



Abstract
Purpose: The purpose of this study was to assess dentists' and dental hygienists' current motivation, attitudes, and knowledge regarding volunteering in a non-profit dental setting and the opportunity for earning continuing education (CE) credits.
Methods: This cross-sectional study surveyed a convenience sample of dental and dental hygiene professionals from the state of Michigan. A 20-question paper survey was developed and pilot tested. The survey was disseminated to attendees at various component meetings of the dental and dental hygienists' associations in southeastern Michigan.
Results: Out of the 274 surveys that were distributed, 182 (n=182) were completed, yielding a 66% response rate. Eighty percent of the participants were unaware of the opportunity for earning CE by volunteering and 79% were unaware of the volunteering site approval requirement by the Michigan Board of Dentistry. Thirty percent of participants were unable to determine how many unpaid days per year they were willing to volunteer and a similar percentage, (28%), were unable to determine how many paid days. The most common motivating factor to volunteer was to give back to the community (60%) while the greatest barrier was lack of time (62%).
Conclusion: The opportunity to earn CE credit for volunteerism is seen as a benefit, however, it needs to be better promoted to potential volunteers, through dissemination of information by professional associations and in educational settings. Community-based clinics also need to be made aware of how to become a CE provider. Further research on the longitudinal impact of CE for volunteerism in community-based clinics is warranted.
Introduction
Oral health care is not uniformly attainable by all in the United States (U.S.).1 Individuals lacking access include those living in poverty, people with special needs, older adults, pregnant women, children, and racial minorities. Unfortunately, these underserved populations consistently have the most need for dental care.1 Consequences of these disparities have significant influence not only on oral health, but also on overall health. Poor oral health can lead to poor health outcomes,2 and has been associated with diabetes, cardiovascular disease, and premature/low birthweight births.2 Oral disease in pregnant women and young mothers can be transmitted to their children, perpetuating a cycle of disease.2 Adverse effects of oral disease present an economic burden to the patient and society in lost productivity and missed days from work or school.3
The U.S. Surgeon General issued a call to action in 2003 addressing all levels of public health policy makers and practitioners.4 Several objectives were outlined to improve access to oral health care including a focus on the promotion of programs designed to improve access to care.4 The call to action also addressed exploring policy changes that would result in increased provider participation in public health insurance programs, empowering the public to implement solutions to meet oral health care needs, and evaluating effectiveness of access to care programs.4
Access to Care in Michigan
The 2020 Michigan State Oral Health Plan was developed by the Michigan Oral Health Coalition and the Michigan Department of Health and Human Services with the goal of creating a plan to promote health, prevent disease, and improve access to health care for Michigan residents.5 In the area of improved access to oral care, five objectives were outlined, three of which were specifically related to improving access. These objectives included decreasing the number of underinsured and uninsured people; reducing barriers to oral care; and increasing comprehensive care services among young people, those with disabilities, and pregnant mothers.5 It was envisioned that by attaining these objectives, oral health disparities should decrease in the state of Michigan.5
In 2014, a little more than half (55%) of Michigan residents with a household income of less than $20,000 reported not having had a dental visit that year, compared with only 14% among those with household incomes of $75,000 or more.5 There are several factors, most of which originate from the social and economic environment, impacting the ability of an individual with low socioeconomic status (SES) to access services for oral preventive care and treatment. Shortages of providers practicing in low-income communities, shortages of dentists willing to accept public insurance reimbursement such as Medicaid, high rates of unemployment, jobs that do not offer dental insurance, and limited or no transportation services are just a few of the barriers to oral health care faced by individuals with low SES.5
These circumstances leave very few options for over 1.89 million people in Michigan living at or below 200% of the federal poverty level.6 Persons with low SES in every age group are more likely to have had a history of dental caries and more than twice as likely to have untreated dental caries when compared to those with annual income above 200% of the poverty level.7 These individuals must most often seek oral care from Federally Qualified Health Centers (FQHCs) provided they have dental benefits through Medicaid; those without insurance benefits often need to find a non-profit community-based clinic. Increased competition for funding has presented challenges for community-based clinics to find operating capital; particularly since a large percentage of the costs go to paying dental professionals to treat the patients.8 It has become common for these community-based clinics to rely on volunteer dentists and dental hygienists for patient care; however, it can be difficult to find oral health care providers willing to volunteer their valuable time and skills.8
Continuing Education
Continuing education has been promoted as a means to maintaining clinical competence with a focus on improving patient health outcomes, dating to the 1960's. In recent years, Boards of Dentistry have begun to explore obtaining continuing education credits for providing care in underserved areas as an avenue for increasing the number of providers available to care for vulnerable populations in response to the Surgeon General's call for action to investigate innovative plans to reduce health disparities.10,11 Currently, 49 states and the District of Columbia, have practice act rules requiring CE for licensure renewal for dental hygienists,12 and 19 states allow for clinical volunteering in access to care settings as a means of obtaining CE credits.12
Wilkie et al. studied the knowledge and attitudes of dental hygienists in the Idaho, a state granting CE units for clinical volunteering, as compared to dental hygienists in Utah, a state that does not offer a CE option for volunteering.13 Results showed that nearly half, 43%, of the dental hygienists expressed uncertainty whether time spent volunteering in a clinical setting was an option for earning CE credits toward license renewal in their respective state.13 It was concluded that amendments to Administrative Rules, which are intended to encourage volunteerism in access to care settings, may have little to no bearing on the actual number of volunteer hours performed.13
Motivation to Volunteer
Volunteerism is defined as an altruistic activity where an individual or group provides services for no financial gain.14 Nearly half of the respondents, 44%, in the Wilkie et al. study stated that the CE credits to satisfy state licensing requirements was the greatest motivating factor to volunteerism.13 Wilkie et al. further concluded while the respondents had positive attitudes toward volunteerism, the actual willingness to participate may have been influenced by outside forces, such as encouragement by colleagues or professional organizations.13 Study results also indicated that dental hygienists respond positively to opportunities that simulate intrinsic motivation, allow for self-initiation, and are interesting and challenging; suggesting that simply increasing awareness of oral health needs and ways to meet them, may provide adequate encouragement for volunteering.13
Participants in a survey conducted by Patel et al., reported that dental professionals were motivated to volunteer by intrinsic factors such as giving back to the community, helping others in need, having the opportunity to travel to other countries, and collaborating with other health professionals.15 In contrast, Rovers et al. found that medical and physician's assisting students were motivated to volunteer by extrinsic factors such as a means to build a curriculum vitae, earn academic credit, improve clinical skills, and experience other cultures.16
Service-learning is defined as, “any carefully monitored service experience in which a student has intentional learning goals and reflects actively on what he or she is learning throughout the experience.”17 As part of an educational curriculum, service-learning has shown to improve students' attitudes toward community service by increasing perceptions of connectedness to a community, obligation to help the community, benefits, and intention.18 Coe et al. found that by exposing dental students to existing health disparities in the community, and providing opportunities to provide care to underserved populations, students are more likely to develop a stronger awareness of needs in the community and a willingness to offer their skills once their career begins.18 These results suggest that a positive attitude toward the delivery of care to an underserved population should be a fundamental part of professional training.
Level of education may also be a factor affecting volunteerism. Dental hygienists with a bachelor's, master's, or a doctoral degree have been found to have more positive attitudes toward community service, a greater sense of patient need, and were more likely to volunteer in underserved populations than those with an associate's degree.19 Studies surveying surgeons with doctoral and post-doctoral degrees, found a significant frequency related to past volunteer experiences.20,21
Volunteer Opportunities and Barriers
Oral health care professionals must be able to know where find volunteer opportunities; limited awareness presents significant challenges for not-for profit community clinics. Potential volunteers are also unaware of the tangible benefits such as CE associated with donating their time and skills.13 Lack of awareness of opportunities to volunteer has been cited in multiple studies,13,21,22 while the most frequently cited barriers include time constraints due to family, work, or school.13,15,19-21 Obligations, such as needing to work to pay off student loans and/or cover practice overhead, may outweigh the benefit of giving back to the community.18 Other identified additional concerns include the risk of causing harm to patients, not being able to meet the needs of the patients, language barriers, lack of transportation, and in one case, familial disapproval.15,16,22,23
Michigan Dental Professional Data
Dentists licensed in Michigan must complete 60 hours of continuing education credits within a three-year licensing period.9 Up to twenty of the required continuing education credits may be obtained by volunteering in a community-based clinic approved by the Michigan Board of Dentistry at the rate of one credit hour awarded for 120 minutes of patient care.9 Dental hygienists licensed in Michigan are required to complete 36 continuing education credits within a three-year licensing period. Up to 12 credits may be awarded as clinical volunteerism from a program or clinic approved by the Michigan Board of Dentistry.9 Data from September 2016, indicates 5,839 actively licensed dentists in Michigan,24 and 9,870 registered dental hygienists as of May 2015.25 Obtaining continuing education credits through seminars, programs, and lectures are most often paid for by the professional. However clinical volunteerism may be a more cost-effective method to supplementing one's continuing education requirements while also addressing access to care issues. Given the total number of oral health care professionals in Michigan, utilizing these volunteer services could be a part of a comprehensive approach to making a significant impact on oral health care access in the state.
The Michigan Board of Dentistry amended the Administrative Rules, providing dentists and dental hygienists the option to provide care on a volunteer basis in approved community-based facilities in exchange for continuing education (CE) credits in December of 2015.9 Given the recent adoption of this rule, many oral health care professionals may be unaware of this opportunity. The purpose of this study was to assess dentists' and dental hygienists' current motivation, attitudes, and knowledge regarding volunteering in a non-profit dental setting and the opportunity for earning continuing education credits.
Methods
This cross-sectional study surveyed a convenience sample of dental and dental hygiene professionals from southeastern Michigan and was granted Institutional Review Board (IRB) exemption status by the University of Michigan Health Sciences and Behavioral Sciences IRB.
The paper survey consisted of 20 multiple choice, close-ended, partially close-ended, and Likert Scale questions focusing on personal and career characteristics, knowledge of current state regulations, previous volunteering experience, and attitudes regarding volunteerism. Content validity was determined through pilot tested of the survey by three registered dental hygienists and one licensed dentist. Survey modifications were made based on their feedback.
The final paper-based survey was distributed at Michigan Dental Association (MDA) and Michigan Dental Hygienists' Association (MDHA) component meetings held during the months of September-October 2016. Component societies included: Washtenaw District Dental Society, Livingston District Dental Society, Capital District Dental Hygienists' Society, Greater Detroit District Dental Hygienists' Society, and South-Central District Dental Hygienists' Society. The survey included an introduction describing the purpose and intended significance of the project, along with informed consent.
Data analysis was performed with the Statistical Package for the Social Sciences (IBM SPSSÒ, Armonk, NY), version 24. Descriptive statistics, specifically the number and percentage of respondents, for each survey item were obtained. Paired samples t-test was used to evaluate the difference between paid days versus unpaid days dentists and dental hygienists were willing to volunteer, as well as the overall difference between paid days and unpaid days. Independent samples t-test was used to determine the difference between American Dental Hygienists' Association (ADHA) and American Dental Association (ADA) member and non-member participants willing to take off paid days versus unpaid days to volunteer. Statistical significance was set at p<0.05.
Results
Out of the 274 surveys that were distributed, 182 (n=182) were completed, yielding a 66% response rate. Of those who participated, 57% were dentists, 38% were dental hygienists, and 5% were dental specialists. The majority of the participants, 76% (n=138), were male and 88% (n=159) identified themselves as White. Thirty-two percent of respondents (n=58) were in practice over 30 years and 18% (n=32) had been practicing 0-5 years. Over half, 55% (n=99), were between the ages of 46-65 years. Forty-two percent (n=76) were members of the ADA and 30% (n=54) were members of the ADHA. Complete demographic information is provided in Table I.
When asked about current knowledge of the 2015 amendment to the Michigan Board of Dentistry Administrative Rules allowing for dental professionals to earn continuing education credits in exchange for volunteered clinical hours for underserved patient care, over three quarters of the respondents were unaware of the amendment or that the clinical setting for earning these CE required approval by the Michigan Board of Dentistry. Over two-thirds of the respondents saw a benefit to volunteering at a not-for-profit community-based clinic, while slightly less than one quarter of the respondents were either unsure or did not see it as a benefit. Additionally, respondents were asked to share how important volunteerism was to them. Nearly half viewed volunteerism as important, a little more than one quarter expressed neutrality, while the remaining quarter of the respondents did not view volunteerism as important.
Participant Demographics
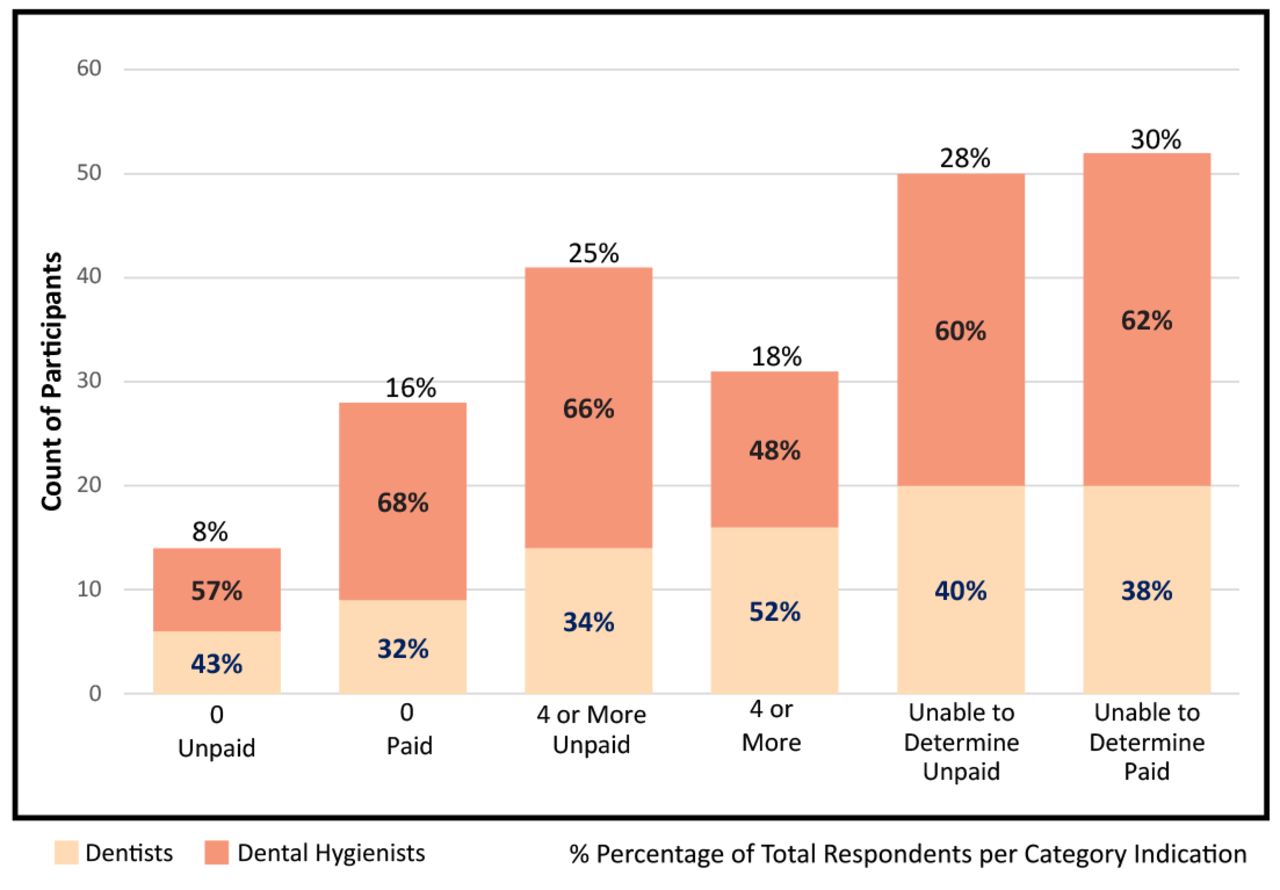
Regarding time commitments, participants were asked how many unpaid and paid days per year they would be willing to volunteer and about two categories of time commitments (Figure 1). “Unpaid days” were defined as regularly scheduled days off and “paid days” were defined as scheduled work days that would be taken off by the clinician in order to volunteer. The most frequent answer for both questions was “unable to determine,” 28% and 30% respectively, followed by “4 or more days per year,” 25% and 18% respectively. Nearly twice as many dental hygienists than dentists were willing to volunteer four or more unpaid days per year. Similarly, more than twice as many dental hygienists as compared to dentists expressed an unwillingness to volunteer any paid days.
Participants were asked to share the most significant factor motivating them to volunteer (Figure 2). Over half indicated “giving back to the community,” followed by “volunteerism is a professional responsibility,” “religious or spiritual reasons,” and “other” which included answers such as an opportunity to teach or learn. Several respondents were motivated by “the opportunity to work with other professionals.”

Number of Days Willing to Volunteer Per Year (n=180)
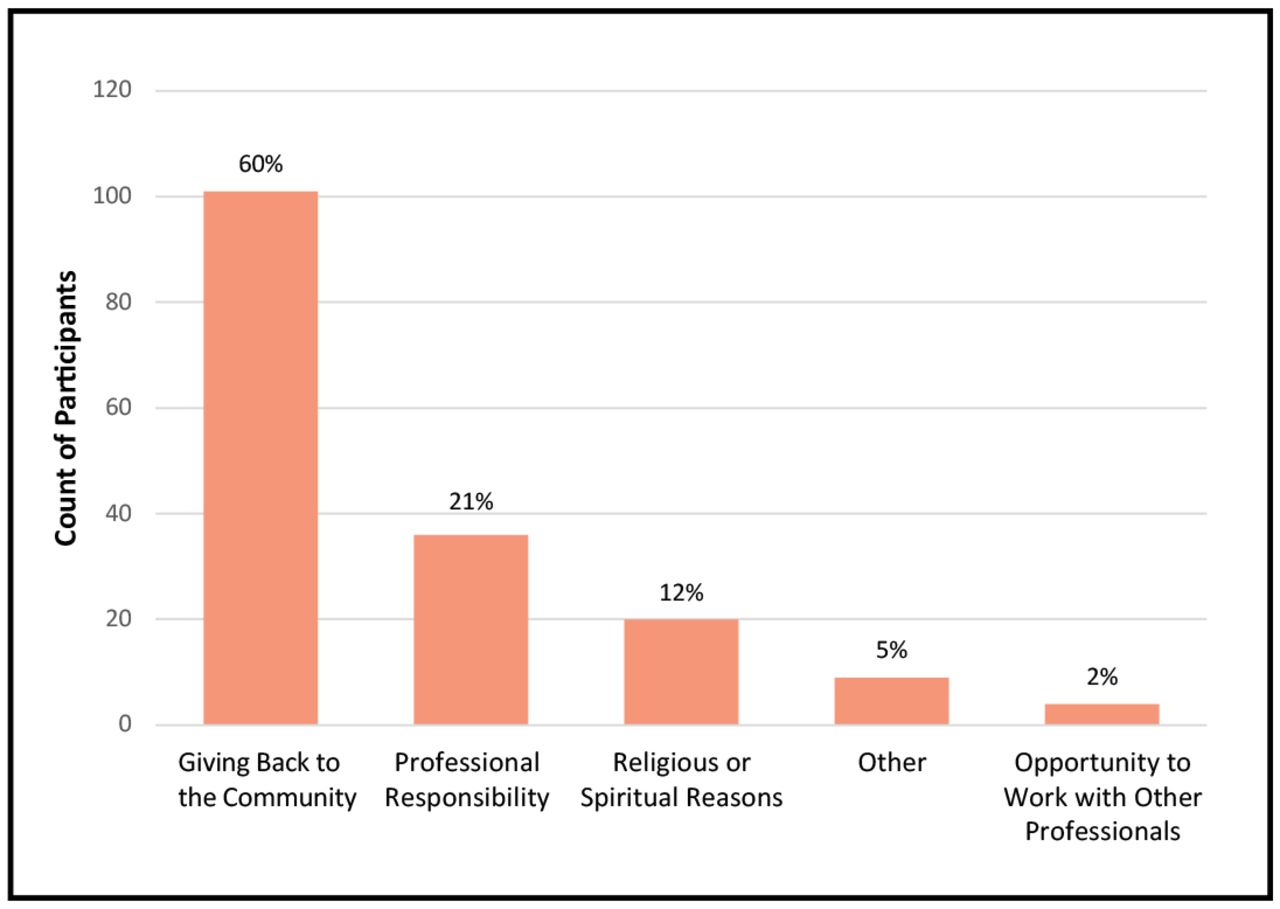
Greatest Motivating Factor to Volunteer (n=170)

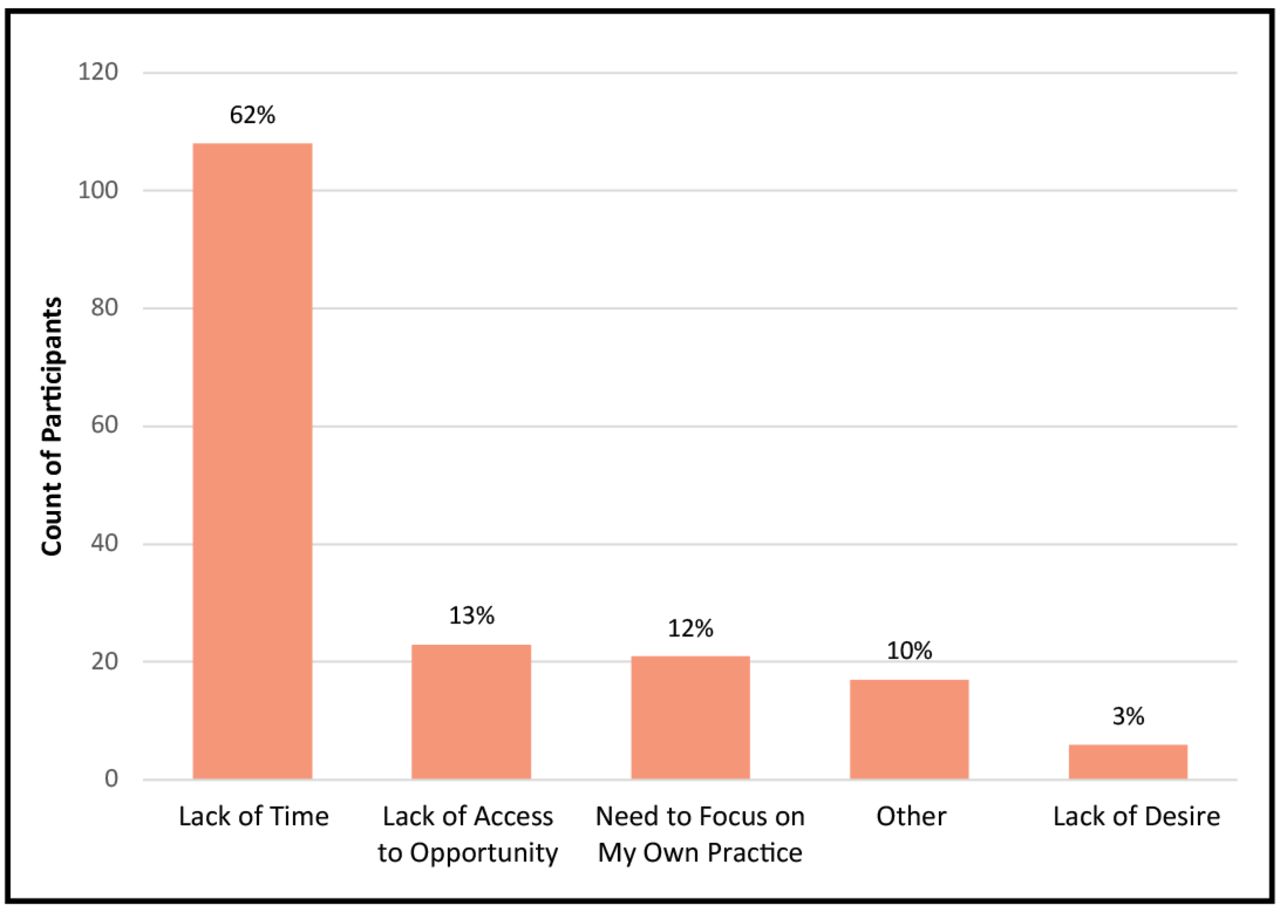
Greatest Barrier to Volunteering (n=175)
Regarding the most significant barriers to volunteering, over half indicated “lack of time” followed by a “lack of access to opportunity to volunteer,” “need to focus on my own practice,” and “other” which included answers such as “chronic injury, health problems, family obligations, and current volunteerism as part of the practice.” Several respondents expressed a “lack of desire to volunteer entirely” (Figure 3).
Differences between demographic variable responses regarding type of days off respondents would be willing to volunteer are shown in Table II. Findings were statistically significant (p =0.002) that, in general, dentist and dental hygienist respondents were willing to volunteer more unpaid days than paid days, per year. There was no statistical significance in dental hygienists' willingness to volunteer unpaid days versus paid days; however, dentists were willing to volunteer more unpaid days than paid days per year (p=0.004). Among ADA/ADHA members and non-members respectively, differences in willingness to volunteer between the number of unpaid days versus paid days was not statistically significant. When comparing ADA/ADHA members verses non-members willingness to volunteer paid days, it was found that professional association members were, on average, willing to sacrifice more paid days (p=0.005) No statistical significance was found when comparing member versus non-member unpaid days.
Discussion
The majority of the respondents were unaware of the opportunities for earning CE by volunteering their services at not-for-profit community-based clinics nor were they aware of the site approval requirement by the Michigan Board of Dentistry. These results were similar to those of Wilkie et al. who found that nearly half of the dental hygienists surveyed were unaware of the opportunity to earn CE by volunteering in the state of Idaho.13 Similarly, McGlinigle et al. found that over a quarter of the members of the American College of Surgeons were not aware of the “Giving Back Program,” an altruistic outreach program founded by their own professional association.21 These findings suggest an overall lack of knowledge among health care professionals about opportunities available for clinical volunteerism, including those that offer CE. It is recommended that professional associations consider improving communication about any changes in practice act/administrative rule information, as well as clinical volunteer opportunities, to their members. Furthermore, it is recommended that professional schools and dental educational programs, focus on the importance of having an ongoing working knowledge of the state's practice act. It would also be appropriate to emphasize how service-learning activities align with the concept of volunteerism for CE.
Demographic Variables and Types of Days Willing to Volunteer
Results in this study indicated that the greatest motivating factor to volunteerism was giving back to the community, which are similar to the findings of Patel et al.15 The greatest barrier to volunteering among the participants was lack of time, which was consistent with results from five other studies.13,19-22 While study participants indicated a generalized positive attitude and intention to volunteer, a perceived lack of time may still inhibit an oral health care professional from committing to work as a volunteer. Although service-learning is a part of most dental and dental hygiene curricula, opportunities to enhance student involvement should be investigated. As students develop into professionals they should be provided opportunities to increase their understanding of their responsibility as health care providers to help the community.18 Additional emphasis on community outreach should be a special focus in associate degree dental hygiene programs in order for students to achieve attitudes toward volunteerism similar to cohorts who have earned a bachelor's degree or higher.19
Almost a third of participants were “unable to determine” how many paid or unpaid days they would be willing to volunteer. Close to one quarter were willing to devote four or more paid or unpaid days per year to volunteer; and there were twice as many dental hygienists as dentists willing to do so. Additionally, more dentists were willing to volunteer unpaid days, but were significantly less likely to take off paid days for volunteering. These findings combined with the observation that the majority of participants recognized the benefits of receiving CE for volunteering and the perception that volunteerism is an important activity, well positions oral health care professionals for providing care in not-for-profit community clinics, once awareness is raised.
The majority of participants in this study were members of ADA and ADHA and were found to be more likely to volunteer paid days than non-members; however, there was no statistically significant difference in willingness to volunteer on non-paid days related to professional membership. A study by Marsh identified that members of professional associations are more likely to be involved with community service than non-members.19 Based on these findings, professional associations can play a critical role in communicating volunteer opportunities and benefits to their members. Since the new Administrative Rule has gone into effect in Michigan, 12 sites have been approved as volunteer CE sponsors.26 With approximately 107 not-for-profit community dental centers in Michigan,27,28 this accounts for utilization of only 11% of the available clinics, speaking to the need for the development of a means to disseminate this Administrative Rule change along with the steps to become a CE provider. Professional associations could play a role in encouraging these community-based clinics to become CE providers via application to the Michigan Board of Dentistry.
Granting CE through volunteering to provide dental care for vulnerable and underserved populations, was established to assist in addressing the access to care crisis. Although this is one means for doing so, it is only a small contribution toward resolving the access to care crisis. Given the barriers identified in this study, this method of increasing the volunteer work force may not provide a long-term solution for a shortage of volunteers in community-based dental clinics. Several limitations of this study should be noted. This study had a small sample size from Southeast Michigan only. Nearly three quarters of participants were members of a professional association, and consideration should be given to disseminating this survey to a cross-section of professionals that better represents all licentiates. In addition, further research should focus on the specific opportunities available for clinical volunteer involvement and the long-term effects.
Conclusions
Access to oral health care for uninsured/underserved populations is an ongoing problem in the U.S. Community-based dental clinics rely heavily on volunteers for patient care. Reliance on volunteers is challenging to sustain as it cannot be guaranteed that professionals will be available or willing to provide care. While the incentive of earning CE in exchange for volunteerism will not solve the access to care crisis, it may serve as a useful means of providing care for underserved populations. Opportunities to earn CE credit for volunteerism is seen as a benefit; however, foundations for this concept should be addressed in professional educational programs. In addition, knowledge of changes to state practice acts and volunteer opportunities should be promoted by professional associations and other organizations. Community-based clinics also need to be made aware of the process for becoming a CE provider. Further research on the longitudinal impact of CE for volunteering care in not-for-profit community-based clinics is warranted.
Acknowledgements
The authors wish to thank L. Susan Taichman, RDH, MPH, PhD; Wendy Kerschbaum, RDH, MA, MPH, and Joseph Naiman for their support throughout this study.
Footnotes
Chelsea M. Holladay, RDH, BSDH is a 2017 graduate of the Dental Hygiene Degree Completion Program; Anne E. Gwozdek, RDH, MA is a retired clinical assistant professor in the Department of Periodontics and Oral Medicine; both at the University of Michigan School of Dentistry, Ann Arbor, MI.
This manuscript supports the NDHRA priority area: Professional development: Education (Educational models)
- Received June 22, 2017.
- Accepted March 15, 2018.
- Copyright © 2018 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}