



Abstract
Purpose: The demand for esthetic dentistry has led to the development of new treatments for white spot lesions (WSLs). Microinvasive therapies, such as resin infiltration, have been used to treat demineralized enamel. Recently, resin infiltration using the active ingredient triethylene glycol dimethacrylate (TEGDMA), has been used to restore WSLs. The purpose of this narrative review is to evaluate the evidence on TEGDMA, an innovative resin that has been introduced, as an alternative dental material for treating WSLs.
Methods: A review of the literature was conducted using key words pertaining to WSLs and resin infiltration including cosmetic dentistry; dental caries; dental materials; general dentistry; sealants; technology for patient care. Evidence was incorporated from biomedical data bases including PubMed and the Cochrane Library, which formed the framework for the review.
Results: Based on the synthesis of the evidence, resin infiltration using TEGDMA is an effective alternative treatment option for WSLs. Studies suggest that the outcomes for micro-invasive procedures using resin infiltration may vary depending on the depth of the lesion.
Conclusions: Resin infiltration, using TEGDMA, removes minimal amounts of enamel and preserves the hard tissue surrounding the WSLs. Additionally, TEGDMA restores the natural fluorescence, hardness, and texture of intact enamel. Future studies are needed to assess the long-term clinical effects of resin infiltration using this material on both permanent and primary dentition.
- white spot lesions
- demineralized enamel
- triethylene glycol dimethacrylate
- resin infiltration
- micro-invasive dentistry
- cosmetic dentistry
Introduction
White spot lesions (WSLs) are the first sign of a subsurface enamel porosity due to demineralization.1 These lesions exhibit an opacity on the tooth surface and contribute to esthetic complications.1 Demineralization can occur as a result of several intrinsic (ie hypocalcification; fluorosis), as well as, extrinsic (biofilm accumulation; orthodontic brackets; extended exposure to bacteria) factors.2,3 Prolonged biofilm accumulation allows the acidic byproducts from the bacteria to create micro-porosities within the enamel surface, which results in the development of WSLs.3 When the acid challenge is removed, saliva becomes saturated in calcium and phosphate allowing the ions to be reabsorbed into the demineralized area, resulting in net mineral gain and repair of the hydroxyapatite structure.4
White spot lesions are commonly seen on the facial surfaces of enamel, resulting in an increased concern for esthetics. These lesions may appear as irregular, milky-white opacities on the surface of enamel.3 Patients with fixed orthodontic brackets are at higher risk for experiencing enamel demineralization. This is especially evident in orthodontic patients with poor oral hygiene practices, which can lead to the development of a WSL.3 White spot lesions that form during orthodontic treatment can become problematic for both patients and oral health care providers.
White spot lesions have been treated with a variety of modalities including dietary interventions, topical fluoride products, and microabrasion.1 Although dietary control is effective for prevention, it does not directly reverse the effects of WSLs once formed. Fluoride has been shown to reduce caries in both permanent and primary dentitions by remineralizing tooth surfaces depleted of minerals, such as a WSL.1 Self-care methods of delivery include dentifrices and oral rinses that contain fluoride. Professionally applied methods include fluoride gels, varnishes, and silver diamine fluoride products. Microabrasion has been shown to improve the appearance of WSLs by removing the defective outer layer of enamel using chemical erosion and mechanical abrasion.5 Minimally invasive removal of enamel allows for the possibility of remineralization, allowing saliva to reach deeper into the enamel surface and restore the WSL over time.5 However, if a WSL is left untreated, it may reach the clinical end point of cavitation, and require a more invasive approach including resin-based restorative materials, porcelain veneers, or crowns. While restorative treatments like crowns and veneers must be provided by a licensed dentist, treatment with resin infiltration may be performed by a licensed dental hygienist.
Micro-invasive strategies such as pit and fissure sealants and resin infiltration have been used to arrest early cavitated lesions.1 Components used in pit and fissure sealants include resin materials and glass ionomer cements.1 Sealants are applied onto phosphoric acid-etched enamel to act as a barrier between the susceptible tooth surface and acid production, therefore preventing mineral loss from the tooth. Resin infiltration uses low-viscosity light cured resin to treat WSLs. The technique allows the resin to permeate into the hydrochloric acid-etched WSL by capillary action and stops the progression of demineralization by obstructing the pathway of acids produced by bacteria.6,7 Research has shown that the infusion of the resin into the pores of the tooth, also replaces lost tooth structure and improves the esthetic appearance of the WSL.8
Numerous studies have been conducted to determine the effectiveness of resin infiltration compared to other restorative treatments on WSLs. Recently, a resin infiltration method using the active ingredient triethylene glycol dimethacrylate (TEGDMA), has been used to restore WSLs.2,9,10,11 Currently, there are limited studies that synthesize published data on TEGDMA, comparing it to various other therapeutic and preventive modalities for WSLs. The purpose of this narrative review is to evaluate the evidence on TEGDMA, an innovative resin, as an alternative dental material for treating WSLs.
Methods
A narrative review using deductive reasoning was used to gather evidence related to the topic. Search strategies used in formulating this narrative review were scientific data bases such as PubMed and the Cochrane Library, limiting the criteria to articles that have been published within the last five years. Key words such as cosmetic dentistry; dental caries; dental materials; general dentistry; sealants; technology for patient care, were used to find randomized control trials and systematic reviews on this topic. The strengths of the evidence used in this review were based on the articles’ validity and reliability.
Results
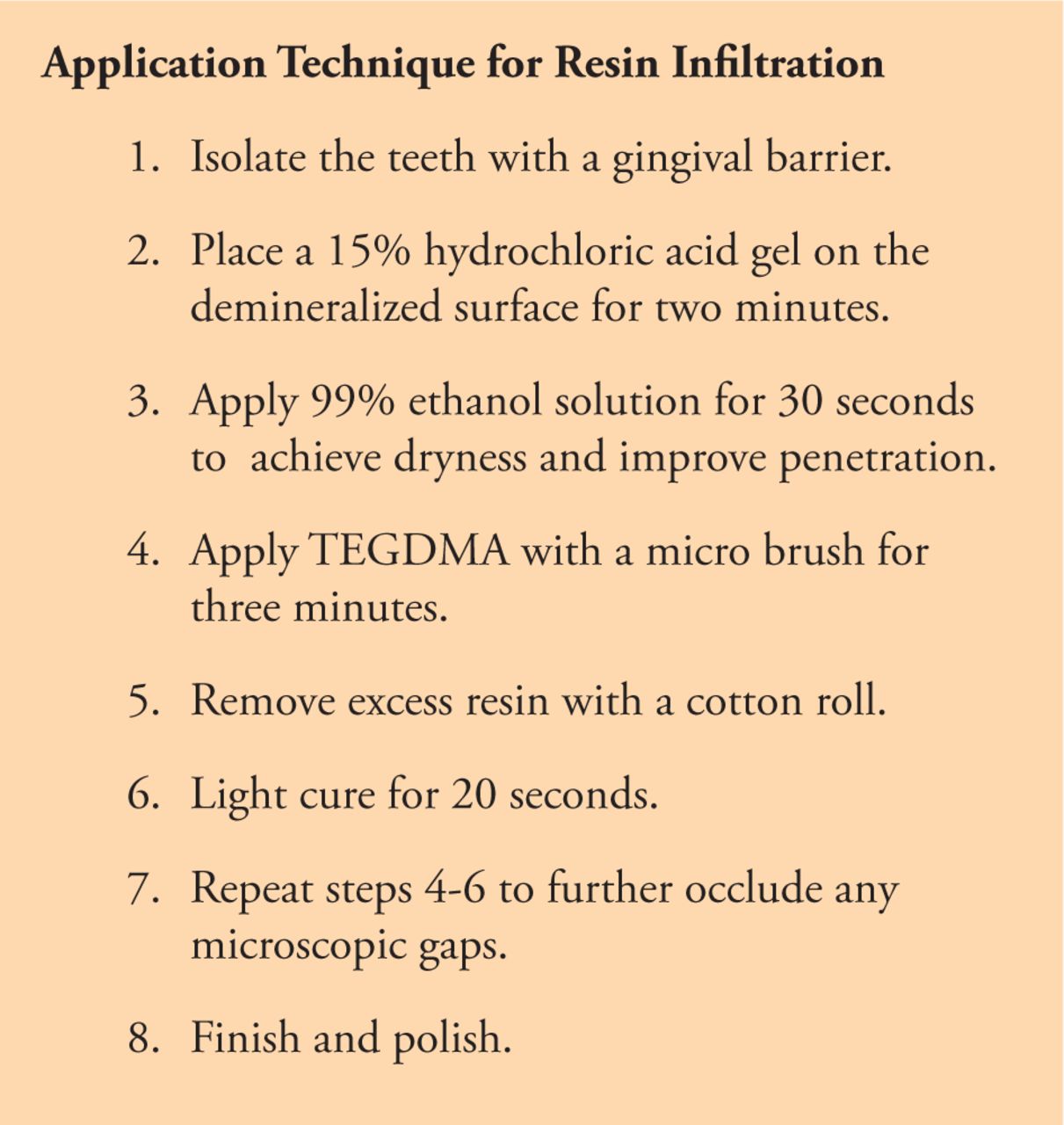
Research has examined how effective resin infiltration penetrates within the enamel.9 Depth of resin penetration could be a key determining factor for the creation of a diffusion barrier and the esthetic effects of resin infiltration.9 In a study by Paris et al. seventy extracted human teeth (n=70) were classified according to the International Caries Detection and Assessment System (ICDAS).12 Half of each tooth was etched with 37% phosphoric acid, the same type of etchant used to prepare the tooth surface for sealants.12 The other half was etched with 15% hydrochloric acid, the etchant used to prepare a demineralized lesion for resin infiltration.12 It was found that etching with 15% hydrochloric acid gel for two minutes eroded the ≤50 μm surface layer sufficiently, which resulted in nearly complete penetration of the resin.12 In contrast, 37% phosphoric acid eroded less sufficiently and resulted in reduced penetration depths, at a level that was both clinically and statistically significant (p<0.05).12 Resin infiltration has also been shown to penetrate deeper with the use of 15% hydrochloric acid etchant, when compared to treatments using fluoride or casein phosphopeptide with the use of a 37% phosphoric acid etchant.13
Triethylene glycol dimethacrylate resin can be infiltrated into hypomineralized enamel, which masks the white discoloration and produces a more uniform appearance of the enamel.1 In addition to improved esthetics, conclusions from a systematic review by Manoharan et al. reported that resin infiltration using TEGDMA did not induce post-operative sensitivity or pulpal inflammation.2 When the microscopic pores within the enamel were filled with the resin infiltrate, marginal gaps and leakage were no longer present, resulting in reduced sensitivity.2,14
A number of studies have reported that resin infiltration fills the micro-porosities and brings the tooth’s fluorescence, hardness, and texture back to values of sound enamel.2,10,15 An in vitro study by Markowitz and Carey used a fluorescent camera to assess the brightness intensity on extracted caries-free third molars.15 In this study, a 1mm x 4mm area on the facial surface was treated with lactic acid for two weeks to create a demineralized white spot lesion.15 Half of the lesion was then treated with resin infiltration and the other half was untouched. The fluorescent camera captured the ability of the resin to fill micro-porosities and mask white spot discoloration.15 Mean brightness intensity readings for intact enamel prior to treatment, after demineralization, and after treatment with resin infiltration were measured. Prior to resin infiltration, the brightness intensity value of intact enamel was 159.6.15 After the enamel was etched with lactic acid, the artificial white spot lesion showed a value of 123.4.15 Following resin infiltration therapy, the brightness intensity value was 160.9, which brought the value back to that of intact enamel, a finding suggesting that resin infiltration therapy has the potential to restore enamel to its original state, thus improving the appearance of WSLs.15
A study by Taher et al. evaluated resin infiltration therapy’s ability to restore the micro-hardness and texture of demineralized enamel.10 The hardness of caries-free extracted premolars (n=20) was measured using the Vicker’s surface hardness test before and after treatment with resin infiltration.10 It was found that the premolars treated with resin infiltration had approximately the same microhardness as sound enamel.10 In regards to texture, scanning electron microscopy was used to examine micro-porosities in enamel and it was found that the micro-porosities appeared occluded and the enamel surface was smooth following resin infiltration using TEGDMA.10 Findings from Taher et al. also suggest that resin infiltration has the ability to restore both hardness and texture back to that of intact enamel, thus restoring structure, function, and esthetics.10
Research studies have also examined the ability of resin infiltration to restore WSLs occuring during orthodontic treatment.5,16,17 Gu et al. conducted a randomized clinical trial on post-orthodontic patients who presented with WSLs to assess resin infiltration versus micro-abrasion on the improvement of WSLs.5 In this split-mouth design study, one side of the mouth was treated with resin infiltration, and the opposite side with microabrasion.5 A Crystaleye spectrophotometer was used to measure WSLs at different stages starting at baseline, one week, six months, and twelve months.5 The resin infiltration group showed a significant decrease in WSLs at one week (p<0.0001), however no significant changes were reported at six or twelve months (p=0.0549).5 Conversely, the micro-abrasion group showed a decrease in WSLs with a significant change from one week to six months (p=0.0003), but no significant difference from six to twelve months (p=0.0996).5 Gu et al. also found that resin infiltration was more effective in decreasing lesion size when compared to microabrasion, though no visual difference was observed between the two groups at the twelve month follow-up. Results showed that both treatments had similar masking of WSLs at twelve months; however, resin infiltration was found to be more effective for both immediate and long-term esthetics (p<0.001).5
Resin infiltration therapy has also been used to treat WSLs due to fluorosis. Garg et al. measured the effects of resin infiltration on three cases of mild to moderate fluorosis treated with resin infiltration using TEGDMA.11 In this study, eighteen fluoresced spots were measured using visual assessment with digital photographs, a colorimeter and spectrophotometer.11 The assessment tools were used at four different stages: pre-operative, post-bleaching prior to resin infiltration, post-infiltration, and at a twelve-month follow-up.11 It was found that 78% (n=14) of the WSLs treated with resin infiltration using TEGDMA, were within an acceptable range (p<0.001).11 The remaining 22% (n=4) were found to be unacceptable as the WSLs were not completely masked at the post-infiltration stage.11 However, at the twelve month stage, three of the four lesions improved and were found to be in the acceptable range, resulting in an overall success rate of 88%.11 Resin infiltration with TEGDMA was found to be significant in maintaining the appearance of WSLs for at least twelve months (p<0.001).11 All of the participants saw an improvement in the appearance of their teeth over the course of the study and reported an increase in their self-esteem.11
It is important to consider that the outcomes for micro-invasive procedures using resin infiltration may not always reach the desired esthetics. One limitation of resin infiltration is that optimal results are not permanent, therefore bleaching is recommended prior to resin infiltration and every 12-18 months thereafter to maintain the desired color of tooth structure.18 If an area of demineralization extends deep within the enamel, resin infiltration may not mask the WSL entirely. In order for resin to reach the full depth of the demineralized enamel, dental clinicians should apply the etchant for two minutes.2 Deeper enamel defects and demineralized WSLs previously treated with resin infiltration may be resistant to the etchant.2 Acid etching may be repeated in two-minute intervals up to two additional times to achieve the desired outcome.2
Medium-grit disks have been used to remove the superficial layer of enamel prior to resin infiltration.19 This step is often used on patients who have undergone resin infiltration therapy in the past, making their enamel surface more resistant to the etch.19 Although, the use of the disk would allow deeper penetration of the etch into the enamel surface, it may also have the potential to irreversibly remove a thin layer of tooth structure, making the treatment more invasive in some cases.19 The application technique for application of resin infiltration using TEGDMA adapted from Manoharan et al.2 is shown in Figure 1. An example of maxillary central incisors treated with resin infiltration is shown in Figure 2.
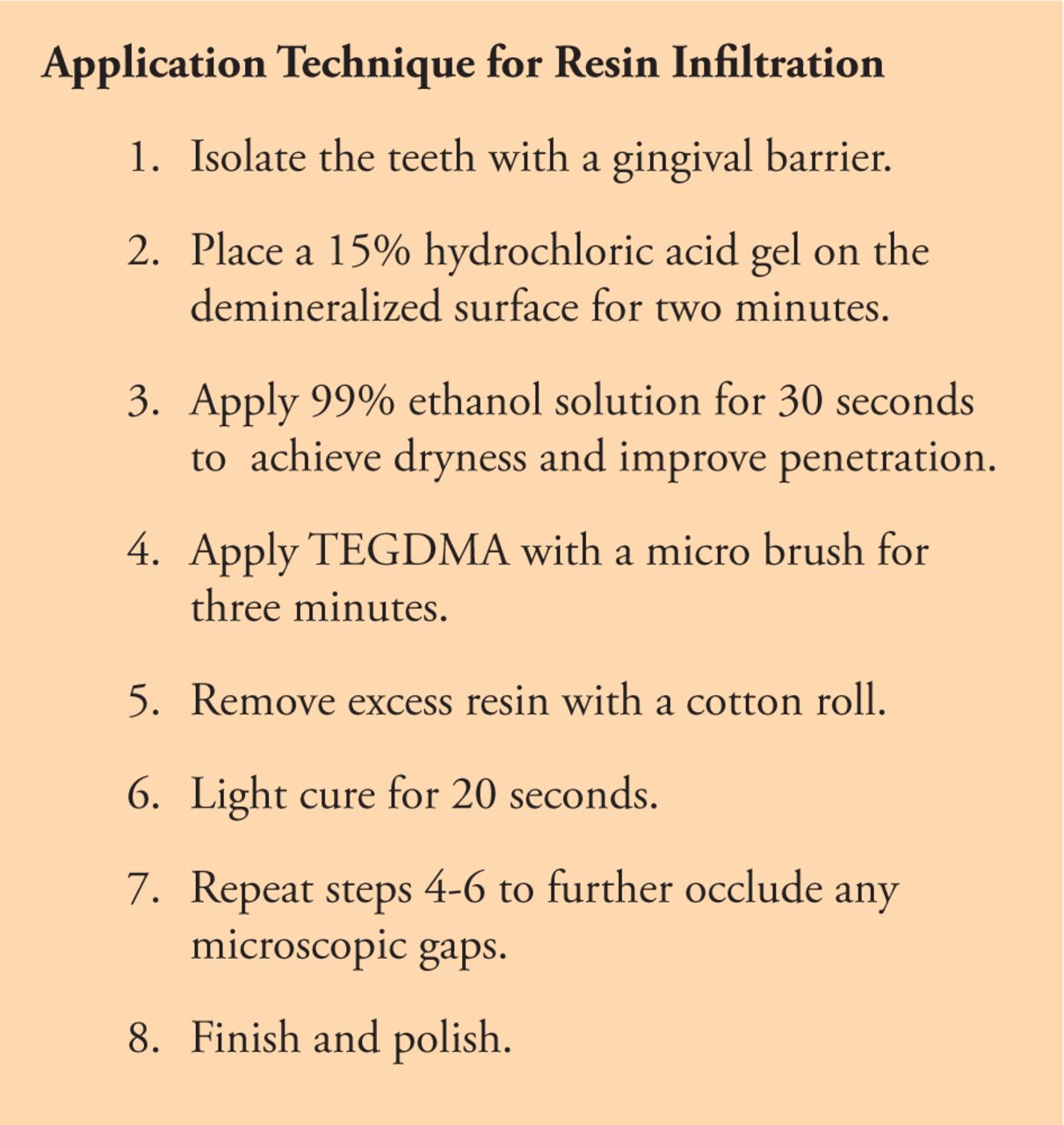
Resin infiltration technique using TEGDMA2

Before and after images of resin infiltration of the maxillary central incisors*
* Image courtesy of Shanae Lowrance, DDS; Lowrance Dental, Rockwall, TX, USA
It is important to note that there are differences in treating primary versus permanent teeth with resin infiltration.2 Primary enamel is less mineralized and more porous than permanent enamel, and as a result, the resin has been shown to have a greater diffusion coefficient when applied to primary enamel.2 In a study by Paris et al., confocal microscopic images were used to measure lesion and penetration depths of resin infiltration for both primary and permanent teeth.20 Primary teeth exhibited better penetration of the resin than permanent teeth after a one minute application of resin infiltration.20 Therefore, dental clinicians are encouraged to treat each case individually, and not adhere to a single protocol for application. The number of in vivo studies in the literature examining the long-term effects resin infiltration has on the esthetic appearance of the tooth of is limited, therefore more research is needed in this area.
Conclusion
Evidence suggests that resin infiltration using TEGDMA is an effective minimally invasive treatment option for WSLs. Resin infiltration, using TEGDMA has been shown to remove minimal amounts of enamel while preserving the hard tissue surrounding the WSL. Triethylene glycol dimethacrylate also restores the natural fluorescence, hardness, and texture of intact enamel. Future research is needed to assess the long-term effects of resin infiltration using TEGDMA and determine whether resin infiltration is effective in reducing the staining that can occur during tetracycline therapy and other etiologic factors that may lead to intrinsic staining. Further studies should also evaluate other newer restorative resin-based therapies that are being developed to treat WSLs.
This manuscript received the 2020 Sigma Phi Alpha undergraduate journalism award sponsored by:

Footnotes
This manuscript supports the NDHRA priority area, Client level: Oral health care (new therapies and prevention modalities).
- Received August 11, 2020.
- Accepted February 18, 2021.
- Copyright © 2021 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}