



Abstract
Purpose: Iowa is one of 42 states with a direct access dental hygiene workforce model. Public health supervision (PHS) in Iowa allows dental hygienists (DH) to provide services in community settings without a prior examination from a dentist. The purpose of this study was to assess the current PHS workforce in Iowa and add to the body of evidence on direct access DH care.
Methods: A 40-item mixed-mode survey was administered to all DH working under PHS in Iowa (n=126). Consent letters were mailed with directions to an online survey. Follow-up letters were sent to non-responders with an enclosed paper copy of the survey. Univariate analyses were performed to analyze the data.
Results: The response rate was 52% (n=62), with 69% (n=42) of participants currently providing services under PHS. The most common employer categories were local public health agencies (59%), community health centers (CHCs) (20%), and nonprofit clinics (10%). The most common types of services provided under PHS were dental screenings (95%), fluoride varnish (91%), and sealants (50%). The majority of supervising dentists worked in private practice (61%) and CHCs (27%). Most supervising dentists (71%) accepted some referrals; however, a majority of PHS participants (71%) reported that it was somewhat or very difficult to find dentists to accept patient referrals.
Conclusions: Most PHS DHs were employed by government agencies, however the majority of supervising dentists worked in private settings. Although most supervising dentists accepted at least some patient referrals, PHS DHs still experienced a high degree of difficulty referring patients for care.
- access to care
- direct access
- public health dental hygienists
- health disparities
- oral health
- workforce models
Introduction
Oral health is linked to overall systemic health, yet millions of Americans go without routine dental care each year.1 Dental diseases can be prevented or treated if a patient has access to dental healthcare professionals. However, accessing dental care can be difficult due to barriers including cost of care, language, fear, distance, taking time off work, or being under or uninsured.1 In addition to patient barriers, the dental workforce is often geographically maldistributed, with many counties having fewer than one dentist per 5,000 people, a threshold that classifies a county as a dental Health Professional Shortage Area (HPSA).2 It has been estimated that over 7,000 additional dentists would be needed in the United States (U.S.) to eliminate all dental HPSAs.3
As part of the solution to provider shortages and other barriers to care, many new workforce models have emerged that utilize non-dentist members of the oral health workforce. These workforce models include dental therapists, expanded function dental assistants, and direct access dental hygienists.4 Direct access models allow dental hygienists (DH) to provide services within their scope of practice without the need for a dentist to be physically present. This arrangement creates the opportunity for DHs to practice in community based settings in order to bring services closer to at-risk populations.2 This model also expands potential employment options for the dental hygiene workforce, which is increasingly a concern as national projections suggest that there will be more DHs than jobs available by 2025.3 To date, 42 states allow direct access to dental care.5 Within these direct access states, there is considerable variation in the types of allowable services as well as the level of supervision that is required under state scope of practice acts.6 Many states require a collaborative agreement with the supervising dentist, which sets guidelines and allows the DHs to see patients without prior dental exam or direct supervision, whereas some states allow DHs to practice fully independently.4 States also differ in the qualification requirements for providing direct access care. For example, Colorado has no additional requirements beyond an active license whereas Oregon requires 2,500 hours of supervised dental hygiene employment and 40 hours of approved continuing education credits.4
Iowa implemented a direct access model, public health supervision (PHS), in 2004. From 2004 to 2017, the size of Iowa’s PHS workforce grew from 14 to 95 DHs, making up approximately 5% of the total dental hygiene workforce in Iowa.7 To qualify as a PHS DH, a licensed DH is required to have a minimum of one-year clinical experience and a written supervision agreement with a dentist. This allows Iowa’s PHS DHs to provide services in community-based settings consistent with their supervision agreement and within their scope of practice.8 Iowa’s direct access requirements are much less extensive than other states’ as Iowa does not require a bachelor’s or master’s degree and there are no set clinical hour prerequisites.8 In addition, Iowa’s scope of practice guidelines for DHs have been identified as “satisfactory” with regard to how DHs can utilize their skills to improve access to care, on a continuum ranging from restrictive, limiting, satisfactory, favorable, or excellent.9 Iowa’s PHS DHs may perform screenings, communicate oral hygiene education, and provide therapeutic or preventive services such as oral prophylaxis or fluoride varnish, silver diamine fluoride, or sealant application.8 To date, no studies have been published on direct access DHs in Iowa.
Several studies have evaluated various aspects of direct access DHs.10-13 A qualitative study conducted in Massachusetts explored practice factors and participants’ attitudes about their work in public health and found that key barriers to success as public health DHs were Medicaid limitations, third party reimbursement restrictions, and issues finding a collaborative dentist.10 Two studies of Kansas’ extended care permit (ECP) model have explored attitudes and practice factors. A 2009 study showed that 60-70% of direct access respondents reported they disagree or strongly disagree that access to dental services for children, seniors, immigrants, special needs, and low-income populations is adequate.11 Comparatively, a 2017 Kansas study showed similar findings in addition to mentioning barriers to care like directly billing to Medicaid, physical requirements of the job, and financial viability; it was noted that providers that had more years of direct access experience perceived more barriers to providing services.12 In addition, a workforce study of Maine public health DHs showed that half of their independent practice workforce were employed in rural areas.13 Unlike Kansas, Maine public health DHs treat more adults than children, and about 60% reported difficulty finding a dentist to would accept their patient referrals.13
Despite the widespread use of direct access dental hygiene models across the U.S., the body of research about these workforce models is limited. Previous studies commonly assessed career satisfaction, patient populations served, and services provided, referral patterns, and participant attitudes and experiences working in this model. However, several factors merit further exploration, including the source of employment and working relationships with the supervising dentists. The purpose of this study was to build upon the small body of evidence on direct access dental hygiene workforce models by assessing the current PHS DH workforce in Iowa, including the employment environment, practice settings, scope of practice, and motivations for working in this career field.
Methods
A mixed-mode survey was administered in July-September 2019 to all (n=126) PHS DHs in Iowa with active licenses and PHS status. The Iowa Department of Public Health provided the research team with the names and work addresses of the potential participants. An email was sent to all Iowa PHS DHs (n=126) by the Oral Health Consultant of the Iowa Department of Public Health to inform them about the survey. A paper consent letter was mailed to all Iowa-licensed PHS DHs; a personalized link to the online survey was included in the letter. At two and four weeks following the initial fielding, additional reminder mailings were mailed to the non-respondents including a paper copy of the survey. Responses were collected for eight weeks in both modes. A software program (Qualtrics, Provo, UT, USA) was used to administer the electronic survey.
The 40-item instrument was developed using close-ended, open-ended, and 4-point Likert scale questions; the latter used responses from “very satisfied” to “very dissatisfied.” Survey items were either adapted from other sources7,10,11,13,14 or original to this survey. The survey instrument included items regarding employment status and type, scope of practice utilized, compensation methods, relationship with their supervising dentist, motivation for working under public health supervision, and job satisfaction. The survey instrument was pretested by four content experts for clarity and relevance of questions; changes were made based on feedback.
Data were analyzed with SPSS Version 23 (IBM, Armonk, NY, USA) using univariate analyses. The project was approved by the Institutional Review Board of the University of Iowa (#201906752).
Results
Of the potential PHSDH study participants (n=126), 62 completed the survey, yielding a 52% response rate after excluding undeliverables. More participants completed the survey on paper (62.3%), versus online (37.7%). Out of the 62 responses, 42 (68.8%) were actively providing services under public health supervision. The remainder of the results were based on the population of PHDHs actively providing care (n=42).
Among the respondents, 52.4% held an associate degree, and 97.6% (n=40) identified as White. The survey did not ask regarding gender as it has been previously shown that 99% of Iowa dental hygienists are female.15 The highest proportion respondents were age 40-49 years (35.9%). Most (71.6%) had worked clinically as a registered dental hygienist for 10 years or more, while a little more than half (54.7%) had been working under PHS for 5 or fewer years. Sample demographics are shown in Table I.
Demographic and employment characteristics of respondents (n=42).
Employment Patterns
When asked about the number of current jobs, 83.3% of respondents held one job in dental hygiene, and 97.6% held one job under PHS. The most common employer types were local public health agencies (58.5%), community health centers (CHCs) (19.5%), and nonprofit clinics (9.7%). The least common employer types were nursing homes (2.4%) and private dental practices (0%) (Table I).
When asked about their motivation to start working under PHS, 54.8% chose to become a PHS DH on their own (n=23) while 45.2% (n=19) were encouraged to do so by their employer. Of those who were self-motivated to become a PHS DH, the most common motivating factors were an interest in working in public health settings (n=11), the increased job flexibility (n=4), and increased autonomy (n=2). Among self-motivated PHS DHs, 66.7% had a somewhat or very difficult time finding work as a PHS DH the last time they looked for employment in public health. Nearly all the participants (97.6%) were somewhat or very satisfied with their work under PHS (Table I).
Professional Responsibilities
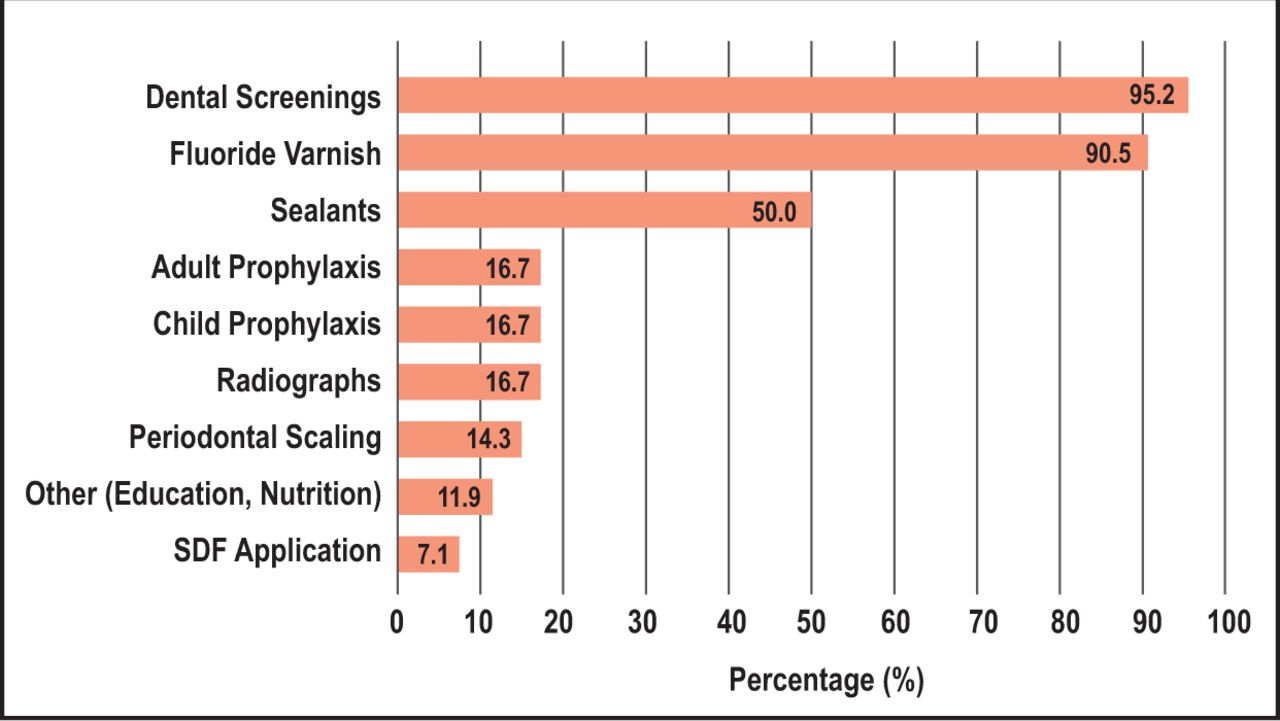
Regarding the types of services provided under PHS, most respondents reported providing dental screenings (95.2%), fluoride varnish (90.5%), and sealants (50.0%). Only 7.1% of respondents reported applying silver diamine fluoride (SDF) under PHS (Figure 1). The average amount of time spent working was 34 hours per week, and nearly half (48.7%, n=20) reported they spent more than three-quarters of their working time providing PHS clinical services.

Types of services provided by PHS respondents* (n=42).
* Multiple response options possible; sums do not equal 100%
Compensation and Billing
Most respondents (73.8%) were paid an hourly wage, and 23.8% were paid via salary; none were paid based on commission. Regarding how public health supervision services are billed, most respondents had services billed by their employer (81.0%) and/or were paid by a program grant (50%) (Table I).
Working Relationships with Supervising Dentist and Referral Patterns
Among public health supervision respondents, a majority (61.0%) of their supervising dentists worked in private practice, followed by 26.8% in CHCs. The amount of communication between the PHS DH and supervising dentist varied, with the highest proportion (38.1%) stating that they communicate several times throughout the year. Most (88.1%) of the respondents found it somewhat or very easy to find a supervising dentist and most (82.9%) were very satisfied with their working relationship with their supervising dentist (Table II).
Supervising dentist and referral factors among respondents (n=42).
Regarding patient referrals, 21.4% of participants reported that their supervising dentist accepted all patient referrals, 50.0% accepted some referrals, while 28.6% did not accept any referrals. Additionally, 71.4% of participants reported it was somewhat or very difficult to find a dentist to accept patient referrals. When making a referral, two thirds (66.7%) of the respondents worked directly with the patient to find a dentist and half (50.0%) provide patients with a list of local dentists to contact (Table II).
Discussion
The purpose of this study was to assess the current PHS DH workforce and describe the self-reported experiences of Iowa’s PHS DHs. Demographic results showed that PHS DH respondents were typically older, with only one respondent under age 30. This may indicate that the more experienced DHs prefer to work in public health or that PHS DH employers have a preference toward more experienced practitioners. This finding may also indicate that there is limited interest or knowledge from new graduates regarding this career option. Findings from the state of Kansas are similar to Iowa in that 74% of their public health DHs are older than 40 years.11
Iowa’s PHS hygienists were most frequently employed by governmental agencies such as local public health agencies and CHCs. Conversely, most supervising dentists work in private practice settings. This could be due to the fact that fewer dentists are employed at local public health agencies, so PHS DHs must seek a supervising dentist elsewhere. Despite being employed by local public health agencies and CHCs, the most common locations where PHS DHs provide services were preschools, elementary schools, and Head Start Programs. The respondents were also employed through federal public health programs such as Women, Infants, and Children (WIC) centers demonstrating that children are receiving more PHS services in Iowa than adults.16 Very few respondents worked in nursing facilities, which could be due to multiple barriers such as patient cooperation and medical complexity, as well as service-related barriers such as increased appointment times for patient visits. These findings were similar to Maine where over 90% of Independent Practice Dental Hygienists provided services in school-based programs and only 3% served nursing homes and long-term care facilities.13 However, Oregon’s Extended Practice Permit Dental Hygienists provide most of their services at residential care facilities followed by primary and secondary schools.17
Regarding the types of services provided by Iowa PHS DHs, the most commonly provided services were screenings, fluoride varnish, and sealants, which is consistent with other states and is in line with the fact that most are providing services in school-based settings.13 Very few Iowa PHS DHs reported applying silver diamine fluoride (SDF). However, it is expected that more PHS DHs are currently utilizing SDF application as this duty was only allowed for PHS use in the year that the survey was fielded.8
There was an almost even split between those who were self-motivated to become a PHS DH and those who were encouraged to do so by their employer. The most important reason for pursuing PHS among those who were self-motivated was a personal interest in public health, which could present opportunities to educate public health-minded dental hygiene students during their education or early in their careers. However, job availability appears to be a limiting factor as 67% of the respondents had a difficult time finding employment as a PHS DH the last time they looked for work. Comparatively, a 2014 study found that 58% of registered DHs in Iowa reported having a somewhat or very difficult time finding work in clinical practice, indicating that the difficulty in finding employment may be broader than the PHS DH workforce.7
When asked about billing and compensation, most PHS respondents had their clinical services billed by their employer because Iowa does not allow DHs to directly bill for services. However, in Maine, where DHs can bill for services rendered, 18% bill themselves and 71% have an employer bill for reimbursement.13 This indicates a potential barrier to PHS DHs as they must rely on a third party to bill for payment; if PHS DHs in Iowa were permitted to directly bill for reimbursement, it could allow for greater flexibility and offer more employment opportunities given that many respondents indicated difficulty finding work.
A majority of supervising dentist respondents accepted at least some patient referrals from their PHS DH. However, PHS DHs also reported difficulty finding dentists to accept patient referrals, suggesting that the quantity of patient referrals may be greater than the number the supervising dentists were willing to accept. In a Maine study, the majority of public health hygienists also expressed challenges finding a dentist to accept patient referrals.13 Low dentist participation in Medicaid is a well-known issue, and may likely be a key factor driving referral difficulty for all public health hygienists. Studies have suggested that dentists may not choose to participate in Medicaid due to the poor or low reimbursement rates.18 In 2016, 40% of Iowa’s dentists reported refusal to participate in any state-offered insurance plans; in addition, many Iowa dentists who do accept Medicaid limit the patients they will see to children or those with a previous patient relationship.19
Regarding the working relationship with their supervising dentist, most respondents found it relatively easy to find a supervising dentist to work with. This is consistent with results from Kansas, Minnesota, and New Mexico where a majority of public health hygienists indicated similar ease in finding a supervising dentist.11,14 In contrast, public health hygienists in Massachusetts reported more difficulty finding a supervising dentist due to issues with malpractice insurance providers.10 There was considerable variation in the frequency of communication between PHS DHs and supervising dentists, with the greatest number communicating less than once a month but more than annually. Conversely, 40% of the ECP holders in Kansas communicate with their supervising dentist daily.11 A majority of PHS respondents had high levels of satisfaction with their job and supervising dentist relationship. These findings were consistent with results from Kansas where 96% reported high satisfaction with their supervising dentist’s support.11
There are several limitations to this study. The target population and response rate to the survey was small, with 42 active PHS DH respondents out of 126 potential participants. There was also a limited amount of diversity within the sample population (98% White). In addition, all survey research is subject to several types of bias; response bias could impact results if survey respondents differed systematically from nonrespondents and recall bias may impact respondents’ ability to remember past events accurately.
Future research should explore in greater detail on the motivations and barriers to DHs working under PHS including how compensation methods and referral acceptance affects their success and satisfaction as well as the employment environment for positions working under PHS. Other research could investigate the ways dental hygiene programs prepare their students to serve in alternative practice settings and possible improvements that could be made to the curriculum. Future studies should also examine the outcomes of direct access dental hygiene workforce models on measures of access to care for underserved populations. One promising study found an association between broader state scope of practice for DHs and improved population oral health;9 however, further research is needed on state-level impacts.
Conclusion
This study of Iowa’s growing workforce of PHS DHs demonstrated that most DHs were employed by government agencies, whereas most supervising dentists worked in private settings. Although most supervising dentists accepted at least some patient referrals, PHS DHS still indicated a high degree of difficulty referring patients for care. Results from this study contributed to knowledge gaps in direct access dental hygiene models, particularly in the areas of employer types and working relationships. Additional research is needed to investigate barriers to care with direct access dental hygiene services in Iowa and other states to ultimately improve access for the underserved.
Footnotes
This manuscript supports the NDHDA priority area, Population level: Access to care (interventions).
Disclosure: This study received funding from the University of Iowa College of Dentistry, Iowa Dental Student Research Award.
- Received October 9, 2020.
- Accepted February 18, 2021.
- Copyright © 2021 The American Dental Hygienists’ Association





{kind=link}