



Abstract
Purpose To evaluate changes in toothbrushing behavior and plaque removal performance with usage of a next generation oscillating-rotating electric toothbrush (NG-OR).
Methods This exploratory clinical study had a two-treatment, three-period, single-group, sequential design. Generally healthy adults with a screening whole mouth mean Turesky modified Quigley-Hein Plaque Index (TQHPI) score of at least 1.75 on a 0-5 scale and who were primarily OR brush users were enrolled. Participants used each OR toothbrush in A-B-B order, where a currently marketed OR brush with a traditional mechanical drive system (T-OR) was used in period A and the NG-OR brush with a linear magnetic drive was used in period B. At Visit 1, qualifying participants brushed on-site with T-OR. After a 48h washout, participants returned for Visit 2 and brushed on-site with NG-OR. Participants then used NG-OR for 1 week, twice daily, at home and returned for Visit 3 to brush on-site with NG-OR again. For all on-site brushings, participants were instructed to brush for 2min without interactive features. Each toothbrush was tagged with a transmitter chip connected to a Motion Tracking System to record movements of the toothbrush and participant using infrared light transmission to determine Isochronicity (brushing time uniformly distributed across the dentition). Plaque was measured using TQHPI. Primary variables were Isochronicity and TQHPl whole mouth mean plaque reduction (pre-brushing minus post brushing).
Results Overall, 41 participants enrolled and received treatment; 40 completed the trial. NG-OR showed significantly greater Isochronicity after a single brushing (p=0.043) and after a 1-week at-home use (p=0.001) versus T-OR. NG-OR showed 41% greater whole mouth plaque removal than T-OR (p<0.001) after a single brushing. Plaque reduction by region/surface was consistent with whole mouth results.
Conclusion The NG-OR brush showed greater brushing uniformity and plaque removal versus the T-OR brush.
INTRODUCTION
The cornerstone of oral hygiene instruction is thorough toothbrushing with a fluoride toothpaste for 2min, twice daily.1,2 However, manual brush usage consistently leaves plaque behind. A systematic review of 59 studies evaluating 212 separate brushing exercises among more than 10,000 participants showed that, on average, using a manual toothbrush only reduces plaque scores by 42% following a brushing exercise.3 Undisturbed plaque biofilm produces a more pathogenic microbiome, increasing the patient’s risk for oral disease with possible systemic implications longer term.4 Manual brush users, when they switch to electric, typically improve plaque removal due to technology but may still keep (inadequate) brushing habits, in particular missing inside surfaces. In an observational trial, nearly all participants (96.8%) reached all vestibular surfaces when using a power toothbrush, but only 58.9% of participants reached all oral/lingual surfaces.5
One factor linked to an individual’s capability to achieve post-brushing oral cleanliness, as assessed by plaque evaluation, is even distribution of brushing time.6 Interestingly, even when study participants are asked to brush to the best of their abilities, their increased effort does not result in greater attention to all surfaces.7 Lingual surfaces are still overlooked.7 In an effort to promote more uniform brushing across the dentition, along with other desired brushing behaviors (e.g. proper pressure, duration), electric toothbrush manufactures have incorporated features such as quadrant timers, visual displays, and coaching apps through the years.8-11 These elements provide sensory cues to guide individuals to brush evenly and thoroughly across the dentition.
Despite this longstanding recommendation from dental professionals, inconsistent patient behavior is common and can lead to suboptimal plaque control.12 Implementing successful interventions to improve patients’ daily plaque control via effective toothbrushing is an ongoing challenge for dental hygienists. Brushing behaviors are multifaceted, impacted by factors such as patient motivation, knowledge of and ability to perform proper brushing technique, and sensorial aspects of toothbrushing.13 Psychological evidence suggests brushing changes to oral health routines be composed of both habit and intention-based interactions.14 This same study demonstrated the importance of effective aspects of brushing behavior and the potential to incorporate sensor based objective measures in future research.14
In 2020, a next generation oscillating-rotating (NG-OR) electric toothbrush was introduced. This toothbrush has a linear magnetic drive that directs motor energy directly to the bristle tips, producing oscillation-rotations with micro-vibrations. The NG-OR provides an acoustically-optimized, unique sensory experience compared to traditional OR models8 while demonstrating gingival health and plaque removal benefits compared to manual and sonic control brushes.15-19 The NG-OR also has features to encourage recommended brushing behaviors, including sensor-mediated Position Detection via an app. Notably, data from multiple clinical trials show disproportionately greater plaque removal and gingival bleeding reductions in lingual surfaces when subjects used the NG-OR, even without use of the app, compared to manual and sonic toothbrush controls.15-19 This finding suggests there may be other brush phenomena impacting efficiency.
As a first step in understanding the basis for the disproportionate efficacy in lingual areas, this clinical trial was undertaken to explore one aspect of toothbrushing behavior, uniformity of brushing time across the dentition (Isochronicity), along with plaque removal performance associated with usage of the NG-OR. Isochronicity was prioritized for evaluation first over other potential influences (e.g. brushing sensation, auditory cues) because of accessibility to the objective, validated Motion Tracking methodology.20 Methodological research previously confirmed that Motion Tracking provides comparable data to Video Observation, a gold standard tool to assess the Toothbrushing Systematic Index, of which Isochronicity has been determined to be the clinically relevant component.
METHODS
This exploratory clinical study was conducted at the Consumer Product Research Center, Procter & Gamble Innovation Center (Kronberg, Germany) from September 2021 to March 2022 in accordance with the International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use–Good Clinical Practices as published by the FDA, with the Commission Directive 2005/28/EC published by the European Union, and ISO 14155:2011. The study protocol and all study-related documents were reviewed and approved by the Ethics-Commission of the Landeszahnärztekammer Hessen Institutional Review Board. Participation was voluntary; there was no penalty for withdrawing from the study. The study was registered in the ISRCTN registry (ISRCTN99464691). All participants provided written, informed consent.
Participants
Participants were recruited between September 2021 and February 2022, primarily from the principal investigator’s practice, either in-person (at the practice) or by phone. Due to difficulties recruiting during COVID, the population was supplemented by recruiting from an existing plaque panel at the Consumer Product Research Center in Kronberg, Germany by phone. They were generally healthy adults, 18 years of age or older, who normally used an Oral-B OR toothbrush, either exclusively or with another brush type (e.g. manual or sonic), and had a screening whole mouth mean Turesky modified Quigley-Hein Plaque Index (TQHPI; described in Assessments) score of at least 1.75. Other inclusion criteria included possessing a minimum of 16 scorable teeth with facial and lingual scorable surfaces; maxillary and mandibular second molars on both sides; at least four maxillary and mandibular anterior teeth; and balanced distribution of teeth between the quadrants. Participants agreed to refrain from all oral hygiene procedures for approximately 24h prior to all visits; to refrain from eating, chewing gum and any tobacco use for at least 2h, with only small sips of water up until 45 mins, prior to all visits; not to participate in any other oral care study for the duration of this study; to delay any elective dentistry, including dental prophylaxis, until study completion; and to refrain from using any non-study oral hygiene products, other than their usual at-home toothbrush and toothpaste between Screening and Visit 1 and between Visit 1 and Visit 2.
Participants were excluded if there was evidence of carious lesions requiring restorative treatment; active treatment for periodontitis; fixed orthodontic appliances on the facial surface of anterior teeth; a removable denture; use of antibiotics or chlorhexidine mouth rinse within 2 weeks prior to the study; or presence of any disease or condition that could interfere with examination procedures or with the participant safely completing the study as determined by the investigator.
Study Design
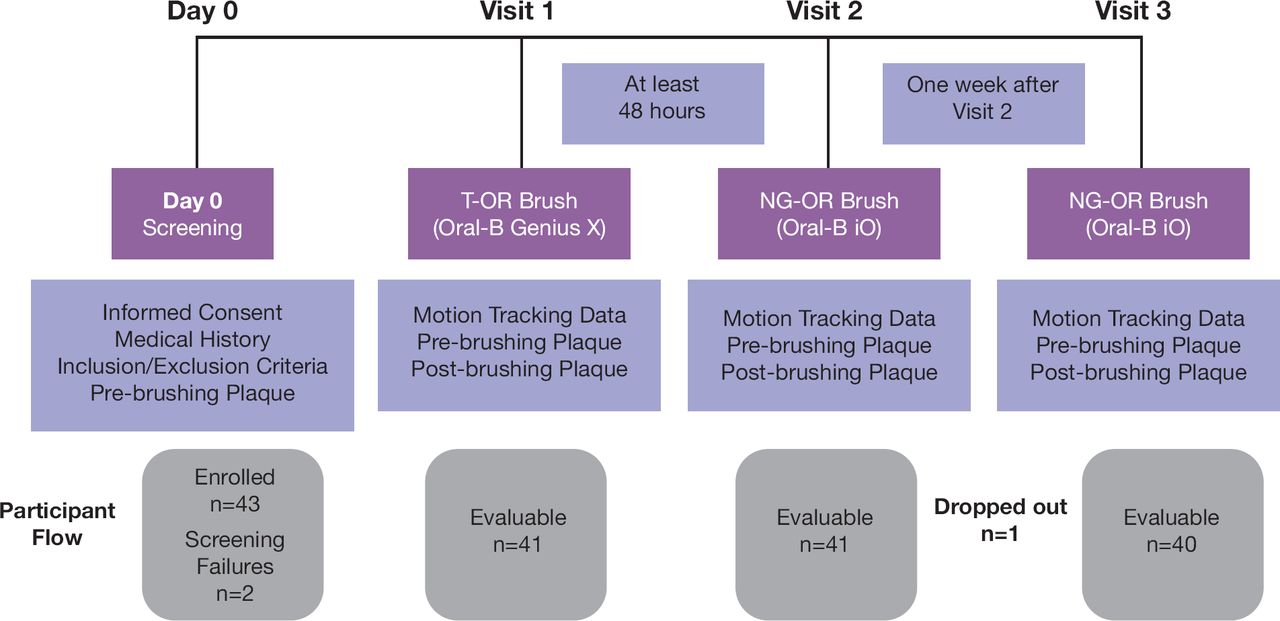
This exploratory study used a two-treatment, three-period, single-group, sequential clinical study design. Every participant in the study used each of the two OR electric rechargeables toothbrushes in an A-B-B order, where a marketed OR brush with a traditional mechanical drive system, Oral-B Genius X with CrossAction head (T-OR), was used in period A. The next generation OR brush with a linear magnetic drive, Oral-B iO with Ultimate Clean brush head (NG-OR), was used in period B (Figure 1). Toothbrushing was conducted with a standard sodium fluoride toothpaste (blend-a-med Classic, 1450 ppm F; Procter & Gamble, Cincinnati, OH, USA).
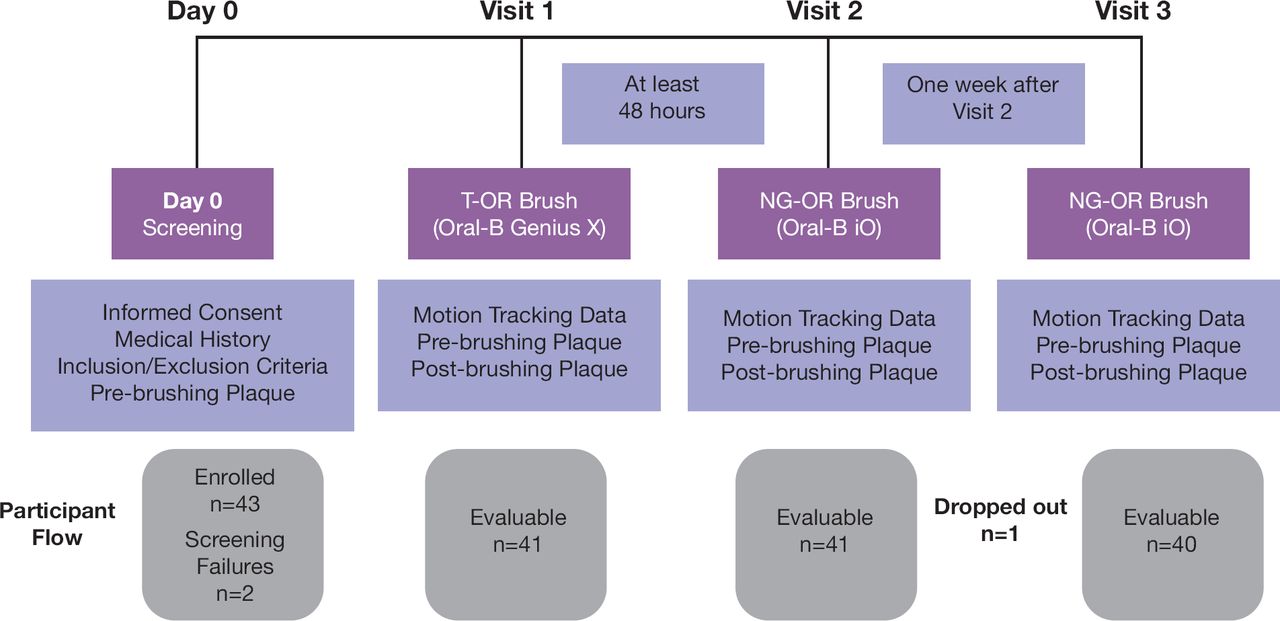
Study design and participant disposition at each visit
At the screening visit, participants were evaluated for plaque accumulation after refraining from all oral hygiene procedures for approximately 24h prior to the screening appointment. Participants provided informed consent, medical history information was obtained, and a pre-brushing oral examination of hard and soft tissues was conducted. Participants then self-disclosed plaque using Mira-2-Ton solution (Hager & Werken GmbH; Duisburg, DE) for 1min, after which a trained and experienced examiner15 (JE) conducted a pre-brushing plaque examination using the extended TQHPI.21,22 After the plaque examination, participants received the T-OR brush from site staff and brushed their teeth under supervision, but without Motion Tracking equipment attached to the brush. Participants meeting all inclusion criteria were enrolled in the study, which was conducted in different cohorts and scheduled for Visit 1. They were instructed to follow the same oral hygiene and eating restrictions employed with their screening visit.
At Visit 1, participants returned to the site and continuance criteria were assessed. A pre-brushing oral examination was conducted followed by a pre-brushing plaque examination. Participants then received the T-OR brush from site staff with the Motion Tracking system included, as described by Ganss and colleagues.20 Participants then brushed their teeth on site for 2min with the assigned brush following manufacturer’s instructions. Participants did not have access to a mirror while brushing, they did not use the app/interactivity, and they did not view any output or receive any guidance from the Motion Tracking system. No other brushing instructions were provided. The Motion Tracking system recorded all toothbrush movements and the participant‘s movements, when brushing, allowing absolute positioning of the toothbrush in the mouth at a given time. After toothbrushing, participants received post-brushing oral and plaque examinations by an examiner in an area separated from toothbrushing to mitigate the examiner’s awareness of the intervention. Self-reported and/or observed Adverse Events (AEs) were recorded. There was a wash-out period of at least 48h between Visits 1 and 2 during which participants used their usual toothbrush and toothpaste. Participants were reminded of the standard oral hygiene and eating restrictions prior to Visit 2.
Visit 2 followed the same procedures as Visit 1, except participants brushed with the NG-OR brush on site. Participants were then given the NG-OR brush, charger, and toothpaste by site staff to take home. They used the NG-OR brush at home for 1 week, brushing twice per day (morning and evening) for 2min per brushing, with the same sodium fluoride toothpaste used on site. No other oral care products were permitted to be used. Participants were reminded of the standard oral hygiene and eating restrictions prior to Visit 3.
At Visit 3, participants returned to the site and conducted the last assessment with the NG-OR brush, following the same procedures as Visits 1 and 2. Product was returned and visually inspected. Compensation was provided at the end of the trial.
Assessments
The extended TQHPI was used to score plaque deposits at six sites (distobuccal, midbuccal, mesiobuccal, distolingual, midlingual and mesiolingual) of each tooth, excluding third molars, crowns and surfaces with cervical restorations.21,22 Scores range from 0 to 5, with 5 indicating higher plaque (Appendix 1). Buccal, lingual, and whole mouth average plaque scores were calculated for each participant and tooth surfaces by totaling the scores and dividing by the number of gradable sites.
For each participant and visit, Isochronicity (I) was computed as.

n =total number of reachable areas in the mouth,
di =brushing duration within an area in seconds,
x =total brushing duration in seconds.
Isochronicity considers the distribution of the brushing duration by the mean absolute deviation of the relative brushing duration based on vestibular and oral surfaces (12 areas: mandibular/maxillary, left/right/center, lingual/buccal) only, ignoring occlusal/incisal brushing. Isochronicity scores range from 0 to 1 with higher scores indicating greater uniformity.23
Statistical Methods
Based on a previous pilot study, 45 participants were to be enrolled with 40 evaluable participants providing at least 90% power to detect a mean difference in plaque reductions between visits (e.g. Visit 2 mean [pre minus post] - Visit 1 mean [pre minus post]) of 0.27 units using a standard deviation of 0.188.
The primary variables, Isochronicity (uniform brushing across the mouth) and TQHPl whole mouth mean plaque reduction (pre-brushing minus post-brushing), were compared across visits to understand uniformity changes and plaque differences. Plaque reduction (pre-brushing minus post-brushing) by region and surface was also assessed as a secondary analysis. For all primary and secondary analyses, comparisons across visits were calculated as follows:
Visit 1 versus Visit 2: First use brush difference: T-OR versus NG-OR after first use.
Visit 2 versus Visit 3: NG-OR behavior change: NG-OR after 1week of use versus NG-OR after first use.
Visit 1 versus Visit 3: Overall brush differences: T-OR versus NG-OR after 1week of use
Both Isochronicity and plaque data were normally distributed, and the above comparisons were carried out using a paired t-test. Additionally, the pre-brushing and post-brushing plaque values were summarized and compared across visits. Visit comparisons were two-sided tests carried out at the 10% significance level. All analyses were conducted using SAS 9.4 (SAS Institute; Cary, NC, USA).
RESULTS
Forty-three participants were enrolled, 41 received treatment, and 40 completed the study. Two participants dropped out as screening failures, and one dropped out before the last visit due to a scheduling conflict. Participants’ mean age was 47.2 years and 56% were female. Sixty-one percent of participants were exclusive OR users, and 39% primarily used an OR toothbrush but also used a manual or sonic toothbrush (Table I).
Demographics summary (n=41)
Isochronicity
The average Isochronicity scores were 0.71 at Visit 1, 0.73 at Visit 2 and 0.75 at Visit 3. See Table II. The comparison between Isochronicity at Visit 1 (T-OR brush) and Visit 2 (1st use of NG-OR brush) showed a statistically significant difference of 0.027 (p=0.043), with the NG-OR brush having higher Isochronicity, indicating more uniform brushing across areas. The comparison between Isochronicity at Visit 2 (1st use of NG-OR brush) and Visit 3 (NG-OR brush after 1week home use) showed a statistically significant difference of 0.025 (p=0.028), with the NG-OR brush having higher Isochronicity or more uniform brushing after having 1week familiarization at home. The comparison between Isochronicity at Visit 1 (T-OR brush) and Visit 3 (NG-OR brush after 1week home use) showed a statistically significant difference of 0.052 (p<0.001), with the NG-OR brush after 1week of familiarization at home resulting in higher Isochronicity.
Isochronicity Results
Plaque
The pre-brushing whole mouth mean TQHPI scores were 3.62 at Visit 1, 3.55 at Visit 2 and 2.36 at Visit 3. The pre-brushing whole mouth mean TQHPI for the T-OR brush at Visit 1 was statistically significantly higher than the plaque score for the NG-OR brush at Visit 3 (p<0.001). Additionally, the pre-brushing plaque score for the NG-OR brush at Visit 3, after 1 week of use, was statistically significantly lower (p<0.001) than after the first brushing (Visit 2).
The post-brushing whole mouth mean TQHPI scores were 2.33 at Visit 1, 1.73 at Visit 2, and 1.13 at Visit 3, representing plaque reductions of 36%, 52% and 52%, respectively. The post-brushing whole mouth mean TQHPI for the T-OR brush at Visit 1 was statistically significantly higher than the plaque scores for the NG-OR brush at Visits 2 (first use of NG-OR brush) (p<0.001) and 3 (after 1 week use of NG-OR brush) (p<0.001). Additionally, the post-brushing plaque score for the NG-OR brush at Visit 3, after 1 week of use, was statistically significantly lower (p<0.001) than after the first use of brushing (Visit 2). Table III shows the pre- and post-brushing mean plaque scores and the plaque reduction over time for the different brushes/visits.
Whole Mouth Plaque Results
The comparison between whole mouth mean TQHPI reduction of Visit 1 (T-OR brush) and Visit 2 (NG-OR brush) showed a statistically significant difference of 0.52 (p<0.001), representing 41% greater plaque removal for the NG-OR brush after the first brushing (Table III). The comparison between whole mouth mean TQHPI reduction of Visit 2 (1st use of NG-OR brush) and Visit 3 (NG-OR brush after 1 week home use) and between Visit 1 (T-OR brush) and Visit 3 (NG-OR brush after 1 week home use) were not relevant since the pre-brushing plaque score at Visit 3 was significantly lower than pre-brushing score at Visit 1 and Visit 2, which influences the reduction at Visit 3.
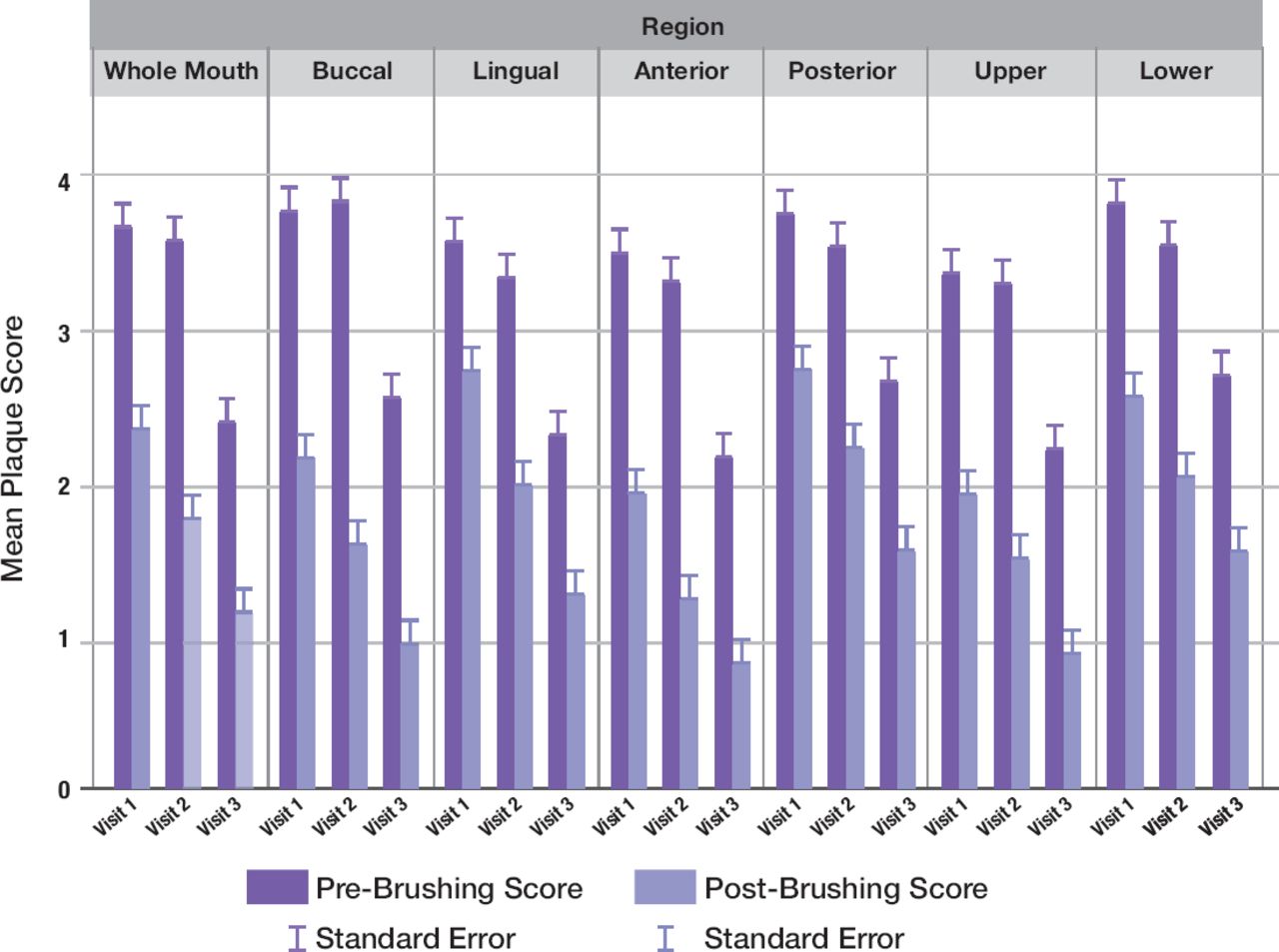
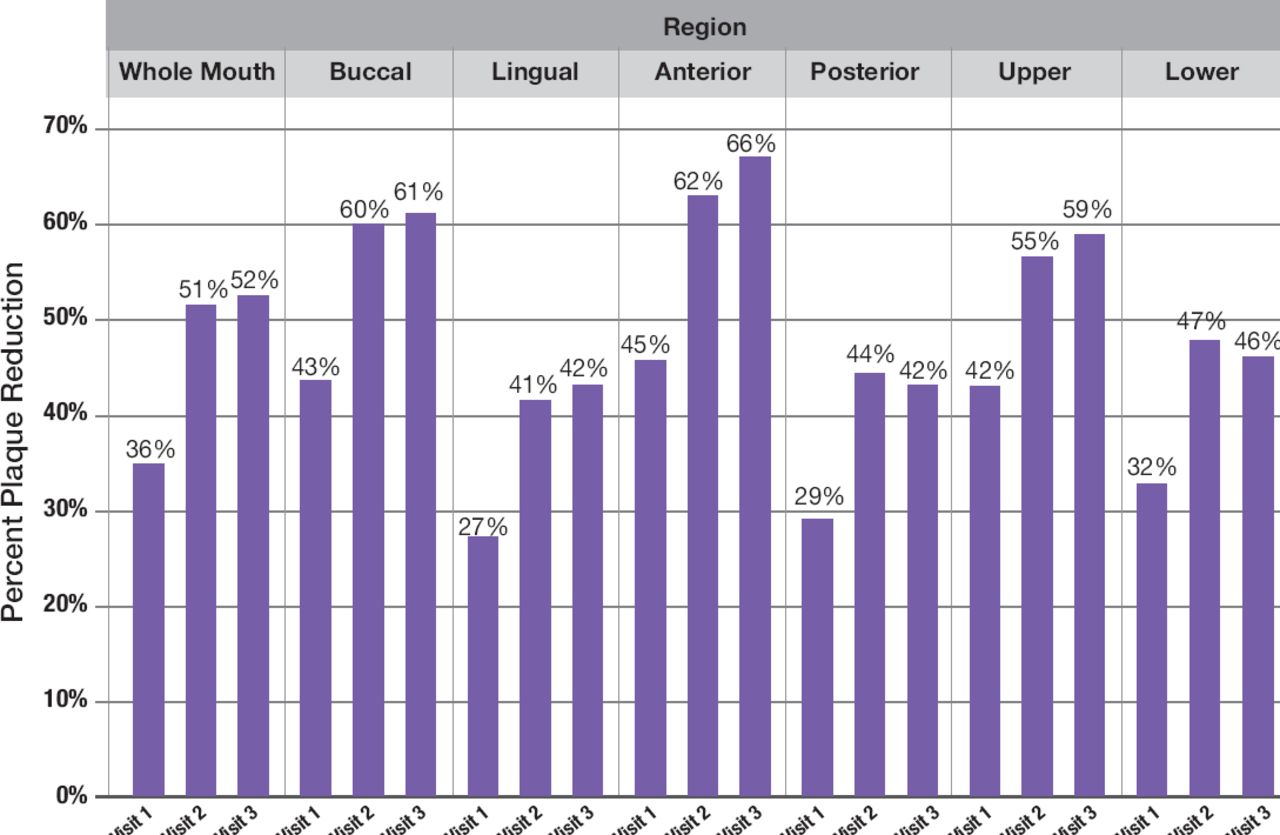
The supplementary Figure 1a and 1b shows pre- and post-brushing mean plaque scores and percent plaque reductions by region and surface across all visits. For all analyses by region and surface, plaque reduction comparisons between visits followed the same pattern for statistical significance as whole mouth plaque results described above. Specifically, percent plaque reductions were greater for Visits 2 and 3 with the NG-OR brush compared with Visit 1 with the T-OR. These results were similar to Isochronicity findings in that the NG-OR brush demonstrated more uniform brushing than the T-OR brush.
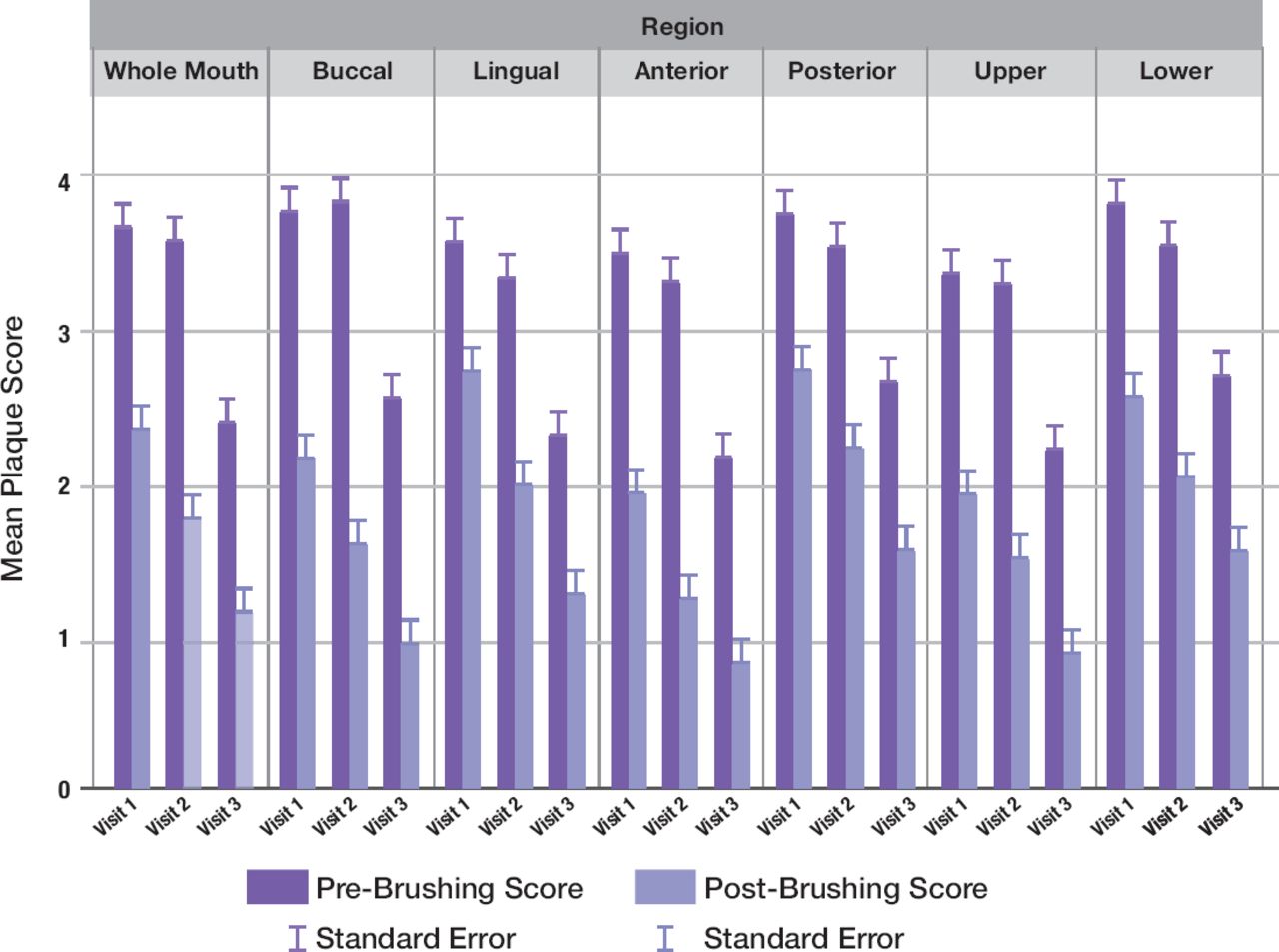
Mean pre-and post-brushing plaque scores by region and surface across visits.
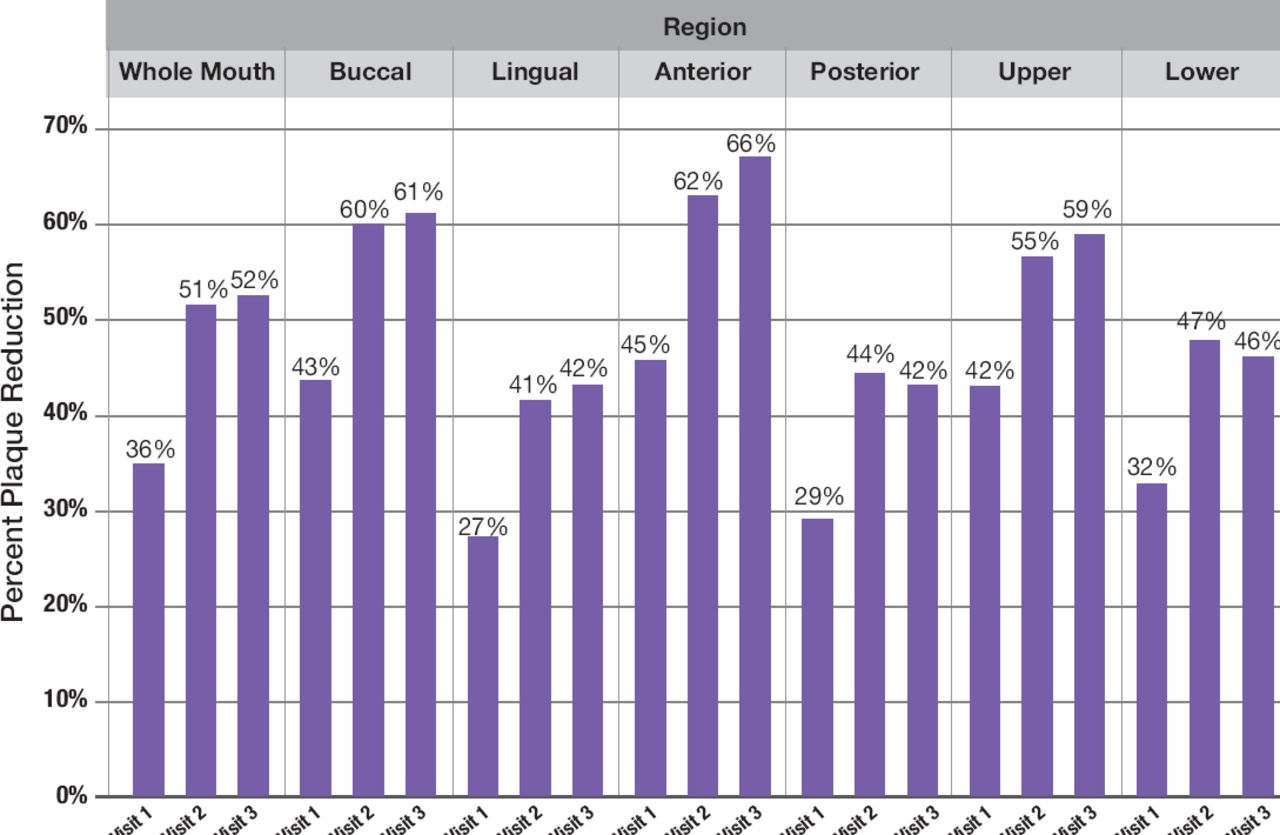
Percent plaque reduction by region and surface across visits
One Adverse Event, categorized as dental restoration damage, was reported in the study. It was mild in severity and not related to treatment.
DISCUSSION
This two-treatment, three-period, single-group, sequential exploratory clinical trial demonstrates superiority for the NG-OR brush compared to the marketed T-OR brush for brushing uniformity as well as plaque reduction. The NG-OR brush showed greater Isochronicity, a measure of brushing evenness across the dentition, compared to the T-OR brush after a single-brushing, with this benefit increasing after 1-week of at-home use. The first use of the NG-OR brush also showed lower plaque levels compared to the T-OR brush, with even lower plaque levels observed after using the NG-OR brush for a week. Plaque scores across sub-regions were consistent with whole mouth results, in accordance with Isochronicity findings. All participants who received treatment completed the trial, with the exception of one participant who dropped out between Visits 2 and 3 due to a scheduling conflict.
The Isochronicity findings corroborate previously published studies, ranging in duration from single-brushing to 6-months, showing the NG-OR brush provides disproportionate benefits in lingual regions compared to manual and sonic controls.15-19 In one study, the NG-OR brush showed a 70.3% greater reduction relative to a manual brush for whole mouth plaque yet a 102.9% greater reduction for lingual surfaces.15 Collectively, these findings indicate brushing behavior improvements with the NG-OR brush that are independent from its interactive coaching features. The magnetic drive technology of the NG-OR brush enables a more frictionless and direct energy transfer to the bristles than the T-OR brush, which has a traditional mechanical drive system. The authors hypothesize that the Isochronicity benefit associated with the NG-OR brush may be related to changes in habit, intention and attitudes, possibly driven by mouthfeel aspects associated with micro-vibrations (e.g. gliding sensation) and/or different sensory qualities (e.g. auditory) of the brushing experience,13 but the psychological impacts are unknown and should be more fully researched.
Another notable finding is the enhanced plaque removal exhibited by the NG-OR brush relative to the T-OR. While both toothbrushes are based on OR technology, which has been shown to provide gingival health advantages over manual and sonic toothbrush controls,24-28 the novel drive system of the NG-OR brush eliminates intrinsic losses of energy that are incurred with use of the mechanical drive system in the T-OR and the NG-OR brush has a higher frequency of brush rotations. A recent meta-analysis of 26 RCTs with over 3000 subjects confirms plaque removal and gingival health efficacy advantages for the NG-OR brush over traditional OR models like the T-OR brush.29 The meta-analysis showed that across the studies, 88% of subjects using the NG-OR brush transitioned from baseline gingivitis to a state of gingival health compared with 65% of subjects using a traditional O-R model.
Lack of access to care and use of oral healthcare services vary based on social determinants of health. In these cases, having the option to improve oral health outcomes without person-to-provider interactions is desirable. In this trial, participants improved brushing uniformity and plaque removal when switching from the T-OR brush to the NG-OR brush without additional oral hygiene instruction. This was true regardless of whether patients were previously exclusively OR toothbrush users or primarily OR users who used other toothbrush types as well (manual, sonic). This suggests that recommending the NG-OR brush to patients, regardless of their usual brush type, may result in a positive change in brushing behavior and plaque control that is consistent with the principles of oral hygiene instruction. These learnings illustrate the opportunity that home-care technologies offer to consolidate professional instruction and reinforce desired oral hygiene behaviors.
Strengths and Limitations
A key strength of this trial was use of the Motion Tracking methodology, which is a validated approach to assess toothbrush behaviors in clinical research. Ganss and colleagues demonstrated that Motion Tracking mirrors observations from the gold standard video observation methodology, while offering efficiency advantages.20 Furthermore, this investigation did not involve interactivity features of the brush (e.g. visual coaching) so it assessed changes in brushing behavior based solely on properties of the toothbrush. A limitation of this research is the potential for the Hawthorne effect given subjects knew their toothbrushing behavior was being tracked. However, the consistent plaque removal advantages for NG-OR seen in this trial and a recent meta-analysis suggest otherwise.29 Another limitation is the non-randomized study design, though a traditional crossover design could have had potential carryover effects that might influence the treatment.
There are opportunities to expand upon these learnings in future research. The trial could be repeated using a longer assessment period, different toothbrushes, specific patient groups (e.g. pediatric patients, dexterity or brushing-compromised), and/or interactive coaching features. A randomized trial, if carefully designed, may provide additional insights along with assessments of intrinsic motivation and/or autonomous behavior.
CONCLUSION
In this two-treatment, three-period, single-group, sequential design exploratory clinical study, the NG-OR brush showed greater Isochronicity, indicating more uniform brushing, and greater plaque removal versus the T-OR brush. The benefits of the NG-OR brush were demonstrated after a single brushing and increased over the 1-week usage period.
ACKNOWLEDGEMENTS
The authors thank Magdalena Czapp Zakrewski, Julia Raitz von Frentz, and Phyllis Hoke for their contributions to this research.
Appendix 1. Turesky modified Quigley-Hein Plaque Index

0 = No plaque
1 = Separate flecks of plaque at the cervical margin
2 = A thin, continuous band of plaque (up to 1 mm) at the cervical margin
3 = A band of plaque wider than 1 mm, but covering less than one third of the side of the crown of the tooth
4 = Plaque covering at least one third, but less than two thirds of the side of the crown of the tooth
5 = Plaque covering two thirds or more of the side of the crown of the tooth
Image originally published in: Klukowska M, Grender JM, Conde E, et al. Plaque reduction efficacy of an oscillating-rotating power brush with a novel brush head utilizing angled bristle tufts. Compendium. 2014;35(9). Copyright© 2023 to BroadcastMed LLC. All rights reserved. Used with permission of the publisher.
Footnotes
NDHRA priority area, Client level: Oral health care (health promotion: treatments, behaviors, products).
DISCLOSURES
Ralf Adam, Yuanshu Zou, Julie Grender, Uta Mesples, and Jasmin Erb are employees of Procter & Gamble. Kimberly K. Bray is a member of the P&G Advisory Board. This study was funded by Procter & Gamble.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study may be available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
- Received April 28, 2023.
- Accepted August 20, 2023.
- Copyright © 2023 The American Dental Hygienists’ Association
This article is open access and may not be copied, distributed or modified without written permission from the American Dental Hygienists’ Association.





{kind=link}
{kind=link}
{kind=link}
{kind=link}