



Abstract
Purpose: The purpose of the study was to assess the knowledge, education, attitudes, confidence, and practice of dental hygienists providing dental care to adult patients with dental anxiety (DA).
Methods: A purposive sample of dental hygienists, using a snowball sampling technique, were recruited through social media sites. Inclusion criteria were limited to actively practicing, registered dental hygienists in the United States (U.S.). The validated survey had 29 questions regarding dental hygienists' knowledge, education, attitudes, confidence, and practice in regards to patients with DA. Regression analysis and chi square tests were performed on the data with research outcomes represented through frequency tables and percentiles.
Results: A total of 417 participants attempted the survey; 355 participants (n=355) completed the survey yielding a participation rate of 87%. A majority, 73%, of the respondents reported DA as a “somewhat serious” to “extremely serious” issue when treating patients. Forty-eight percent of the respondents indicated that their education had prepared them to address DA but also reported the need for additional education in this area. Dental hygienists indicating higher levels of confidence in addressing DA in their patients also allowed for extra time in their schedules to treat patients with DA.
Conclusion: Increased DA education in the undergraduate dental hygiene curriculum as well as post-graduate education opportunities may increase dental hygienists' confidence and capability in the management of DA.
Introduction
Odontophobia, or dental anxiety (DA), is a psychosomatic condition1 causing anxiety related to prior pain and/or distressing emotional responses during dental treatment.2 Dental anxiety is defined as a fear and extreme anxiety towards dental stimuli marked by distress, poor compliance, or avoidant behavior towards regular dental appointments, which ultimately may influence overall health.3-8 This anxiety may also influence the individual's prevention regimen including self-care and maintenance.3,9,10 Dental anxiety may also impact general health by triggering emotional and physical symptoms including: negative thoughts and feelings,11 general anxiety and depression,12 overuse of medications, recurrent sleep disturbances, unexplained pain, and poor social and occupational functioning.13,14 Individuals who avoid dental care may also be at increased risk for systemic diseases including diabetes and cardiovascular disease.15
Dental anxiety affects 10-20% of adults in the United States (U.S.).2,16-19 An estimated 5-10% of the adult population in the U.S. avoids seeing the dentist20 and one out of ten U.S. adults do not visit the dentist due to DA.21 Dental phobia is a more severe form of DA that may profoundly affect a person's overall health.7,13,14,22-24 Dental phobia leads to higher rates of avoidant behavior and decreased quality of life (QOL).7,22-24 The most severe forms of DA require treatment by a specially trained psychologist.22,25 Control of DA is also critical in the prevention and development of dental phobia.25,26
Dental anxiety can be caused by certain dental stimuli (extractions, sounds, emotions, etc.), two or more previous traumatic dental experiences,3,27 and the relayed experiences of others.27 Dental anxieties can also be triggered either before or during a dental hygiene appointment.28 Procedures including polishing, periodontal probing, manual and ultrasonic scaling, and local anesthesia are known to trigger DA.29 Among all triggers, the administration of local anesthesia, is reported to be the most anxiety provoking dental hygiene procedure.3,29,30
Oral health care providers need to understand the origin of a DA in order to select the appropriate DA management technique to provide optimal patient care27,31 Validated DA screening tools are available to assist the provider in recognizing the severity of the DA.12 Dental hygienists can identify DA triggers through the use of anxiety screening tools such as State Form of the State-Trait Anxiety Inventory (STAI), 3,28 Marks-Sheehan Phobia Scale,3 Dental Fear Survey (DFS), 32 Dental Anxiety Scale (DAS), or by simpling asking the patient about their dental fears.29
A variety of management techniques are available to help with DA patients, and oral health care professionals should be educated in these techniques for the provision of optimal patient care.33 Management techniques include cognitive behavioral therapy (CBT), relaxation therapy, computer-assisted relaxation learning (CARL), hypnotherapy (HT), group therapy (GT), individual systematic desensitizing (ISD), pre-medication, flooding (implosion), and swallowing relaxation.27 CBT teaches patients skills in modifying their thinking and behavior; relaxation therapy and hydrotherapy eliminate tension in the body and reduce stress; CARL is a computer program designed to reduce a patient's fear of injections, and pharmacological management.27 Some of these management techniques may have a lasting effect, however, they must be delivered by specially trained individuals such as licensed psychotherpaits.34-36
Previous research studies regarding dental practitioners and their understanding of DA, have identified a lack of prior in-depth DA education,33,37-39 along with a need for more DA training in both undergraduate and graduate education programs.33,37,39,40 Research has shown that dental providers were better equipped to address anxiety in a patient after receiving prior training in DA during undergraduate or post-graduate education.38,41 Coursework in the area of DA has been shown to increase attentiveness to the prevention and control of dental fear development, resulting in increased levels of confidence among dentists when treating patients with DA.38 Additional studies of dentists indicate a desire and willingness for more post-graduate courses to compensate for their lack of undergraduate education regarding DA 33,37 Provider anxiety was also experienced by dentists treating patients with DA.33,42 Research conducted with practicing dental hygienists also indicates the need for more education in the area of DA as part of the dental hygiene curriculum.39,41
Previous studies have suggested that general dental practitioners are ineffective in managing patients with DA43 due lack of expertise,40,44 lack of confidence,40 and inadequate education33,45 and training.40,44 Additionally, both the patient and the provider may experience anxiety when a patient presents with DA.33,40 However, studies have shown that providers who have gained experience in treating patients with DA, are able to decrease anxiety levels for both the patient and for themselves.33,40,45 A review of the literature shows a lack of recent research regarding associations between dental hygienists' experience and education in the area of DA. The purpose of the study was to assess the knowledge, education, attitudes, confidence, and practice of dental hygienists when providing dental care to adult patients with DA and to evaluate the need for more formal education on anxiety in dental hygiene curricula.
Methods
This study was approved by the MCPHS University Institutional Review Board (IRB) and was assigned IRB protocol number 050917G. An exploratory, cross-sectional survey design was chosen, using a purposive and snowballing sampling technique (n=417) via dental hygiene related social media sites across the U.S. to access a large population of dental hygienists at minimal expense. Snowballing technique was employed to increase the study population and to target and recruit dental hygienists who were current members of these social media sites. The Facebook sites accessed included: “Dental Hygiene Network”, “RDH,” “Dental Hygiene Life with AndyRDH,” “UNE Dental Hygiene Program,” “Maine Dental Hygienists' Association,” “Dental Hygienist Talk,” “Massachusetts Dental Hygienists Connect,” “RDH-netWORK,” “Dental Hygiene with Kara RDH,” and “Dental Hygienists are Awesome.” A target participation rate of 152 participants, determined through a statistical power analysis, was sought to in order to generalize the results. Inclusion criteria were limited to actively practicing registered dental hygienists (RDHs) in the U.S.
Survey Instrument
The instrument used was a modified web survey developed from the previous work of Brahm et al. and Armfield et al.33,37 Permission was granted by the respective authors to use a modified form of the surveys. Participant knowledge was measured regarding DA patient management techniques, confidence in treating patients with DA, and the participant's ability to supplement their lack of knowledge in DA. The modified survey was comprised of 29 questions with dichotomous, 5-point Likert scale, and fill-in-the-blank questions. The Likert scale questions offered response choices ranging from “always” to “never.” Questions collected demographic information, the participant's dental anxiety knowledge/attitudes about DA, and the participants' DA practices. The last section of the survey included an open-ended question, allowing for the opportunity to share additional information.
The survey was validated prior to data collection with a content validity index (CVI). A panel of 6 dental professionals rated each question according to its relevance, CVI outcomes were averaged and set to 83%.46 Questions scoring below 83% were deleted. The expert panel also provided comments and their rationale, and final revisions were made.
Data Collection
An introduction to the study was posted on the selected social media websites, and a survey link was provided. Participants were asked to share email contact information for additional prospective participants meeting the inclusion criteria. An invitation and survey link, was sent by email to the potential participants to help increase the participation rate. The invitation and survey link were reposted twice weekly through the data collection period to increase participation. The opportunity to receive a $100 Amazon gift card was offered as an incentive for survey completion; and a participant's name was randomly drawn at the close of the study. Data collection was carried out over a 30-day period.
The password protected data was imported into the IBMÒ STATA/SPSS software; only surveys completed in full were included in the analysis. Data was analyzed using both a chi-square test and regression analysis, with results represented through frequency tables and percentiles. Demographic information and variables of interest were examined for statistical assumptions, including normality of all summary statistics. The chi-square test of independence was used to determine whether significant relationships existed between the variables of interest. The phi coefficient was calculated for all significant chi-square tests to demonstrate the effect size of the relationship (small=0.1, medium=0.3, and large=0.5). A Bonferroni correction was used for all tables larger than 2x2 to control for familywise error. Ordinal regression was employed to examine age, years in practice, confidence, and provider anxiety while caring for anxious patients as predictors of practice behaviors.
Results
A total of 417 participants attempted the survey; of those potential participants, 355 (n=355) completed the survey, resulting in a participation rate of 87%. The average age of the study population was 41 years (SD 12.68). The vast majority, 99.7%, of the participants were female, 85% were employed in a general dentistry practice, and 59% reported their highest level of education was an associate's degree. The average number of years participants were actively practicing was 15 (SD 12.84) and the 69% were certified to administer local anesthesia. Participants saw an average of 29 adult patients per week (SD 10.44) while the average number of adult patients with DA per week was 7.59 (SD 6.72). The average number of adult patients experiencing DA during routine prophylaxis per week was reported to be 20 (SD 19.96). Descriptive demographic information is shown in Table I.
Demographics Descriptive Statistics (n=355)
Most participants, 73%, reported DA to be a “somewhat serious” to “extremely serious” issue while treating patients. Of these respondents, 72% felt a need for more formal education on anxiety issues during their dental hygiene education. Thirty-eight percent of participants did not feel prepared to treat patients with DA. Just over half, 57%, of dental hygienists reported experiencing personal anxiety while treating patients with DA. The majority, 99%, did not report using one of the published screening tools for DA, and 67% reported not using a screening tool due to the lack of knowledge about these tools. Sixty-three percent of participants reported “sometimes” to “never” asking patients about DA when reviewing the medical history, while 37% of participants stated that they “often” or “always” ask about DA. A little more than one third, 37%, of the respondents reported “sometimes” allowing extra time for patients with DA, followed by 20% indicating “often,” and 19% who “rarely” allow additional time.
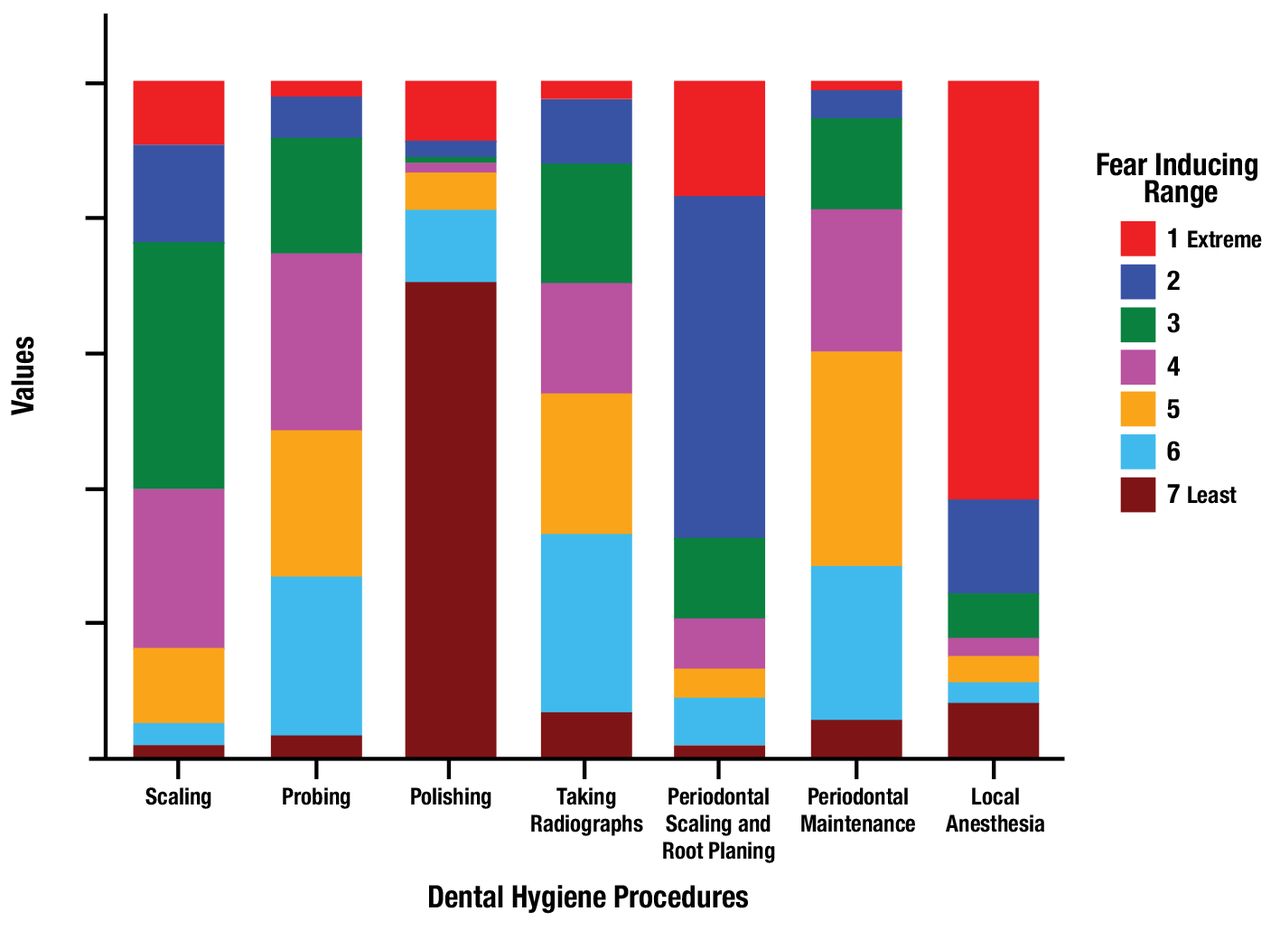
Respondents indicated that most feared dental hygiene related procedure was the administration of local anesthesia (62%) while polishing was rated the least DA-provoking hygiene procedure (71%) Respondents ranking of fear inducing dental hygiene procedures are displayed in Figure 1.
Despite the participants' acknowledgement of dental hygiene procedures known to produce fear and anxiety for patients, 43% of the respondents reported they felt very confident treating patients with DA. The majority of participants, 74%, were knowledgeable in the use of nitrous oxide sedation and 68% were familiar with distraction to manage patients with DA. Nitrous oxide sedation (59%) was the DA management technique used by over half the dental hygienists trained in its use. Most of the dental hygienists reported performing prophylaxis on adult patients with the use of nitrous oxide (64.2%) and about half (49.3%) used distraction. Dental hygienists' knowledge of DA management techniques is shown in Table II.
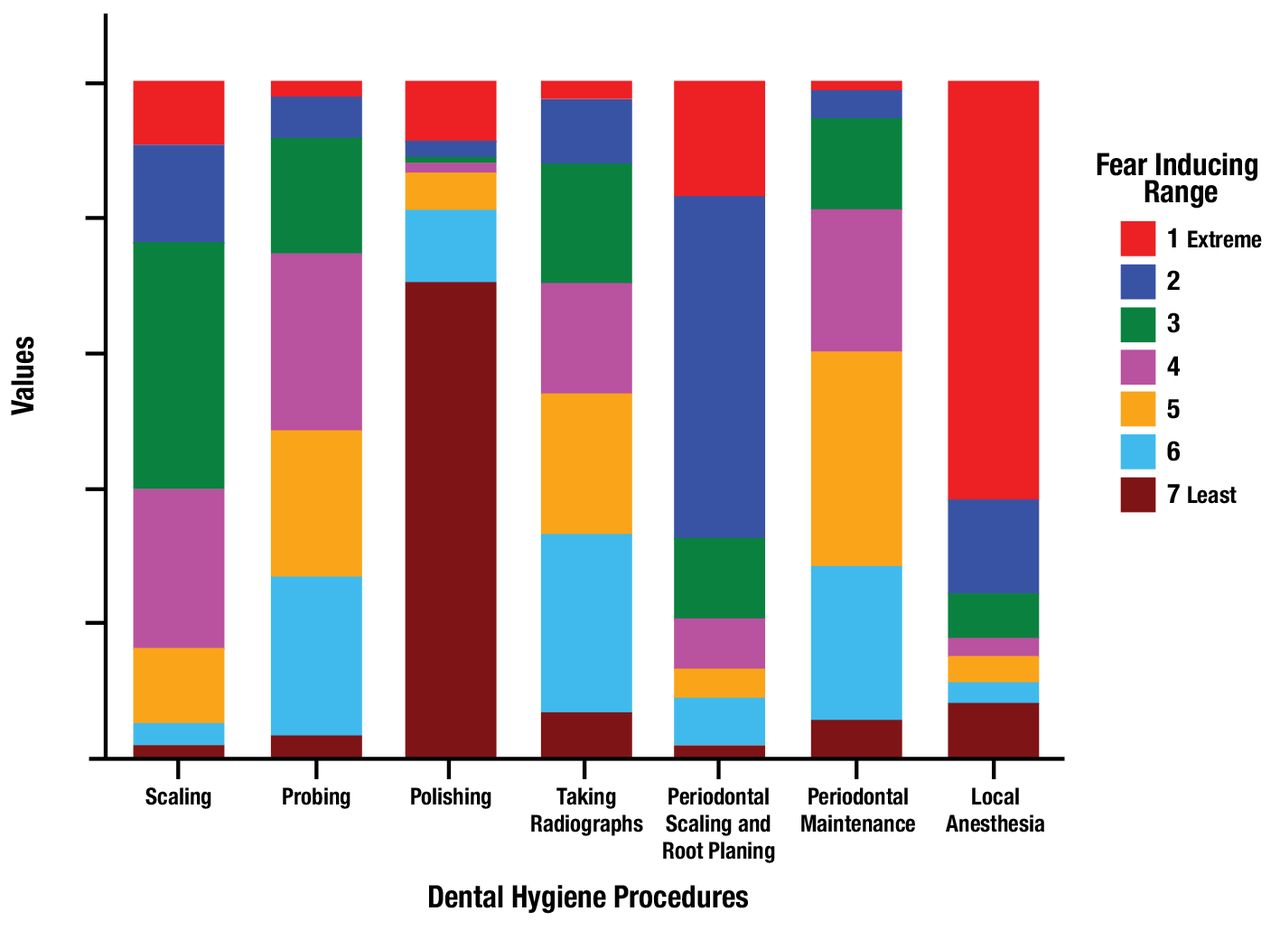
Dental Anxiety Provoking Dental Hygiene Procedures, Ranked by Participants
A chi-square test of independence was performed to examine the relationship between DA preparedness and the need to include DA education in the dental hygiene curriculum. The relationship between these variables was significant (x2(4, 354)=53.615, p<0.001, φ=0.39). Individuals reporting that their education did not adequately prepare them to address DA were more likely to endorse the need for increased DA education; however, 48% of the self-reportedly prepared individuals also believed that there is a demand for more education in DA.
Responses regarding the relationship between attending postgraduate/continuing education courses in the field of DA/care delivery since graduating and referring a patient with an extreme case of DA, dental phobia, for general anesthesia for dental treatment, were tested using a chi-square test of independence and found to be significant (x2(0.203) = 12.874, p=0.002, φ=0.19). Individuals who had not attended postgraduate courses in DA/care delivery since completing their education were more likely to refer DA patients for dental care with general anesthesia; however, 27% of those with additional post-graduate coursework in DA still referred anxious patients for treatment with general anesthesia.
Ordinal regressions were used to test whether age, number of years in practice, confidence level, and provider anxiety would predict the frequency of a dental hygienist directly inquiring about DA, modification of the dental hygiene treatment plan, and allowing for extra treatment time. A test of parallel lines for the three regression models demonstrated the assumption regarding multicollinearity was met (p>0.05).
Practitioner's age, number of years in practice, and personal confidence levels were all significant predictors of whether the dental hygienist would inquire about a patient's DA (p=0.001). For every 1-year increase in age, the likelihood of a dental hygienist reporting inquiring about DA increased by 1.05 times. Regarding practitioners' reported confidence levels, a one-unit increase in confidence predicted that the dental hygienist was 1.46 times more likely to ask directly about DA.
Knowledge of Dental Anviety Management Techniques
Age of the dental hygienist was a significant predictor for modifying the dental hygiene treatment plan/appointment for anxious patients (p=0.009). It was estimated that for every year of the dental hygienist's age in this study, the participant was 1.04 times more likely to report a higher frequency of modification to the treatment plan to accommodate the patient's DA. The remaining predictors were not significant (p>0.05).
Dental hygienists' confidence levels (p=0.006) were significant. It was estimated that an increase in the dental hygienist's confidence resulted in being 1.36 times more likely to have a higher frequency of modifying the treatment plan and allowing extra time for anxious patients. All other predictors were not significant (p>0.05).
Discussion
Dental hygienists are not as effective as licensed psychologists in the management of patients with DA43 due to a lack of expertise,40,44 confidence,40 education 33,45 and training 40,44 in the area of DA. However, this study aimed to survey dental hygienists about their current knowledge, education, confidence, attitudes, and practices surrounding the treatment of adult patients with DA to determine whether practicing clinicians felt the need for more formal education in DA.
While most participants reported knowing that nitrous oxide analgesia and distraction were management techniques for DA, the majority also lacked sufficient knowledge, education or training in using other existing techniques. Similar to findings of Armfield et al.,37 the majority of these participants had not used a validated DA screening tool due to a lack of knowledge regarding these resources. Less than half of the participants felt very confident treating patients with DA. However, provider confidence levels were shown to be significant relative to increased frequencies of treatment modification to accommodate anxious patients. Participants with lower confidence levels were less likely to modify their treatment approach and increased knowledge, education and training was associated with higher confidence levels.
This study also demonstrated a widely recognized need for more formal training in DA in dental hygiene education. Results of this study were consistent with the findings of Armfield et al.,37 who reported inadequate training in the identification and management of patients with DA during dental education.37 Dental hygienists from this study also believed their undergraduate education did not adequately prepare them to address the needs of anxious patients and reported a need for more education focused on DA. Even those participants who reported being prepared in addressing anxiety issues still felt the need for more DA education. The importance of DA training for DH's has also been based on the premise that DHs are typically the first providers in the dental setting to encounter a patient with DA.39,41 Increased confidence levels in caring for DA patients would also benefit the overall dental practice.
Study results also showed that increased confidence towards caring for DA patients, resulted in allowing additional time for dental hygiene care appointments to accommodate for DA. These findings are similar to the results of Brahm et al., with over half of the participants reporting that they allowed extra time when treating patients with DA.33,37 Most dental hygienists in this study reported a preference towards referring patients with DA to receive general anesthesia when needing dental treatment, also similar to the outcomes from Brahm et al.33
Limitations of this study include the non-probability nature of snowball sampling, self-report bias, and recall bias. A virtual snowball sampling technique using social media was utilized for this study to more effectively capture the opinions of DH professionals. While this method is useful in identifying experts and professionals for survey research it limits the ability to generalize the findings. The results may also be biased by individuals with more social media connections or individuals who use social media versus those who do not. Study conclusions may be best conceptualized by taking into consideration that the respondents were individuals who had social media accounts, read their news feeds/notifications, and use read their accounts with some frequency. Traditional phone or mail survey techniques may have also resulted in differences due to the affinity of older generations to use more traditional communication pathways versus the younger generations' use of electronic and social media platforms. However, the age range of this study sample was wide and significant differences based on age are unlikely to significantly change interpretation. Self-reporting bias and recall bias may have influenced participant responses, especially in regards to details on past educational experiences.
Conclusion
Dental anxiety is widespread in the U.S., affecting a large segment of the adult population. Oral health care providers need to be able to identify effective treatment approaches for anxious patients. Study results indicate that practicing dental hygienists are not adequately equipped to effectively treat patients with DA and suggests the need for more formal undergraduate education focused on DA in addition to post-graduate courses. Increased education experiences and the development of skills addressing DA, could increase the dental hygienists' confidence levels and in turn improve oral health care experiences and outcomes for patients suffering from dental anxieties.
Acknowledgments
The authors would like to extend thanks to the leaders of the various dental hygiene social media sites for their assistance with this survey as well as the study participants.
Footnotes
Debra A. Drown, RDH, MSDH is a practicing clinician and an adjunct faculty member at the University of New England, Portland ME.
Lori J. Giblin-Scanlon, RDH, MS is an associate professor and associate dean, clinical programs, Forsyth School of Dental Hygiene, MCPHS University, Boston, MA.
Jared Vineyard, PhD is a postdoctoral fellow, Idaho State University Center for Health Research, Boise, ID.
Dianne Smallidge, RDH, EdD is an associate professor and graduate program director; Christine Dominick, CDA, RDH, MEd is a professor and associate dean; both at the Forsyth School of Dental Hygiene, MCPHS University, Boston, MA.
This manuscript supports the NDHRA priority area, Professional Development: Education (evaluation)
- Received September 21, 2017.
- Accepted February 11, 2018.
- Copyright © 2018 The American Dental Hygienists’ Association





{kind=link}