



Abstract
Purpose Immunization rates can be influenced by community access to immunizations and vaccine promotion from eligible providers. The purpose of this study was to assess the perceptions, willingness, and challenges of vaccine administration among Indiana dental hygienists.
Methods This cross-sectional study targeted Indiana-licensed dental hygienists. The survey instrument consisted of six multiple-choice demographic questions; 13 items used a 5-point Likert-type rating scale to measure perceptions about vaccines and willingness to administer vaccines; one rank-in-order question of seven challenges associated with administering vaccines; and two open-ended questions for additional information and comments. Purposive sampling was used, and the electronic survey was promoted through emails, social media, and direct messages. Categorical variables were analyzed and reported using percentages and frequencies. Open-ended answers were examined and reported in the results.
Results Seventy-one Indiana-licensed dental hygienists responded to the survey and were included in the analysis. Most had positive perceptions on vaccines and administering vaccines; 62.3% of the respondents agreed that offering vaccinations in the dental office would improve access to immunizations for patients; 76.8% were willing to receive training to administer vaccines and 66.7% were willing to consider administering vaccines if permitted by the Indiana State Practice Act. While most respondents (77.9%) perceived licensed dental hygienists as competent to administer vaccines, fewer felt comfortable administering vaccines to children (57.8%) as compared adults (63.1%). Education and training were identified as the greatest challenges associated with administering vaccines.
Conclusion Dental hygienists in this study indicated a willingness to fill the role of non-traditional vaccinators. Increasing the number of eligible healthcare workers, who can administer vaccines in Indiana would increase vaccine access and improve state immunization rates. Policymakers should consider amending the dental hygiene practice act to include vaccine administration as part of the permitted duties for dental hygienists in Indiana.
INTRODUCTION
Vaccines prevent 4 million deaths annually,1 contribute to population growth, and are necessary for improving public health resilience in the 21st century.2 Nationally, immunization rates can be affected by community access to immunizations and vaccine promotion from eligible providers.3-5 Furthermore, underserved communities often deal with health disparities due to limited access to health care which contributes to low vaccines rates.3,4 National estimates from the Centers for Disease Control and Prevention (CDC) suggest that 48% of adults 18 and older and 45.9% of children ages 6 months to 17 years received an influenza vaccine in 2023.6 The CDC also reported that 38.6% of children ages 9-17 years received one or more doses of the human papilloma virus (HPV) vaccine in 2022.7 Furthermore, as of May 2024, the CDC estimates about 22.5% of adults 18 years and older received the updated 2023-2024 COVID-19 vaccines.8 A common public health goal (e.g., Healthy People 2030) is to increase immunization rates by improving community access to vaccine providers and the location of vaccine services.9 With a national shortage in the health care workforce,10 professional associations and state policymakers have considered legislation to improve access to vaccines by permitting non-traditional immunizers, like dental professionals, to administer vaccines.3-5,11
Dental professionals (dentists and dental hygienists) have been recognized during the H1N1 and COVID-19 public health emergencies for their utility with administering vaccines through emergency authorization, thus increasing the number of vaccinators.11,12 During the COVID-19 pandemic, 20 states temporarily expanded their dental hygiene practice acts and 40 states expanded their dental practice acts to include administering the COVID-19 vaccine.12,13 Recently, Oregon, Illinois, and Minnesota passed legislation permitting dentists to administer vaccines in the dental office (e.g., influenza, HPV, and COVID-19).11,14 In 2021, Indiana approved dentists to administer vaccines to individuals aged 11 and up.14 However, at the time of this study there was no published data to determine the safety and effect of dentists or dental hygienists administering vaccines. In Japan, supportive research by Kagawa et al. revealed no significant differences in the safety or side effects in patients who received the COVID-19 vaccination by Japanese nurses and dentists.15
Dental professionals have been recognized for their role in infectious disease prevention,16 like HPV that can lead to high rates of oral and oropharyngeal cancers (OOPCs).17,18 Not only is HPV a vaccine-preventable disease, but the Food and Drug Administration approved the Gardasil 9 HPV vaccine for the prevention of OOPCs.19 The American Dental Association and the American Academy of Pediatric Dentistry support and encourage oral health providers to educate, promote, and advocate for HPV prevention in the dental office and their local communities.17,18 Dental professionals who perform oral cancer screenings on their patients have an opportunity to discuss HPV-related OOPCs and prevention through vaccination.20
Pharmacists, as non-traditional vaccinators, have successfully improved community influenza immunization rates for some underserved populations.5 Part of this success is attributed to the population who access the pharmacy to get their prescriptions (e.g., older adults), and the location of the pharmacy as many are in low-income neighborhoods.3 Likewise, some populations (e.g., adolescents) may seek routine care more frequently from their dental care provider as compared to their physician.16 Dental professionals are also employed in various public health settings like hospitals, jails, schools, WIC clinics, FQHCs, and health departments, creating greater access to care for underserved communities.21 Therefore, expanding the role of dental professionals to administer vaccines can encourage a medical-dental collaboration to meet the vaccine needs of thousands who visit the dental office.16,22
Due to advancements in the profession, dental hygienists have expanded their scope of practice and skills to meet the needs of their patients.23,24 Most state practice acts permit dental hygienists to administer local anesthetic, provide a range of oral disease treatments and services, and promote disease prevention for overall health (e.g., glucose screenings, tobacco cessation education, blood pressure screenings, oral cancer screenings, medical history updates, etc.).11,24,25 Thompson et al. found that a small sample of dental hygienists from across the United States were willing to be trained in vaccine promotion.26 Additionally, a survey by Guadiana et al. found that Michigan dental hygienists were willing to be trained to administer the HPV vaccine.17 Furthermore, Askelson et al. observed that Iowa dental hygienists were trusted by their patients and a reliable source for receiving oral health related recommendations.27 Therefore, access to preventive care may be improved and patient satisfaction increased by expanding the dental hygiene scope of practice23,24,28 and permitting additional services like administering vaccines.12,17
There is limited peer-reviewed, evidenced-based research in the literature regarding dental professionals’, specifically dental hygienists’, willingness to administer vaccines in the dental office. More notably, several studies have shown that dental professionals from various states and regions have an overall positive attitude toward vaccines and a willingness to train to administer vaccines.11,17,20 Most of the existing literature regarding dental professionals and vaccines is focused on their knowledge, attitudes, and beliefs or behaviors regarding HPV-related OOPC and the HPV vaccines.17,22,26,29-35 The literature reviewed found inconsistent knowledge levels, attitudes, and behaviors regarding HPV-OOPC and HPV vaccines among dental professionals and oral health care students.36,37 Additionally, some studies identified dental professionals’ perceived challenges with discussing and promoting vaccines in the dental office.11,12,17,22,26,35,38,39 The challenges included comfort and confidence with discussing vaccine-related topics with their patients (e.g., age of patient and sensitivity with infectious disease-related discussions), limited knowledge on vaccines, personal beliefs, liability, professional role conflicts, and lack of training.11,12,17,22,26,35,38,39 To address some of these challenges, a few studies suggested that vaccine education and training programs can improve dental professionals’ knowledge, skill, and comfort or confidence with discussing vaccines and vaccine-preventable diseases.26,35,40 While dental professionals may expand their roles as non-traditional immunizers to improve community access to vaccines, understanding their willingness and perceived challenges to administering vaccines can support policy development and encourage state practice acts to include dental professionals in administering vaccines. Understanding the challenges of administering vaccines can also lead to the development and implementation of vaccine-focused educational topics and training though dental professional continuing education courses and in program curriculum.
Shukla et al. assessed the willingness of Indiana dentists to administer vaccines (HPV, influenza, COVID-19, and Hepatitis A) in the dental office to adults and children.11 Results from the study suggested a willingness of Indiana dentists to administer vaccines if permitted by the state practice act, however Indiana dental hygienists were not included in the study.11 Furthermore, when legislation was approved for Indiana dentists to administer vaccines, Indiana dental hygienists were excluded. Therefore, the purpose of this study was to assess the perceptions, willingness, and challenges of vaccine administration among Indiana dental hygienists. The data can support legislation from Indiana policymakers and other professional organizations regarding dental hygienists administering vaccines. Additionally, understanding the perceived challenges may lead to appropriate solutions for dental providers who are administering vaccines.
METHODS
A.T. Still University Institutional Review Board determined this study exempt (#2023-099). A cross-sectional, quantitative survey adapted from Shukla et al.11 was used to collect information on Indiana-licensed dental hygienists’ professional demographics, perceptions of vaccines, willingness to administer vaccines, and perceived challenges with administering vaccines. A panel of five professionals with medical, health sciences, and research credentials used a 3-point scoring rubric to review the survey and provided feedback. Modifications included rewording content and adding questions to be specific to dental hygienists, survey format, and grammatical edits. The authors reviewed the panels’ completed rubrics and updated the survey. The panel participated in a beta test of the survey and gave their final approval.
The survey consisted of six multiple-choice questions regarding the participants’ demographics; 13 items used a 5-point Likert-type rating scale to measure the participants’ perceptions about vaccines and willingness to administer vaccines; a rank-in-order question of seven challenges associated with administering vaccines; and two pull-down options for respondents to provide additional information and general comments. A statement of informed consent was provided; completion of the survey confirmed subject consent. Participation in the survey was voluntary; participants were able to exit the survey at any time. The survey was administered through an electronic platform (Qualtrics; Seattle, WA), available for six weeks, and could be accessed using a weblink or QR code.
The target population was 5,169 Indiana-licensed dental hygienists.41 Nonprobability, purposive sampling was used to access the study population. The Indiana Dental Hygienists’ Association (IDHA) approved using their member email list and social media outlets to promote the survey. Additionally, direct messages were used to promote participation. The IDHA had approximately 220 members in its email bank and 1,200 followers on social media. The participants included Indiana-licensed dental hygienists; over the age of 18, who “have graduated from an accredited dental hygiene program, have completed and passed a National Board Exam and a state or regional clinical licensure exam”42 and have an Indiana dental hygiene license.
Deidentified survey data was collected, downloaded, and transferred into a statistical software program (SPSS version 29.0; IBM, Armonk, NY) for quantitative analysis. The multiple-choice questions were individually totaled, and the findings were reported using frequencies and percentages. The Likert-scale ranged from Strongly Agree, Agree, Strongly Disagree, Disagree, and Unsure; each value was totaled, and the findings were reported using frequencies and percentages. The seven challenges of administering vaccines were listed (insufficient training/knowledge, comfort levels, role confusion, reimbursement, time, storage of vaccines/supply chain, and other with a corresponding box to type in other challenges), and participants were asked to arrange the challenges in order of most challenging to least challenging. Each challenge was reported as the percentage of participants that ranked that challenge as the most challenging, second challenging, third challenging, etc. The vaccine willingness questions were individually totaled, and the findings were reported as frequencies and percentages. The open-ended comments were examined and reported in the results.
RESULTS
Seventy-seven survey attempts were recorded; six respondents were excluded from the final sample as they did not meet the inclusion criteria of having an Indiana dental hygiene license. The sample demographics are shown in Table I; data was missing from participants who chose not to answer the items. Notably, half of the participants practiced dental hygiene for 21 years or longer (50.7%).
Sample demographics* (n=71)
Perceptions on Vaccines
Table II provides data from the survey that addressed Indiana dental hygienists’ perceptions of vaccines and willingness to administer vaccines; data was missing from participants who chose not to answer the items. All references to the Likert-scale Strongly Agree and Agree were combined and reported as “agreed.” Overall, the respondents showed positive perceptions on vaccines. The majority (82.6%) agreed that there is scientific proof that immunization helps to prevent infectious diseases. Regarding HPV-related oropharyngeal cancers, most participants (73.1%) perceived that this type of cancer can be prevented using vaccines. The respondents agreed (62.3%) that offering vaccinations in the dental office would improve access to immunizations for patients. Most (77.9%) agreed that licensed dental hygienists are competent to administer vaccines.
Respondents’ perceptions and beliefs on vaccines* (n= 71)
Willingness to Administer Vaccines
Of the surveyed dental hygienists, 57.8% agreed that they are comfortable administering vaccines to children ages 11 to 18. In comparison, a greater percentage (63.1%) noted they are comfortable administering vaccines to adults. The majority (88.0%) agreed that they are willing to be educated about vaccine-preventable diseases. Most (76.8%) were willing to receive training to administer vaccines. The participants had positive perceptions on administering different types of vaccines to children ages 11 and up: HPV (55.4%), influenza (69.2%), COVID-19 (63.4%), and other vaccines (50.8%).The respondents also had positive perceptions of administering different types of vaccines to adults: HPV (61.3%), influenza (67.7%), COVID-19 (63.1%), and other vaccines (53.1%). Overall, the participants were willing or very willing (66.7%) to consider administering vaccines if permitted by Indiana legislation.
Perceived Challenges to Administering Vaccines
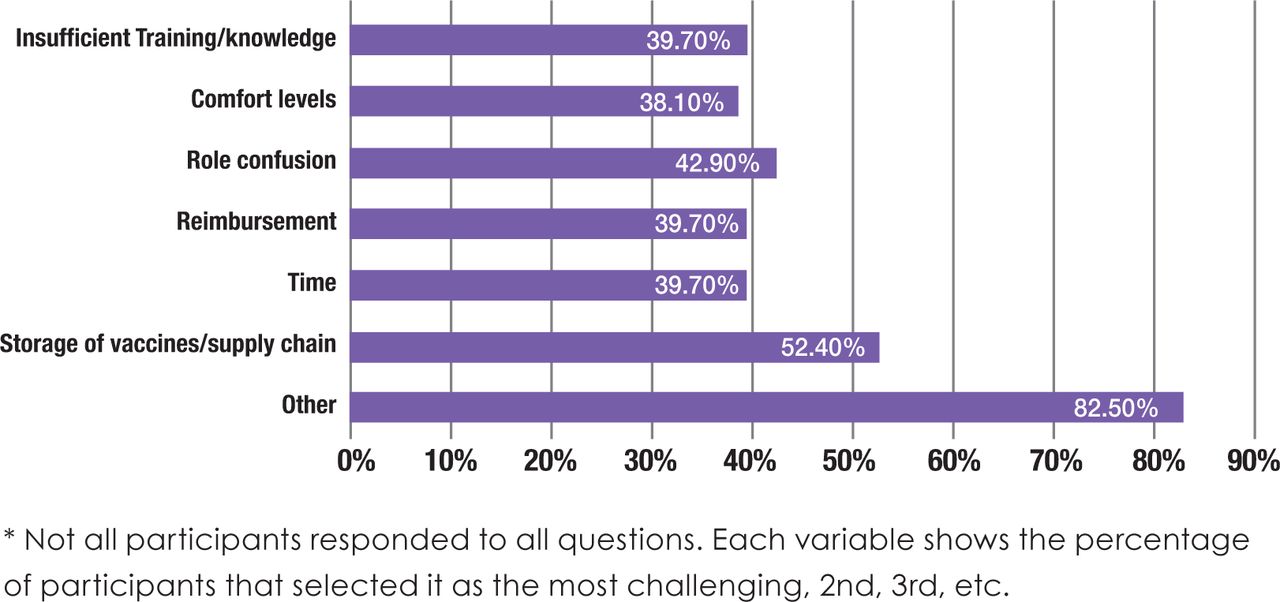
The ranked challenges that the respondents may face with administering vaccines are shown in Figure 1. Overall, “insufficient training and knowledge” was selected as the most challenging and “other” challenges was selected as the least challenging. The open-ended responses included “other” challenges such as patient fear of the dental office; ethical duty and not knowing the long-term effects of the vaccines (especially in children); parental consent; legislation; employer’s willingness; conflict of religious beliefs; no interest; malpractice lawsuit; location; certification; and risks.

Respondents’ perceived challenges to administering vaccines, ranked from most to least challenging* (n = 71)
DISCUSSION
This study assessed the perceptions, willingness, and challenges of vaccine administration among Indiana dental hygienists. Overall, the participants had positive perceptions of vaccines. Most of the surveyed dental hygienists were either willing or very willing to consider administering vaccines if permitted by Indiana legislation.
This study adapted the survey from Shukla et al. who assessed Indiana dentists’ willingness to administer vaccines.11 In comparison, this study had a smaller sample of dental hygienists as compared to the sample of dentists. Shukla et al. reported data for each variable and performed a multivariable analysis to compare dentists’ willingness to administer vaccines by professional characteristics.11 Results from the multivariable analysis found that dentists who practiced in public health clinics were more willing to consider administering vaccines.11 Additionally, Shukla et al. reported that as the dentists’ years in practice increased, there was a decrease in agreement that dentists should be allowed to administer HPV, influenza, Hepatitis A, and COVID-19 vaccines to children and adults.11
In this study, most of the participants had practiced dental hygiene for 21 years or longer, and they were willing to administer HPV, influenza, and COVID-19 vaccines. Consistent with this study’s findings, Shukla et al. identified overall positive perceptions and willingness of Indiana dentists to administer vaccines.11 Likewise, Shukla et al. found that Indiana dentists perceived a greater level of comfort with administering vaccines to adults compared to children.11 Conversely, most Indiana dentists identified storage of vaccines and supply chain issues as the most challenging.11 This study found that the surveyed dental hygienists perceived insufficient training and knowledge as the greatest challenge. Similar challenges associated with dental professionals discussing vaccine-preventable diseases and promoting vaccines in the dental office have been reported in the literature.11,17,36,37 Barriers to administering vaccines and vaccine promotion in the dental office can be addressed through guidance and collaboration with public health authorities.12,31 Additionally, policy changes at the state level permitting dental professionals to administer vaccines can encourage professional education courses and program curriculum updates for oral health students, improving knowledge and training on vaccines.11,22,17 Previous research has focused on administration of HPV vaccines in the dental office.17,22,26,29-35 This study found that over half of the participants agreed (73.1%) that HPV-related OOPCs can be prevented using vaccines. Similarly, other studies found that dental professionals had positive attitudes toward HPV-related OOPC prevention by using vaccines.17,29,33 To increase vaccine awareness and skills, studies that implemented HPV prevention education and training courses for dental hygiene students reported an increase in their knowledge, attitudes, comfort, and confidence in discussing HPV-related topics with their patients.40,43
Over half (66.2%) of the participants in this study had not previously participated in an educational course on vaccine-preventable diseases, however most (75.4%) noted having a policy regarding oral cancer screening in their office. These findings are contradictory as oral cancer screening is a conduit to disease prevention education. It is possible that the participants misinterpreted the survey question since “educational course” was not formally defined. Professional continuing educational courses are designed to offer information and improve dental professionals’ education and skills. Additionally, accredited dental hygiene programs must have biomedical sciences, health promotion, and disease prevention standards in the curriculum.44 However, specific information on current vaccine schedules, vaccine storage, vaccine preparation, and vaccine dose may not be provided in the curriculum. Therefore, the findings from the study suggest a need to increase Indiana dental hygienists’ vaccine knowledge, which can be achieved through continuing education courses and implemented in program curriculum.
Dental visits provide the opportunity for patients to receive vaccine promotion and education from a trusted dental professional.20 While there are over 5,000 Indiana-licensed dental hygienists,41 using dental hygienists as non-traditional immunizers, could improve access to vaccine promotion in Indiana. At the end of the 2022-2023 influenza season, the CDC estimated that fewer than half (45.6%) of Indiana residents aged 6 months and up received the influenza vaccine.45 Additionally, the 2021 National Immunization Survey–Teen found that 55.2% of Indiana adolescents aged 9-14 years completed a full series of the HPV vaccine, falling behind the national average of 61.7%.46 Furthermore, as of May 2024, the CDC estimated that only 20.2% of Indiana adults aged 18 and older received the updated 2023-2024 COVID-19 vaccines.8 The participants in this study had positive perceptions on vaccinating adults and children with the HPV, influenza, COVID-19, and other vaccines. While there is opportunity to improve Indiana’s immunizations rates for children and adults,47 permitting dental hygienists to administer vaccines could increase the number of vaccinators available to dental patients.
Limitations and Strengths
Several limitations in this study may have contributed to a response bias. The survey was provided on an electronic platform, and it could only be accessed using the internet (e.g., smartphone or computer/tablet). Additionally, the survey was promoted using the electronic methods of social media, email, and direct messages. Response accuracy may have been affected due to the participant’s interpretation of the survey questions. Another limitation of this study is that it only assessed Indiana-licensed dental hygienists and did not include dental hygienists outside of the state. Therefore, the small sample limited the generalization of the results and may not adequately reflect the larger populations’ perceptions of vaccines or willingness to administer vaccines.
At the time of this study, no state practice act has increased the scope of practice for dental hygienists to administer vaccines outside of a public health emergency. This study provided evidence-based data for future research to expand on in permitting dental hygienists to administer vaccines. While the sample of Indiana dental hygienists reflected an overall willingness to administer vaccines if permitted by the state practice act, further research should assess the patient’s perceptions of and willingness to receive vaccines from dental hygienists.
CONCLUSION
Dental hygienists in this study indicated a willingness to fill the role of non-traditional vaccinators. Findings from this study can encourage Indiana policymakers to promote legislation permitting dental hygienists to administer vaccines in the state. Additionally, these findings can contribute to solutions for the common challenges identified by dental professionals on administering vaccines. Considering the opportunity for dental hygienists to be non-traditional vaccinators is appropriate as they are highly educated and trained oral health care specialists and are employed in various settings accessible to underserved populations. Expanding the number of eligible Indiana vaccine providers by including dental hygienists may increase access to vaccines for many that visit the dental office; and improve immunization rates in the state.
DISCLOSURES
The authors have no conflicts of interest to disclose.
ACKNOWLEMENTS
The authors would like to acknowledge and thank the Indiana Dental Hygienists’ Association Board of Directors who granted permission to use their member email list and social media platform for promoting and distributing the survey to Indiana dental hygienists.
Footnotes
NDHRA priority area, Professional development: Regulation (scope of practice).
- Received May 8, 2024.
- Accepted October 2, 2024.
- Copyright © 2024 The American Dental Hygienists’ Association
This article is open access and may not be copied, distributed or modified without written permission from the American Dental Hygienists’ Association.





{kind=link}