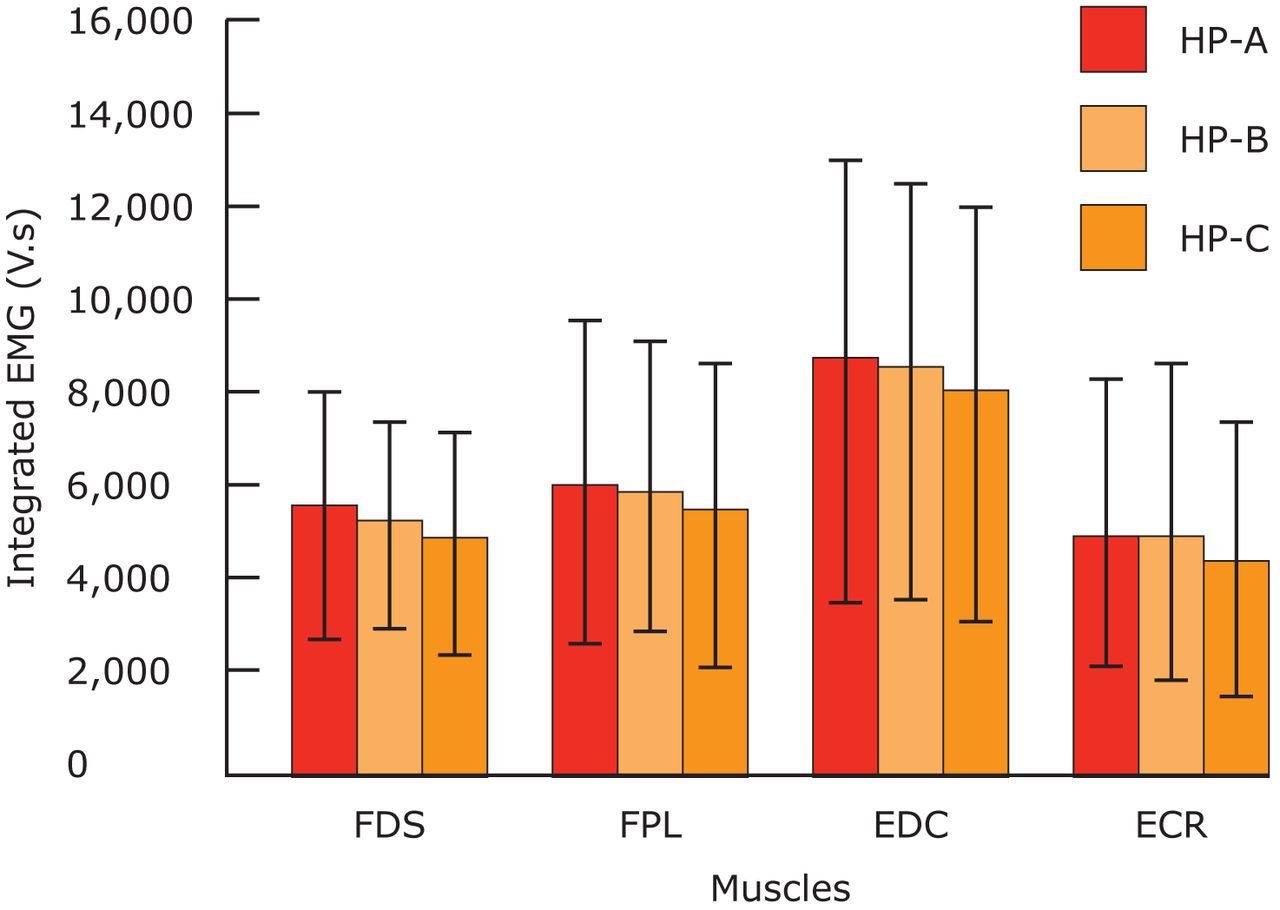
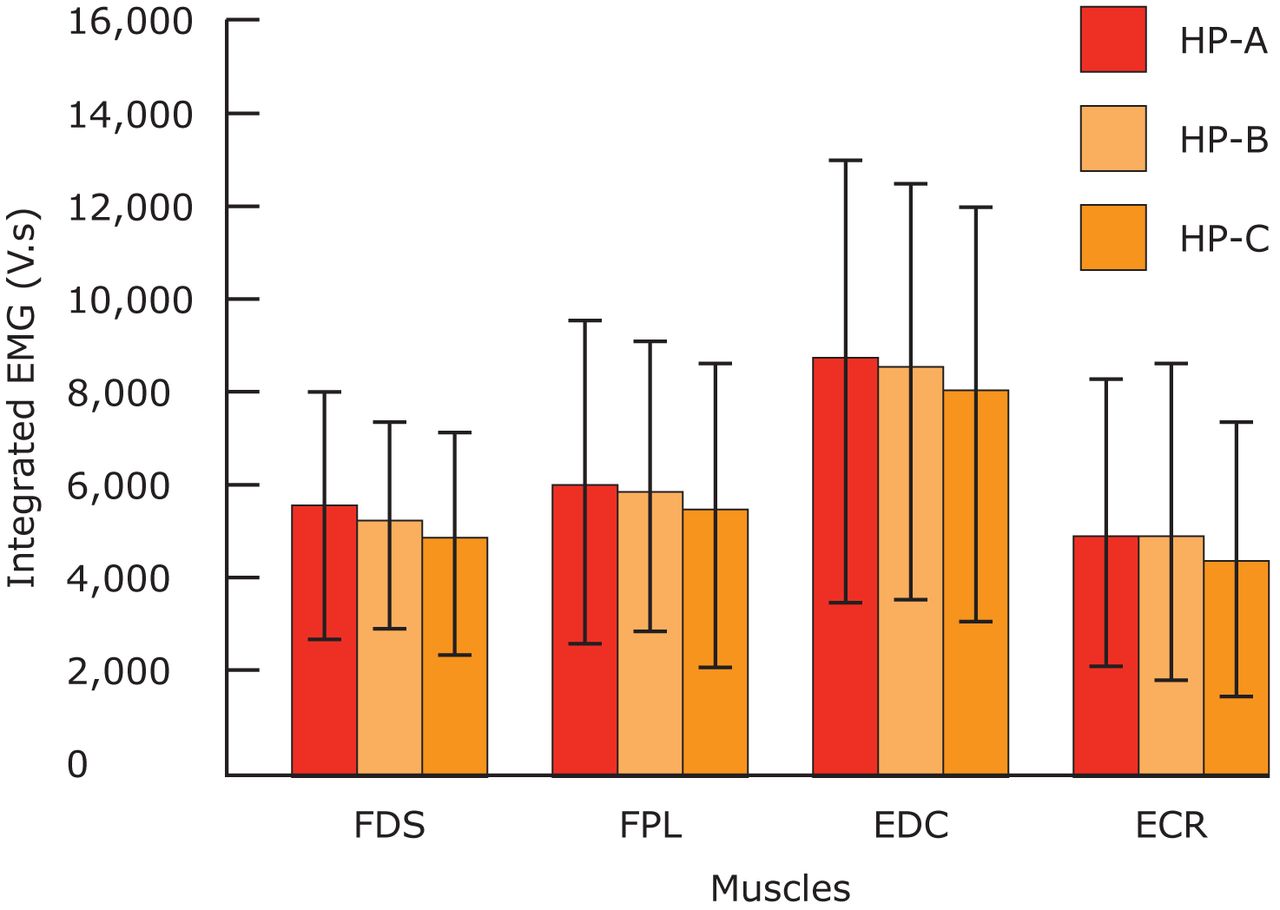
Integrated EMG (Means and Standard Deviation Error Bars) of the 4 Muscle Sites for Polishing With the 3 Different Handpieces (Corded HP–A, HP–B and Cordless HP–C)
Integrated EMG is the area under the rectified voltage-time (V.s) curve, which quantifies total muscle activity. The 4 muscles are: flexor digitorum superficialis, flexor pollicis longus, extensor digitorum communis and extensor carpi radialis brevis. The cordless handpiece (HP-C) resulted in significantly lower integrated EMG for the flexor digitorum superficialis, extensor digitorum communis and extensor carpi radialis brevis muscles (p<0.05).
Results
Thirty female subjects between the ages of 23 to 57 years, with a mean age of 37.7 years, completed the study. All participants were employed at least 3 full days per week and had clinical practice experience between 1 to 20+ years: 1 to 5 years (30%), 6 to 10 years (33%), 11 to 15 years (17%) and 16+ years (20%). Twenty-nine participants reported that they routinely conducted full-mouth polishing, while 1 respondent reported that selective polishing was provided.
Mean and Standard Deviation of Survey Handpiece Comfort Ratings for Grip Diameter, Balance, Maneuverability and Weight
Results from Question 3 of the Survey - What Would You Change about Preferred Handpiece?
Results from Question 2 of the Survey - What Did You like Most about Your Preferred Handpiece
Muscle activity levels (10th, 50th and 90th percentiles) did not vary significantly between the 3 handpieces for any of the muscles tested (p>0.05) (Table II). Mean total activity (integrated EMG) of the flexor digitorum superficialis, flexor pollicis longus, extensor digitorum communis and extensor carpi radialis brevis muscles were lower for the cordless than the corded handpieces (Figure 3). RMANOVA indicated significant effects for the flexor digitorum superficialis and extensor digitorum communis muscles (p<0.05), but not the flexor pollicis longus (p=0.18) and extensor carpi radialis brevis (p=0.08) muscles. Simple planned contrasts revealed that the cordless handpiece led to significantly less total activity than the corded HP-A for the flexor digitorum superficialis, extensor digitorum communis and extensor carpi radialis brevis muscles (p<0.05), but not the flex- or pollicis longus (p=0.06). The effect of order was assessed using RMANOVA and Bonferroni post hoc tests. Only the extensor digitorum communis muscle revealed a significant order effect, with the third procedure employing greater 50th percentile activation than the second trial (p<0.05).
On average, polishing using the cordless (HP-C) handpiece (M=257 seconds, SD=112 seconds) took over 30 seconds less time than with either the HP-A corded (M=290 seconds, SD=137 seconds) or HP-B corded (M=290 seconds, SD=126 seconds) handpieces. The RMANOVA revealed a significant effect of handpiece on polishing duration (p<0.05) and simple planned contrasts revealed that using the cordless handpiece led to statistically significantly shorter polishing times than the 2 corded handpieces (p<0.05). There were no significant differences in duration based on the order the handpieces were used (p>0.05).
Handpiece Design and Preference
A chi-square analysis revealed significant differences (p<0.05) in overall handpiece preferences with 50% (n=15) of the study participants preferring the cordless handpiece (HP-C), 37% (n=11) preferring the corded HP-A and 13% (n=5) preferring the corded HP-B. The survey ratings for diameter, balance and maneuverability were not significantly different between the cordless and corded handpieces (p>0.05) (Table III). However, the weight of the cordless HP-C was rated as significantly more comfortable than the HP-A (p<0.05) (Table III). When participants were asked what they would change about their preferred handpiece, weight/balance, noise level, diameter/grip and cord were cited as common factors (Table IV). Table V reveals that respondents liked the cordless handpiece because it lacked a cord and also because it was light weight, balanced and quiet. Fifty-seven percent felt the cordless handpiece produced sufficient power throughout the procedures. Subjective comments by the dental hygienists emphasized the freedom of movement, lack of cord resistance, lightweight and low noise level of the cordless handpiece as important factors in determining their preferred experimental handpiece.
Discussion
Dental professionals have a high rate of MSD.1-7 Dental hygienists are especially susceptible to pain in the wrists and hands.4,6,8 While ergonomically appropriate postures can minimize force moments on the body, the nature of performing repetitive movements, such as hand scaling and polishing, places high workloads on the muscles and tendons of the forearms and hands. Ergonomically designed instruments offer the possibility of reducing the workload and minimizing the risk of developing work related MSD. Workload on the muscles can be quantified through recording the electrical activity of muscles (EMG).15,17 EMG research studies have only just begun to determine the characteristics of dental instruments that minimize muscle workload.20,21 For the first time, this study examined whether a cordless handpiece, which in principal could reduce the effects of cord pull, reduces intensity and duration of muscle activity of the forearm and hand during dental polishing compared with two standard, corded handpieces.
Polishing teeth with the cordless handpiece reduced the duration, but not the intensity of the muscular workload compared with the 2 corded handpieces. The EMG intensity distribution remained the same across handpieces as revealed by no significant changes to the 10th, 50th or 90th percentile levels of muscle activity. However, using the cordless handpiece reduced the integrated EMG of 3 out of 4 muscles, that is the total work (intensity x duration). These findings can be explained by the, on average, 30 second reduction in polishing time when using the cordless handpiece (HP-C) compared with the 2 corded handpieces (HP-A and HP-B). This difference in time cannot be readily explained by worse polishing performance. It is important to realize that 30 seconds is 20% of the average polishing time for only 12 teeth, hence a larger reduction in duration would be expected for polishing all the teeth, which most dental hygienists tested reported they do. Intensity, duration and frequency of activity are all important factors in the development of MSD.17 This research reveals that the cordless handpiece impacts the workload dose by decreasing duration, but not intensity of muscle activity, and would not change frequency. Unfortunately, the development of MSD is multi-factorial and varies greatly across individuals, therefore we cannot definitively state the workload dose that avoids MSD.15,17 Clearly, there is a need for future research to establish safe workloads and clinically meaningful changes in workload dose. Until these factors are determined it remains important to find ways to reduce workload during activities that have a high incidence of MSD.
The cordless handpiece was preferred most (50%) by the dental hygienists in spite of the fact that the participants were more familiar with the other handpieces and none had any prior experience with the new cordless handpiece. The lack of a cord, weight and balance, and low noise were listed as the main reasons for preferring the HP-C handpiece. While the other handpieces are lighter than the cordless, the hose adds to the weight and can impact the balance of the device. The larger diameter of the cordless handpiece to the corded handpieces is unlikely to be the cause of reduced total muscle activity, although some dental hygienists did prefer the larger diameter. All handpieces tested here had diameters greater than the criterion of 10 mm, found to minimize muscle activity during a previous EMG study of scaling instruments,20,21 and handpiece diameter would be expected to influence muscle activity levels not necessarily the polishing time. Dental hygienists like using a polishing device without a cord, which appears to translate to shorter polishing duration, but not lower muscle intensity.
This study was the first to examine whether a cordless handpiece influenced muscle activity, polishing duration and dental hygienist opinion compared with corded handpieces. There are several limitations that impact the applicability of this research. The 3 handpieces were provided by one company and varied on several characteristics in addition to how they were powered. Future research could examine a broader range of handpieces to separately analyze different device properties. Dental hygienists were recruited using a convenience sample, rather than being randomly sampled from the population. There is also a need to develop a valid questionnaire for assessing dental professionals' opinions of dental equipment. Further research is needed to identify the workload dose and individual characteristics that lead to MSD in dental hygienists.
Conclusion
Within the limitations of the current study, the cordless handpiece did not influence muscle intensity (p>0.05), but decreased the overall muscle workload (p<0.05) by reducing polishing duration (p<0.05). The cordless handpiece was preferred over the corded handpieces by the dental hygienists who participated in the study (p<0.05). Future research is needed to determine whether these changes impact the development of MSD.
Acknowledgments
The authors would like to thank Kyle Kelleran, Amy Marsh, Maricel Navarro, Scott Sechrist and Debbie Williams for their assistance with data collection.
Footnotes
-
Gayle McCombs RDH, MS, is a University Professor, Graduate Program Director and Director of Dental Hygiene Research Center in the School of Dental Hygiene, Old Dominion University. Daniel M. Russell, PhD, is an Assistant Professor in the School of Physical Therapy and Athletic Training at Old Dominion University.
-
This study supports the NDHRA priority area, Occupational Health and Safety: Investigate the impact of exposure to environmental stressors on the health of the dental hygienist (aerosols, chemicals, latex, nitrous oxide, handpiece/instrument noise).
-
Disclosure
This project was supported by Dentsply Professional.
- Copyright © 2014 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}