



Abstract
Purpose: Poor ergonomics is one of the leading factors in developing musculoskeletal disorders. The purpose of this study was to evaluate the level of forward neck flexion of dental hygiene students during manual scaling procedures while wearing magnification loupes and investigate the prevalence of musculoskeletal neck pain.
Methods: A convenience sample of second year dental hygiene students was recruited for this observational study (n=24). A goniometer application was used to measure levels of neck flexion, while wearing dental loupes, 30 minutes into a manual scaling procedure. Participants completed a McGill Pain Questionnaire with a body diagram and an additional survey at the end of the session. Descriptive statistics were used to analyze the data.
Results: All participants’ showed neck flexion exceeding 20° at the conclusion of a 30-minute manual scaling procedure. A majority (67%) were in a compromised range and 33% were in a harmful range. The top five pain descriptors identified in the pain questionnaire were aching, tiring-exhausted, throbbing, tender, and heavy. Pain was identified in the shoulder/trapezius (63%), cervical (50%), scapular (36%); and the participants’ reported pain ranging from 1 to 7.
Conclusion: Fifty percent of the participants experienced cervical neck pain when exceeding a forward neck flexion of more than 20° during a manual scaling procedure. The shoulder/trapezius and cervical regions were most frequently identified as the location of pain or problems. An early prevalence of musculoskeletal pain in was observed in this sample population of dental hygiene students.
- dental hygiene students
- musculoskeletal disorders
- ergonomics
- neck flexion
- clinical education
- magnification loupes
Introduction
Musculoskeletal disorders (MSDs) are important occupational health issues in health care workers;1 and poor ergonomics has been identified as one of the leading factors in developing a MSD.2 Musculoskeletal disorders are identified as injuries to the human body support system such as the ligaments, tendons, muscles, nerves, blood vessels, bones, and joints.1,3 The goal of ergonomics is to develop a safe and comfortable working environment preventing health problems and improving productivity.4,5 Many research studies have documented increased occupational risks for dental hygienists, and dental professionals in general, to develop MSDs.1,2,3 A high prevalence rate of work related musculoskeletal disorders in dental professionals has been reported, ranging from 64%-93%.3 Poor ergonomics such as excessive neck flexion, constrained working postures, excessive static and peak loading of the upper trapezius and the forearm extensor muscles all play a role in developing a work-related MSD.2 The physical demands for the upper extremities, in addition to limited working fields, unique movements, fine and repetitive tasks, and static postures in dental hygiene practice create an increased risk for dental hygienists to develop work-related MSDs in the neck and shoulders.2,6,7 Increased prevalence of work-related MSDs over time has been considered a leading factor in early retirement and career changes among dental professionals.2,3,8
Symptoms of work-related MSDs involve swelling, tenderness, numbness, tingling, and loss of strength and pain is reported in the back, neck, hand, wrist, shoulders, as well as lower extremities such as hips, thighs, and knees.1,6,9 Musculoskeletal discomfort can be described as slight and recurrent ranging to severe and incapacitating.9 Severe pain is often a result of cumulative trauma to effected areas.1,3 In a twelve-month study measuring the physical work load among dental hygienists (n=51), a majority (82%, n=42) reported pain in the neck region with one-third of those with neck pain diagnosed with tension neck syndrome.10
Tension neck syndrome is a separate diagnosis rising from risk factors of work-related MSDs such as sustained exertion, static and awkward postures, and excessive neck bending. Tension neck syndrome involves painful neck spasms and trigger points that come from a specific type of work loading common in dental hygiene.11 Work loading can be explained as the amount of stress put on the muscles during a specific task.12 Symptoms also include stiffness and limited movement around the neck, pain radiating to the arms and shoulder blades, and a palpable hardness in the neck region.13 In a study of the biomechanical demands of manual scaling on the shoulders and neck of dental hygienists, researchers found the neck and shoulders had excessive demands during 30 minutes of manual scaling from the 8 o’clock position.2 The participants spent at least 90% of their scaling time over the recommended limits of neck flexion.2 Studies continually identify the neck region to be heavily affected by pain among dental professionals.
Magnification loupes have been identified in the literature as a protective factor against MSDs.3,14 Dental loupes are beneficial to the clinician in magnifying the work area and reducing muscle strain when fitted correctly, however poorly fitted loupes can contribute to ergonomic strain.14 Working distance, declination angle, and frame size must be considered for correct fit. An optimal working distance should be 14-20 inches but may vary depending on the operator’s size.13,15 The declination angle should be steep enough to allow clarity into the working field without excessive neck flexion. Frame size impacts the position of the microscope lenses and declination angle with larger frames resulting in more optimal declination.15
While work-related-MSDs have been studied extensively in practicing clinicians, including dental hygienists, fewer studies have been conducted among dental hygiene students.1 Despite the limited number of studies among dental hygiene students, existing research has demonstrated that over a three-year period, dental hygiene students demonstrated increased neck pain specifically.6
Healthy neck flexion has been identified in previous research to be less than or equal to 20 degrees.15,16,17,18 Dental hygiene students need to understand the importance of healthy degrees of neck flexion to prevent neck pain, increase productivity and future career longevity. The purpose of this study was to evaluate the level of forward neck flexion of dental hygiene students during manual scaling procedures while wearing magnification loupes and investigate the prevalence of musculoskeletal neck pain.
Methods
Sample
This observational study was approved by the University of New Mexico’s Institutional Review Board (ID 18-785). A convenience sample of second-year students from the dental hygiene program at the University of New Mexico were invited to participate in the study (n=24). Participants needed to be over the age of 18, and in the final semester of their second year to be eligible for inclusion in the study population. Informed consent was obtained from all participants.
Instruments
A goniometer iPhone 8plus application (G-pro; 5fuf5, Nobby Beach, AU) was used to measure levels of neck flexion. The goniometer application uses a built-in accelerometer sensor and digital display to measure angles. All measurements taken were performed on the right side of the face once the correct phone axis was established. The criteria for the evaluation assessment of neck flexion were based on Branson et al. Posture Assessment Instrument (PAI).18 Categories included a healthy range < 20°, a compromised range between >20° and < 45°, and a harmful range of >45° of neck flexion.18
A Short Form McGill Pain questionnaire and an additional two question survey was administered at conclusion of the measurement session. The pain questionnaire19 included a full body pain diagram to indicate the location of pain or problems and columns to indicate the level of pain (mild, moderate or severe) for fifteen pain associated words. Pain was also rated on a linear scale with a range of no pain to the worst possible pain. Pain scales were also ranked from 0-10 in consistent intervals with the pain inventory of no pain to the worst possible pain on the completed questionnaires.
The two-item, yes/no survey asked: “Do you wear dental loupes when performing manual scaling during patient care?” and “Have you had an injury to your head, shoulders, or neck regions prior to dental hygiene school?”
Procedure
A data collection calibration trial on consenting occupational therapy (OT) student volunteers was conducted to test the principal investigator’s (PI) reliability using the goniometer application to measure neck flexion. An OT faculty member supervised the PI during the trial sessions. Measurements with a standard goniometer were used to assess agreement. An agreement of plus or minus 5° for goniometry measurements has been deemed acceptable in previous research.20 A total of 50 trials were conducted on OT student volunteers over two days and a 90% (9/10) agreement was found with the two types of measurements by the end of the second day.
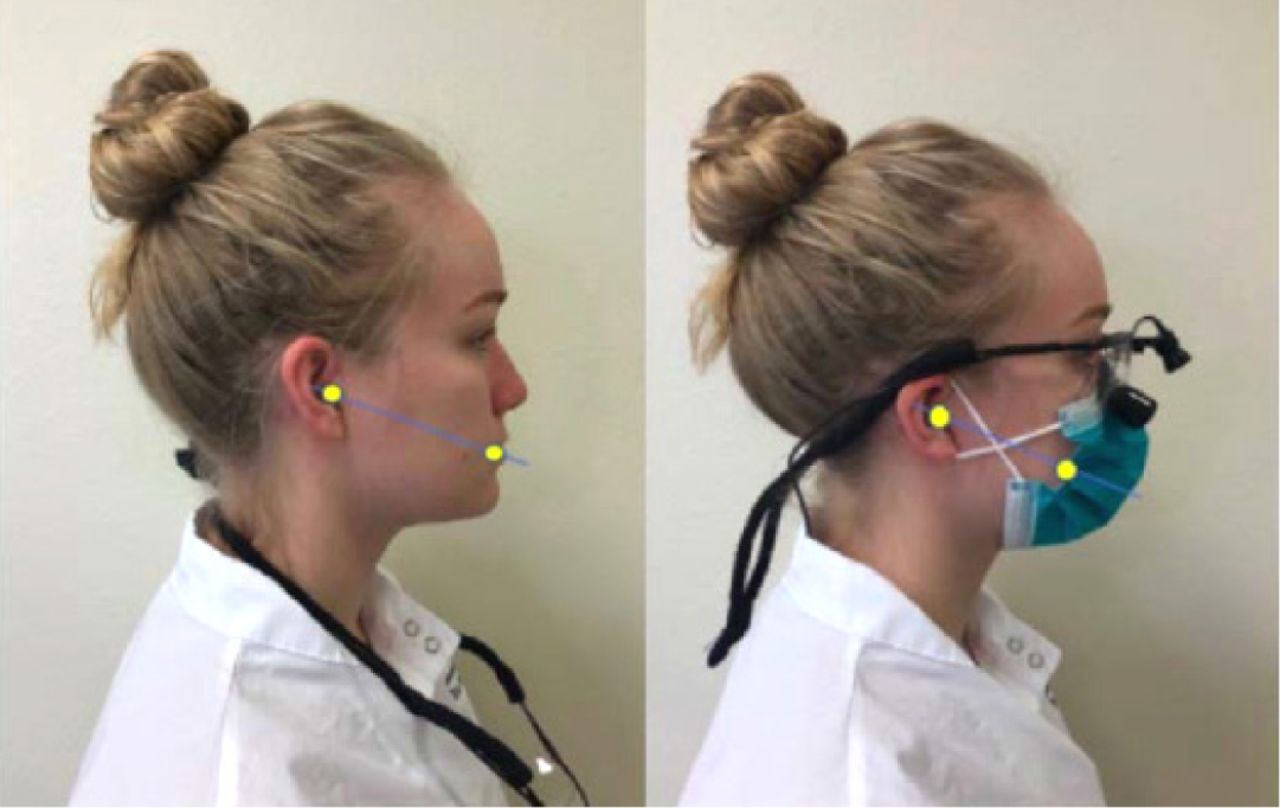
Data collection sessions were scheduled over a period of five weeks and took place in one of the dental hygiene clinical operatories. Participants wore their own magnification loupes and performed a manual scaling procedures for 30 minutes. At the conclusion of the 30 minutes of scaling, the level of neck flexion was measured by tapping the iPhone screen while using the gonimeter application. The iPhone was placed at the external auditory meatus, test position parallel or 0°. The axis was adjusted to the test position and aligned with the commissure of the lip to gather the measurement (Figure 1). At the conclusion of session participants were given a hard copy of a short form McGill Pain Questionnaire18 and the two-item survey.

Neck flexion measurement points without and with magnification loupes and a mask.
Data analysis
Data for neck flexion were grouped into one of the categories from the Branson et al. PAI tool18 and were analyzed through descriptive statistics. Associations between the level of neck flexion and pain measures were analyzed using the Pearson and Spearman correlation coefficient methods to measure the strength of the association between two continuous variables: neck flexion and neck pain.
Results
Twenty-four second-year dental hygiene students consented to participate in the study. The female (n=22) and male (n=2) participants ranged in age from 21 to 47 years of age with a mean age of 27 years. All participants (n=24) demonstrated greater than 20° of neck flexion at the conclusion of the manual scaling session. The minimum degree of neck flexion measured was 30°, maximum was 63°, and the mean degrees of neck flexion was 42.5°. Using the categories established by the Branson et al. PAI, none of the participants were in the healthy range (<20°), two-thirds (67%, n=16) were in the compromised range (>20° and <45°), and one-third (33%, n=8) were in the harmful range (>45°).
Results from the McGill Pain Questionnaire were analyzed and showed the highest rated pain number was a 7 (8%, n=2) by participants while the most frequently indicated pain number was a 2 (29%, n=7). The Spearman correlation with pain score was (r) 0.29 (p=0.17) and the Pearson correlation with pain score was (r) 0.30 (p=0.14). The results showed no statistically significant association between neck flexion and neck pain (p<0.05).
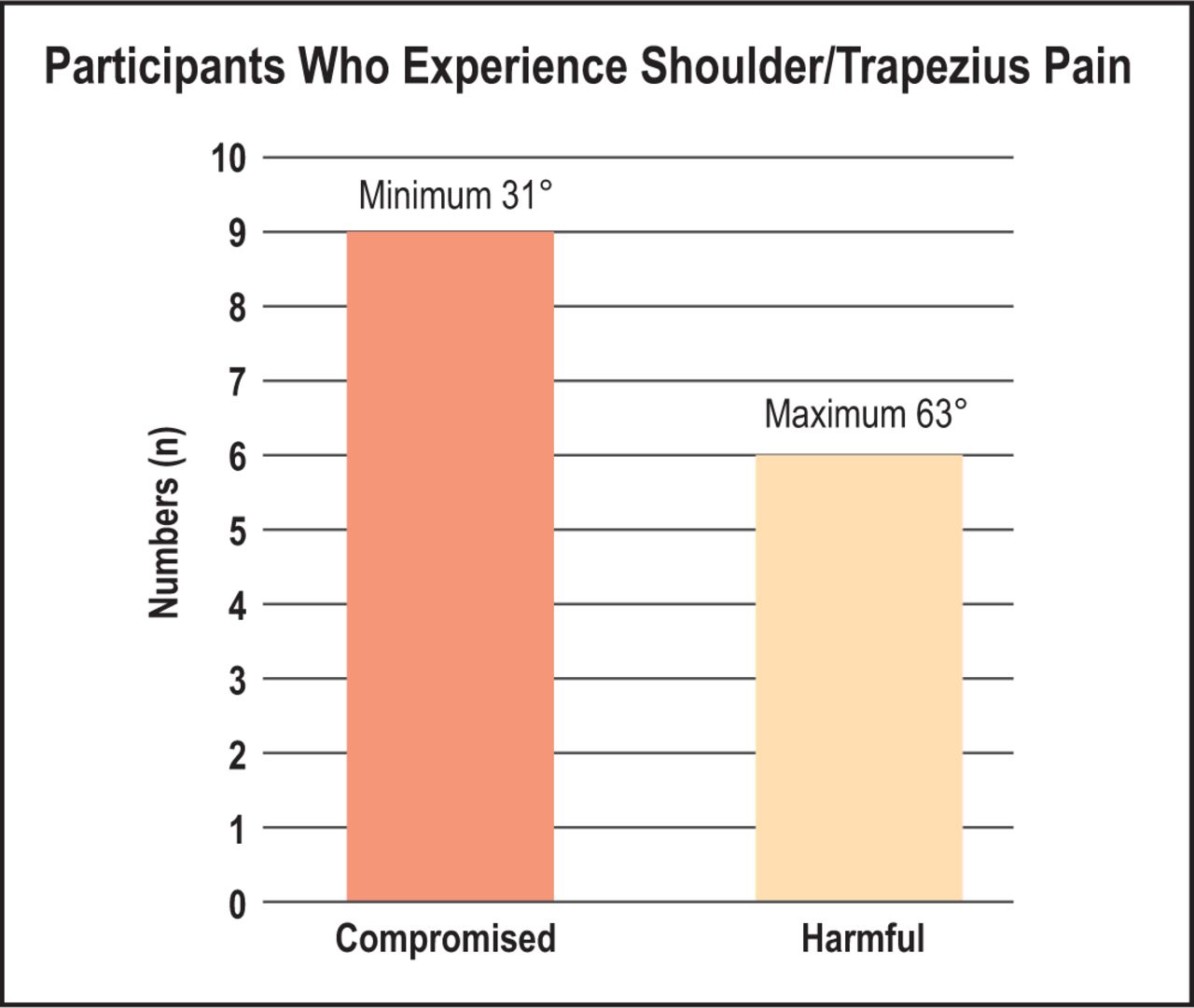
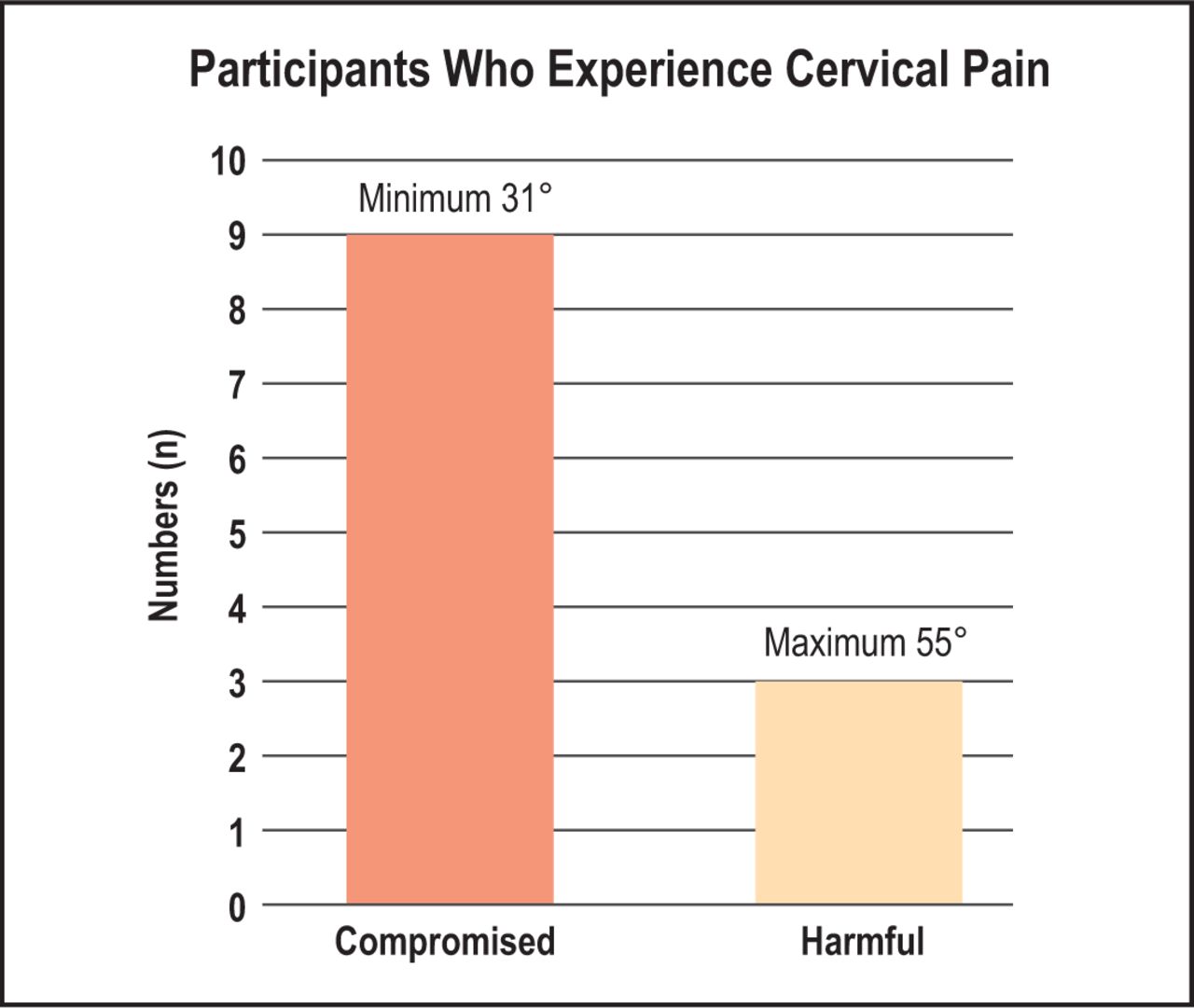
Further data from the McGill Pain Questionnaire includes the top five pain associated words selected as aching (71%, n=17), tiring-exhausted (58%, n=14), throbbing (33%, n=8), tender (25%, n=6), and heavy (21%, n=5). The top five pain or problem areas selected were the shoulder/trapezius (63%, n=15), cervical (50%, n=12), low back (46%, n=11), (36%, n=9) scapular, and (21%, n=5) mid back. Shoulder/trapezius pain was evaluated with a mean degrees of neck flexion at 43°, with a minimum of 31° and maximum of 63°, as shown in Figure 2 The cervical region was also evaluated and matched with a mean degrees of neck flexion at 43°, with a minimum at 31° and maximum of 55°, as shown in Figure 3.
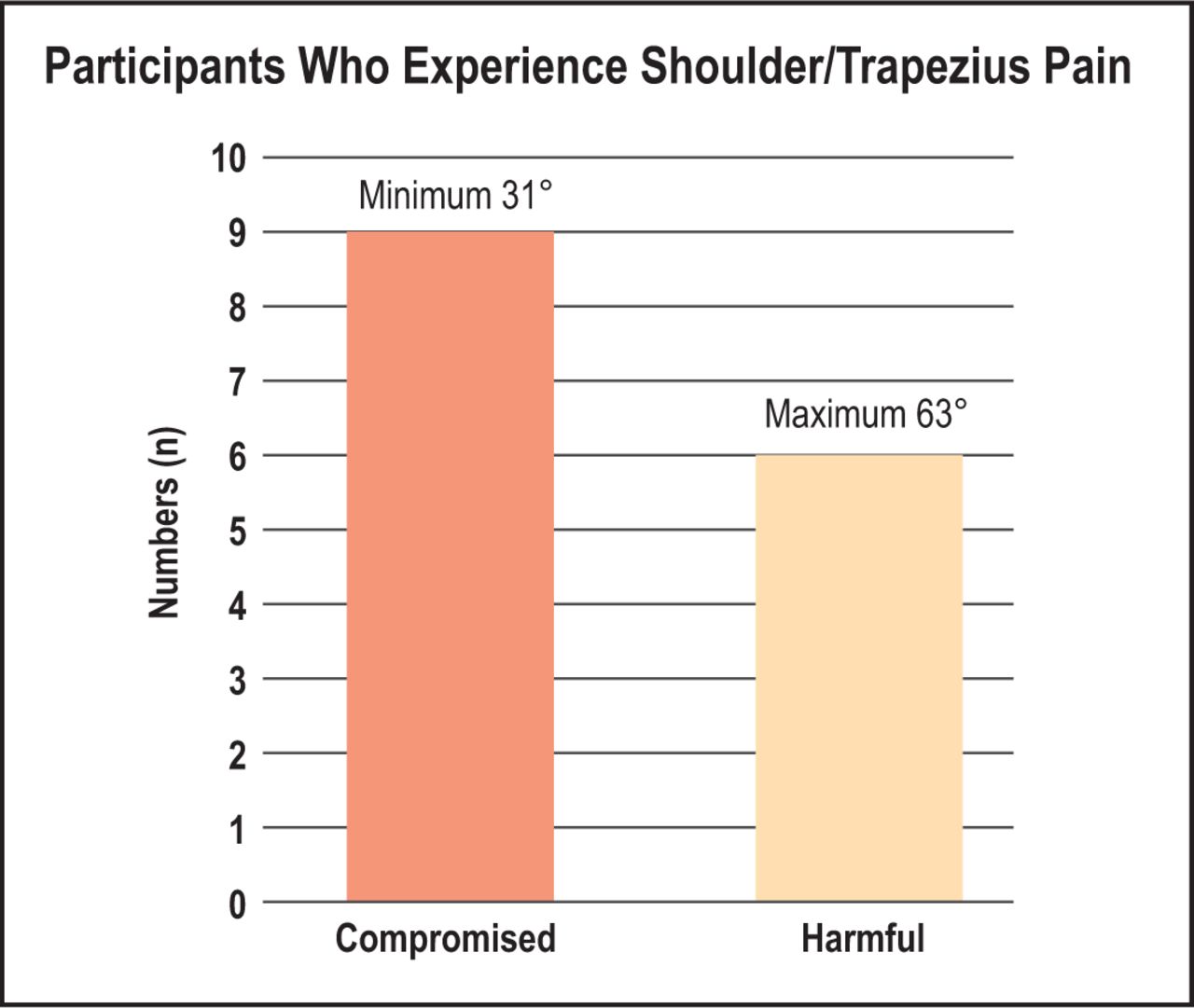
Degree of neck flexion in participants reporting shoulder/trapezius pain.
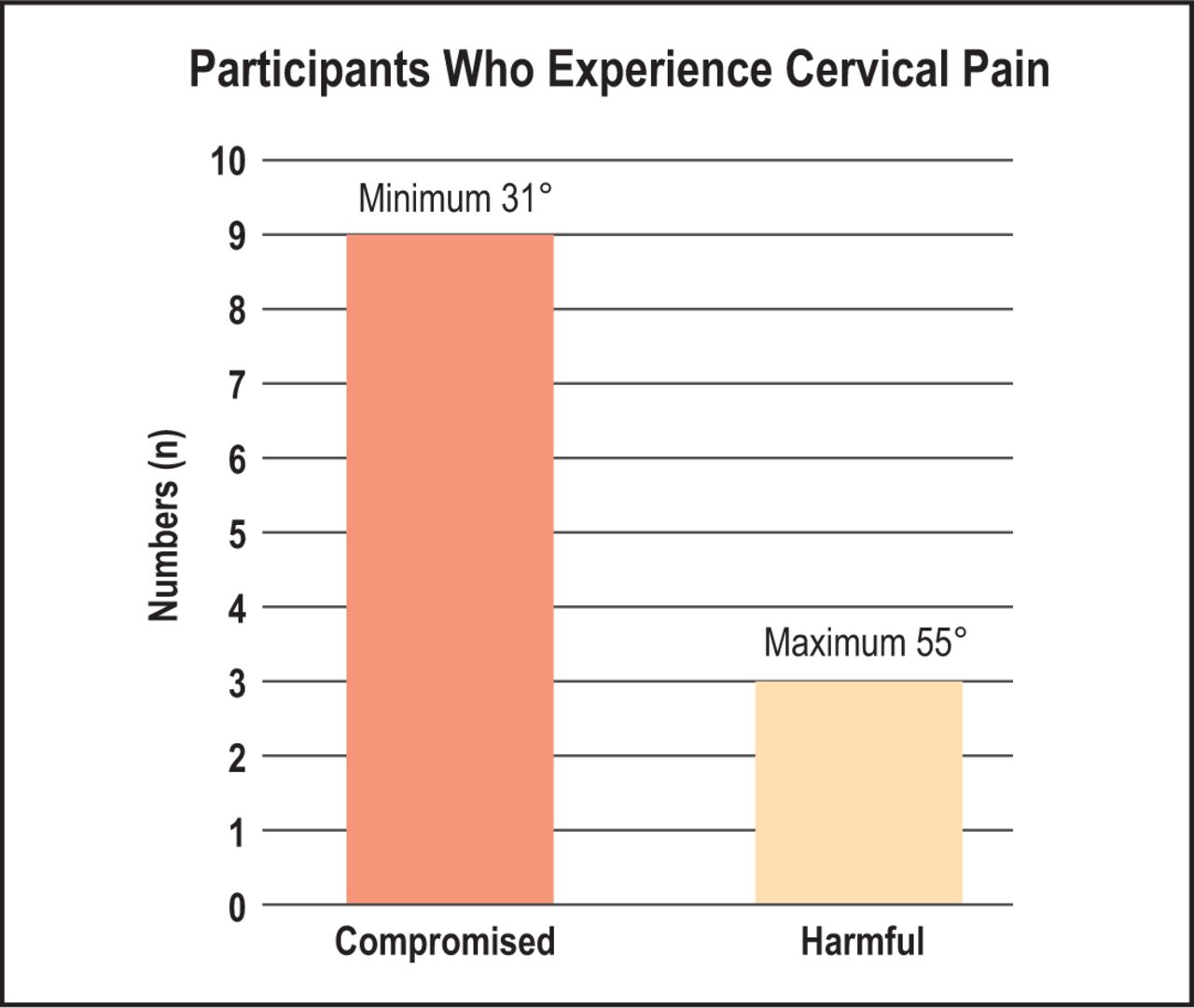
Degree of neck flexion in participants reporting cervical pain
Participants answered two additional questions regarding the use of magnification loupes and any previous injuries to the head, shoulders or neck. All participants reported using magnification loupes while providing patient care and 8% (n=2) reported a history of a previous injury.
Discussion
Dental hygiene students are affected by the same work-related MSD risk factors as practicing clinicians, with the neck, shoulders and lower back at high risk for pain.5 Research has shown that the appropriate degrees of forward neck flexion for dental professionals should be < 20°.15-18 This study investigated the prevalence of neck pain in second year dental hygiene students to determine whether this pain was associated with the levels of forward neck flexion during manual scaling procedures.
Findings from this study suggest that students may start to develop pain in the neck region, along with other areas, associated with excessive neck flexion during their dental hygiene education and support previous research reported in the literature. In a longitudinal study of MSDs in practicing dental hygienists and dental hygiene students, Warren et al. found that pain intensity in the neck and shoulders was primarily associated with bending of the neck and twisting.21 Morse et al. studied neck and shoulder pain in dental hygienists and students and found that the majority of the participants often worked with a bent neck and that over one-third (37%) of the dental hygiene student participants self-reported neck symptoms including throbbing, pain, aching, stiffness, burning, tingling, or numbness on a regular basis.11 La Delfa et al. observed the demands of manual scaling on the shoulders and neck of practicing dental hygienists and found that the neck and shoulders were in extreme demand during a 30-minute manual scaling simulation and more notably the neck was in excessive flexion.2
All of the participants in this study wore dental loupes, an intervention to help decrease neck flexion, in addition to magnification of the work area.14 As suggested by Garcia et al., dental hygiene students should implement dental loupes beginning with pre-clinical work to help with posture and vision clarity.5 While all participants wore loupes in this study, musculoskeletal pain was still present.
One factor that could affect the amount of neck flexion and posture is inadequately fitted loupes. Dental loupes have three variables to assess when being fitted and it is possible that the working distance was measured too close, the declination angle not steep enough, or the frame size was too small. When all of these variables are measured correctly, the operator should be able to flex their neck at 20° or less.16 These variables should be performed correctly by the loupe fitters, however monitoring the fitting process can be difficult and the wearer may not be able to interpret proper fit.
This study had limitations. The sample size was small and limited to one institution. The small sample did not generate enough data to create a significant association between neck flexion and pain. While all the students wore magnification loupes, the fit of the loupes was not tested. Flexion was only measured from one position and may vary depending the area of instrumentation. Since the participants knew that they were being observed there may have been the Hawthorne effect on their positioning. Future investigation with a larger sample size and longer study period would increase generalizability. In addition, future studies would want to investigate more variables including the calibration of adequately fitted magnification loupes to better determine factors affecting the prevalence of work-related MSDs.
Conclusion
Dental hygiene students in this sample failed to maintain optimal neck flexion of less than 20° during a point in time instrumentation procedure while wearing magnification loupes. Fifty percent of the participants experienced cervical neck pain when exceeding a forward neck flexion of 20°. Shoulder/trapezius and cervical regions were most frequently identified as the location of pain or problems. An early prevalence of musculoskeletal pain was observed in this sample population of dental hygiene students. Dental hygiene students should be objectively examined for signs and symptoms of MSDs during clinical education.
Footnotes
This manuscript supports the NDHRA research agenda Professional development: Occupational health (Determination and assessment of risks).
- Received March 1, 2020.
- Accepted September 11, 2020.
- Copyright © 2021 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}