



Abstract
Purpose: Fibromyalgia syndrome (FMS) is a neurosensory disorder characterized by widespread musculoskeletal pain. Typically persistent fatigue, depression, limb stiffness, non-refreshing sleep and cognitive deficiencies are also experienced. Oral symptoms and pain are common, requiring adaptations in patient management strategies and treatment interventions. Appropriate dental hygiene care of patients suffering with this disorder is contingent upon an understanding of disease epidemiology, pathophysiology, clinical characteristics, oral signs and symptoms, as well as treatment approaches. With this information dental hygienists will be better prepared to provide appropriate and effective treatment to patients with FMS.
Introduction
Fibromyalgia syndrome (FMS) is a neurosensory disorder of unknown etiology characterized by chronic musculoskeletal pain, fatigue, tenderness and sleep disturbances. FMS can result in severe disability and loss of function, leading to decreased quality of life.1 This disorder can affect any aspect of an individual's body, including the oral cavity, and adverse orofacial conditions are common. Modifications in dental hygiene treatment are often needed to ensure patient comfort and optimum treatment. In addition, oral care practitioners may identify early symptoms of FMS, assisting the patient in receiving a proper diagnosis. Appropriate dental hygiene management requires an understanding of disease characteristics and pathophysiology, oral health considerations and treatment interventions.
Epidemiology
FMS is the second most common diagnosis made by rheumatologists and is estimated to affect 3 to 6% of the population worldwide.2,3 FMS can affect anyone regardless of age, gender or ethnicity; however 75 to 90% of people diagnosed are women.3 Prevalence of fibromyalgia is higher at middle age (30 to 50 years) or over the age of 50.4-13 The worldwide incidence of FMS is 6.88 per 1,000 males and 11.28 per 1,000 females.14 The incidence may be increasing and is linked to increased disease awareness among physicians.
Basic Characteristics
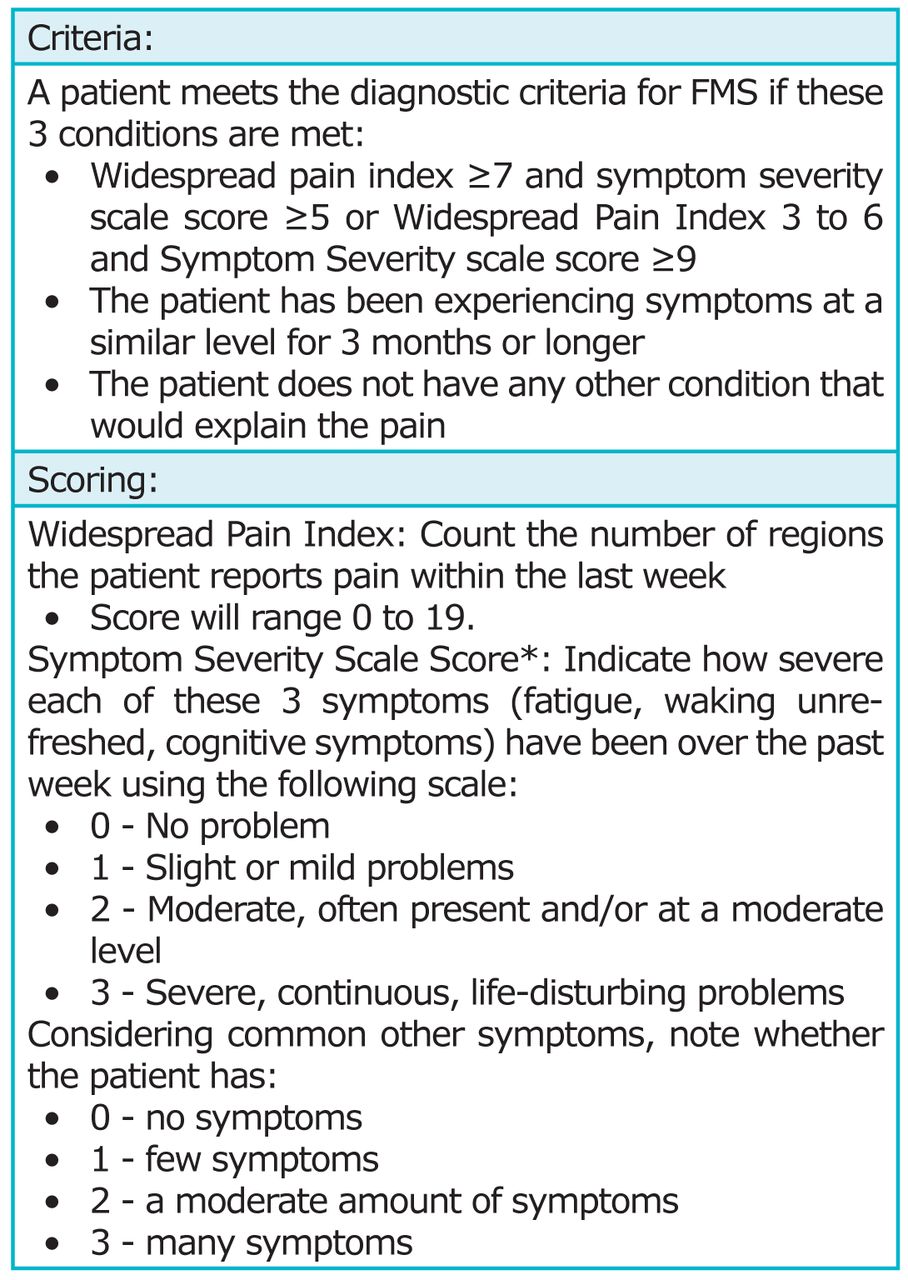
The 1990 American College of Rheumatology classification criteria for FMS included a history of chronic, diffuse pain affecting 4 quadrants of the body for at least 3 months and pain upon palpation in at least 11 out of 18 tender points.15 In 2010, the American College of Rheumatology revised this criterion, eliminating the need to assess tender points. Instead, the criteria requires a detailed interview to evaluate total body pain using a Widespread Pain Index, as well as a measurement of symptom severity, known as the Symptom Severity scale.16 To be diagnosed with FMS the criteria found in Figure 1 must be met.
The most predominant symptom of FMS is chronic, widespread musculoskeletal pain, described as being persistent, deep, aching and/or throbbing. Hyperalgesia (exaggerated or prolonged response to stimuli), dysesthesia (unpleasant, abnormal sense of touch) and allodynia (perception of pain to a non-painful stimulus) are also common findings.17,18 Some people experience uniform pain all day long, while others report pain that is worse in the morning, improves during the day and worsens again at night. Pain associated with FMS can be exacerbated by physical or emotional stress, non-restorative sleep, strenuous activity and changes in weather.18,19
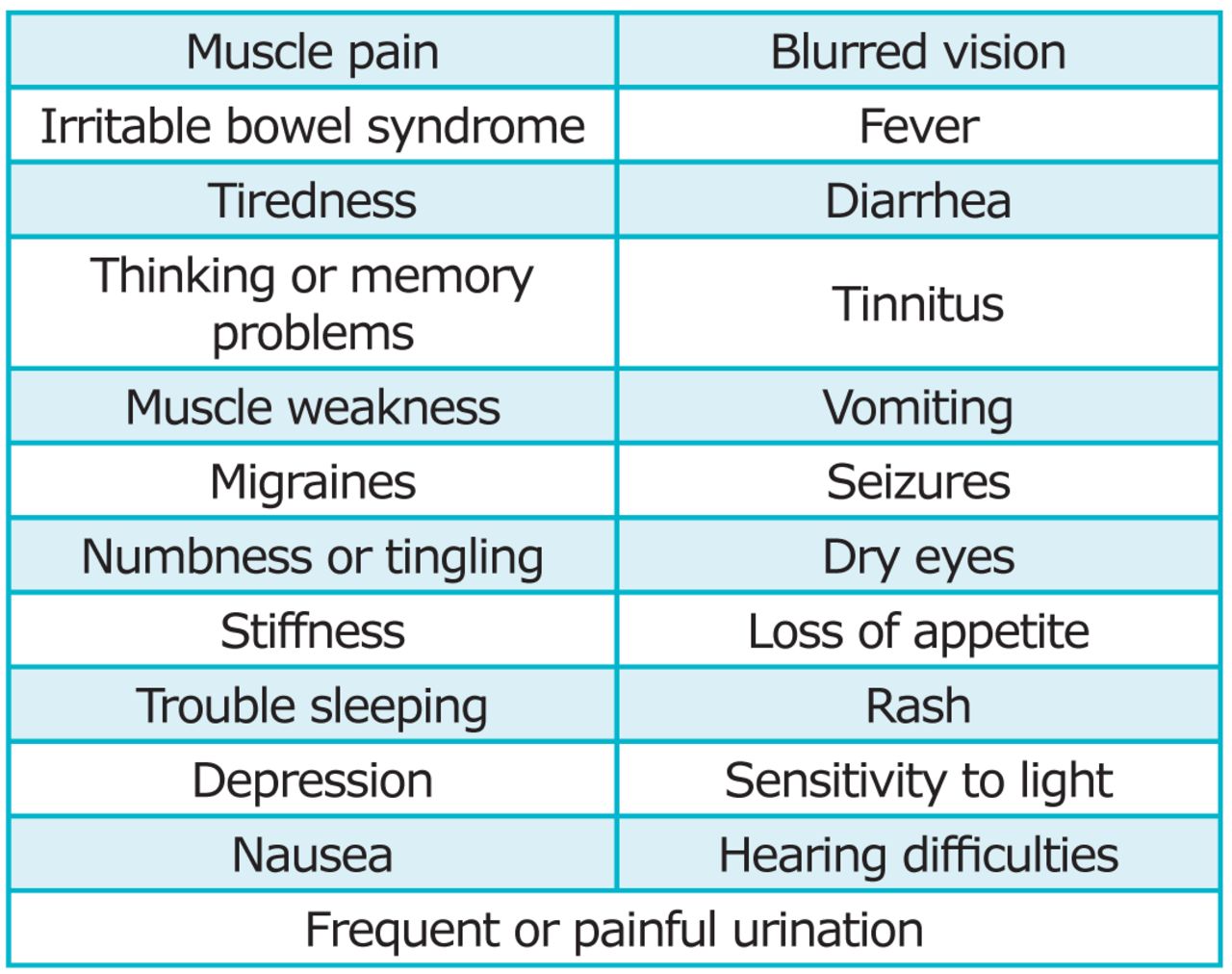
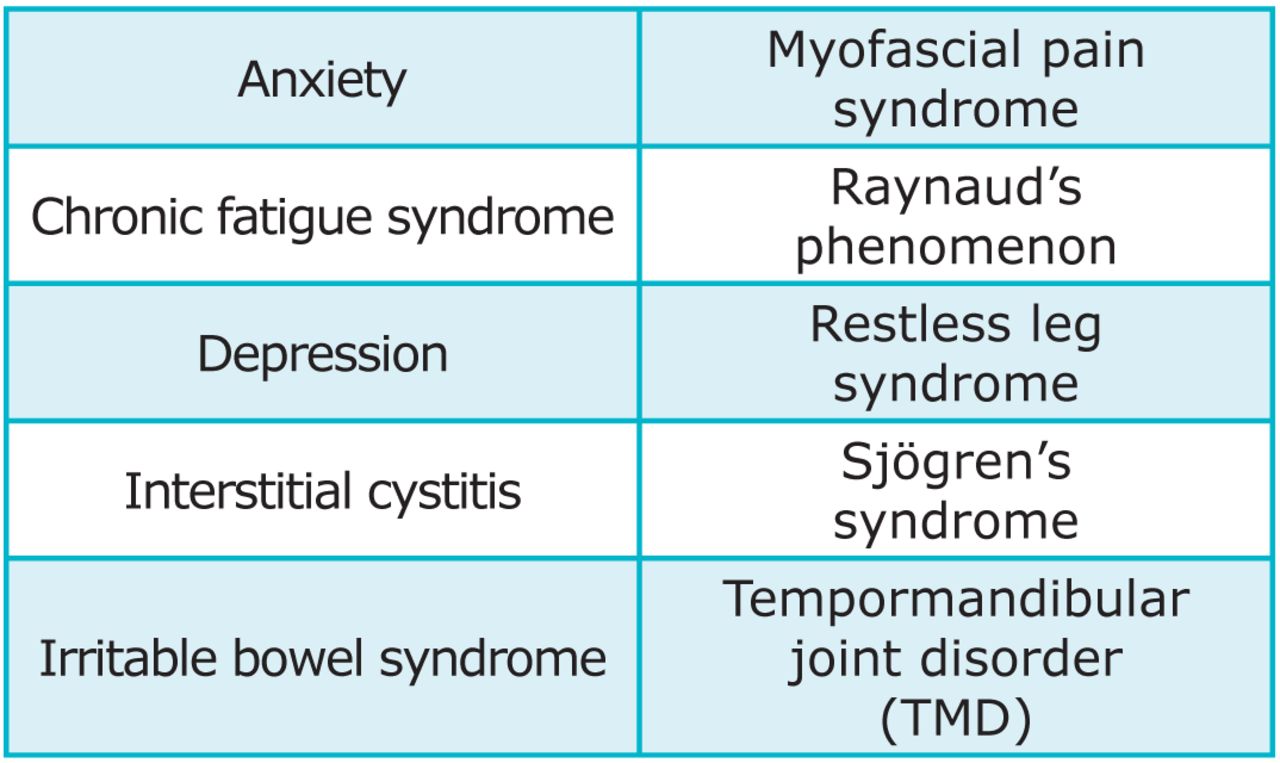
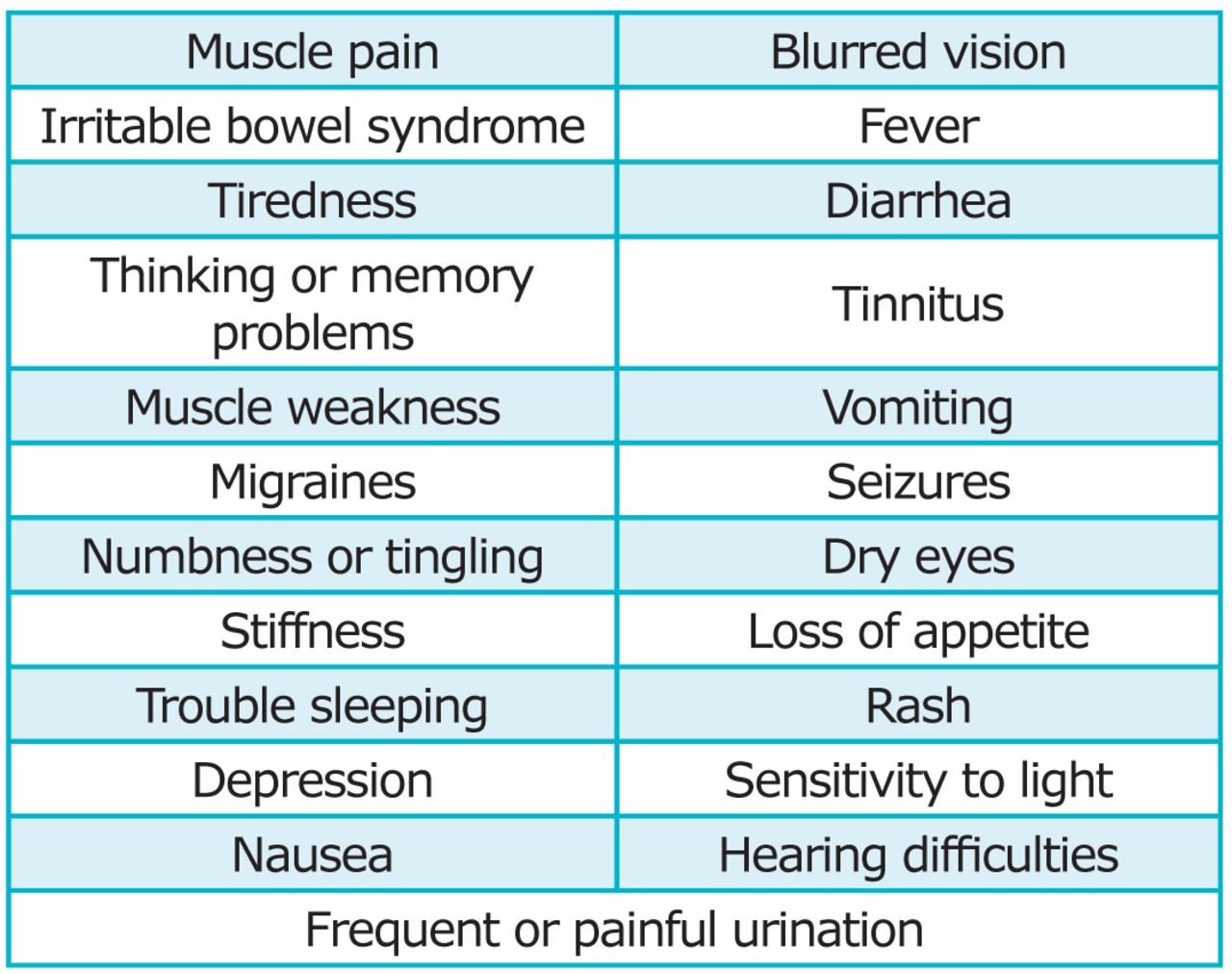
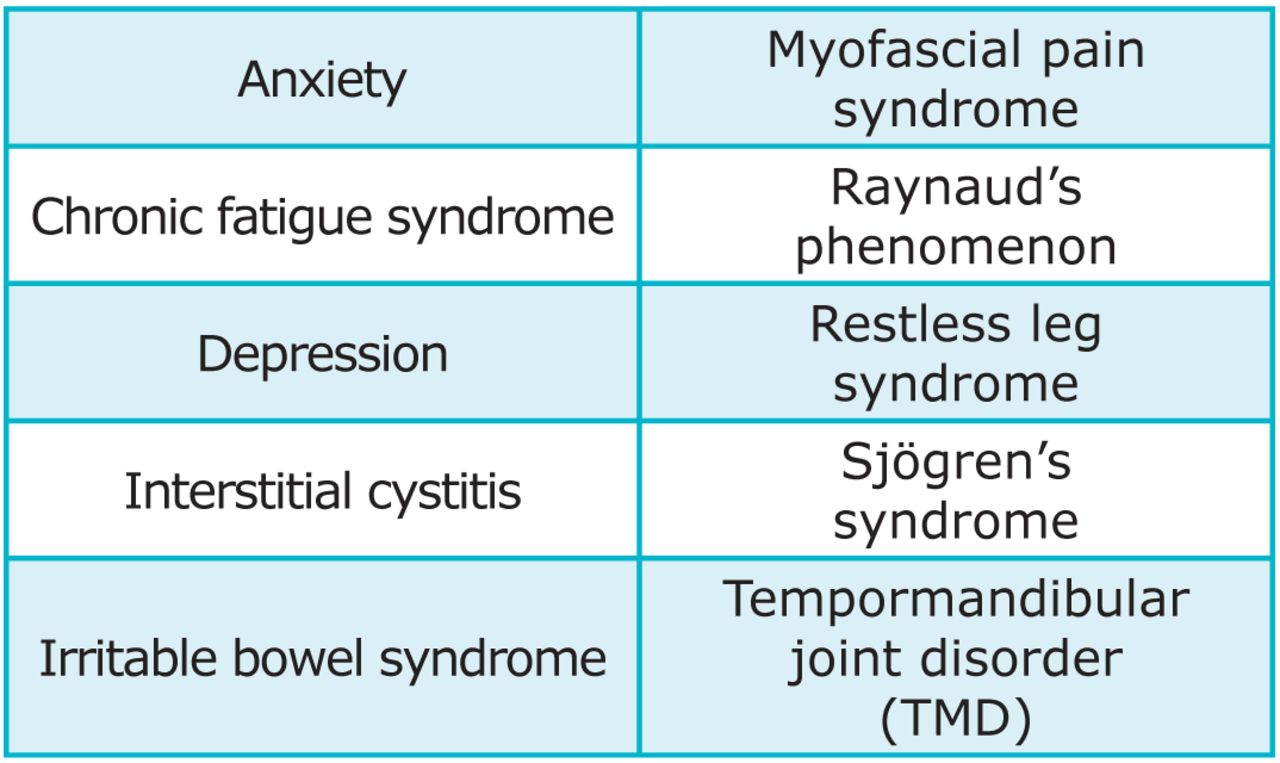
Fatigue, cognitive deficiency, tenderness upon mild palpation and non-restorative sleep are common manifestations often accompanied by a wide array of additional symptoms listed in Figure 2.20,21 The onset of symptoms can appear suddenly; however, they are generally experienced gradually.20,22 Common psychiatric and medical comorbidities may also be present (Figure 3).18,21
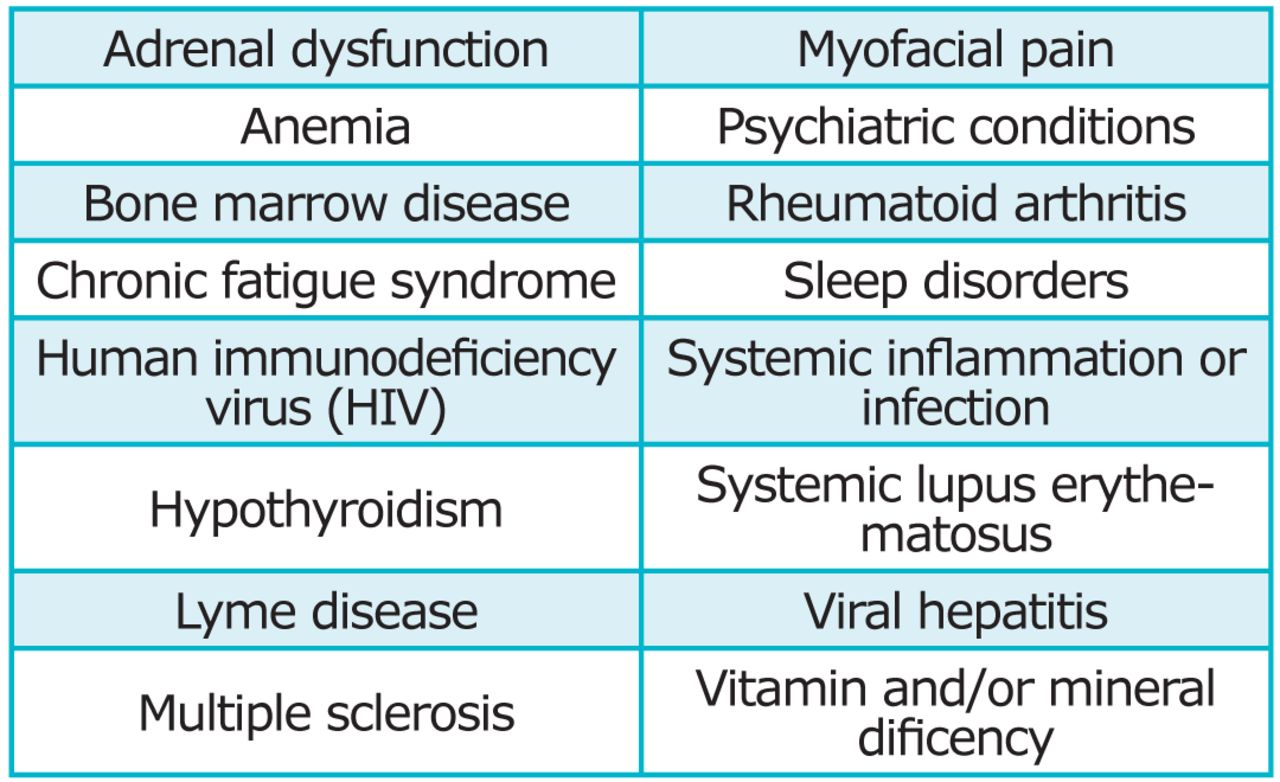
Diseases of fatigue and widespread pain have similar signs and symptoms making the diagnosis of FMS difficult. Lyme disease, hypothyroidism, rheumatoid arthritis, systemic lupus and undiagnosed cancer are often confused with FMS (Figure 4).18,22 Because there are no objective laboratory or radiographic tests to definitively diagnose FMS, patients often report a long delay between onset of symptoms and a diagnosis.1
Sleep disturbances reported include non-restorative sleep, insomnia and poor quality of sleep.23 Munguia-Izquierdo and Legaz-Arrese revealed the prevalence of poor sleep quality was 96% in patients with FMS compared to 46% for healthy subjects.24 Quality of sleep was much lower in patients with FMS compared to controls and poor sleep quality was strongly associated with pain and fatigue.24
FMS can result in severe disability and loss of function, making daily tasks, including oral self-care, difficult or unmanageable.1,19,25 Research by Bennett et al suggests people with FMS have difficulty with routine activities such as walking 2 blocks (55%), climbing stairs (62%), shopping (66%), household chores (68%) and carrying 10 pounds (70%).19 The debilitating effects of FMS can also be seen in the work place. Decreased ability to function leads to loss in productivity, increased work absenteeism and an overall decreased quality of life.26 In fact, working adults with FMS miss an average of almost 17 days of work annually compared to 6 days for those without the syndrome.27 Fatigue, inability to concentrate, decreased motivation, and low self-efficacy may contribute to poor job performance.
Depression, anxiety, stress and impaired cognitive function are common psychological findings in patients with FMS. Bennett el al found 38% of FMS patients reported anxiety and 40% reported depression.19 These psychological disturbances may be related to coping with the debilitating effects and chronic pain of FMS, rather than a primary symptom.28 Cognitive deficiency in people with FMS is sometimes called “fibro fog” and includes short-term memory loss, reduced mental alertness and decreased ability to multitask.18,21
Pathophysiology
FMS is linked to a multifactorial etiology.22 Suspected causes of FMS include abnormalities in pain pathways, as well as genetic and environmental factors.21-23 Cerebrospinal fluid substance P is a neurotransmitter released when axons are stimulated. Consistently elevated in people with FMS, this causes increased sensitivity and enhanced awareness of pain.23,29 Substance P helps regulate the responsiveness of N-methyl-D-aspartate receptors to the neurotransmitter glutamide, which plays a role in central sensitization and temporal summation.20,21 Concentration of substance P in cerebrospinal fluid is 2 to 3 times higher in people with FMS compared to control subjects.23,29 Substance P is involved in transmission of pain information from the periphery to the central nervous system (CNS). Research suggests the combined effect of low serotonin levels and high substance P concentration, contribute to more pain than either abnormality on their own, and this dual dysfunction may be responsible for the onset of FMS.21,30

2010 Fibromyalgia Syndrome Diagnostic Criteria16
*The Symptom Severity scale score is the sum of the severity of the 3 symptoms (fatigue, waking unrefreshed, cognitive symptoms) and the extent of the other symptoms in general. Score will be between 0 and 12.
Symptoms of Fibromyalgia Syndrome16
The CNS is the predominant source of pain in FMS. CNS sensitization, increased excitability of neurons found in the spinal cord, makes neurons more sensitive to stimuli. Central sensitization is characterized by an exaggerated pain response, prolonged duration of pain, increased pain intensity and wider pain distribution.21 A related phenomenon to sensitization is temporal summation, called “wind-up,” which occurs when a stimuli is applied repeatedly. With each repeated stimulation there is a progressive increase in pain leading to prolonged stimulation of C nerve fibers.21 Research suggests levels of temporal summation from repetitive stimulation in people with FMS consistently exceed those of control subjects over a range of stimulus frequencies.31,32 These phenomenon most likely result in people with FMS exhibiting a lower threshold of pain in response to stimuli.
A neuroendocrine system dysfunction involving the abnormal functioning of the hypothalamic pituitary adrenal axis is linked to sleep disturbances in patients with FMS.21,22 In response to stress, the body secretes cortisol, and during chronic stress the body continually increases secretion of this chemical. In an effort to counteract the elevated amount of cortisol, the negative feedback loop is amplified which eventually leads to overcompensation and cortisol deficiency.22 This cortisol deficiency is most likely culpable in causing non-restorative sleep for FMS patients.22

Research has also linked abnormal levels of the neurotransmitters serotonin, norepinephrine and dopamine with FMS.2,20,22,23,30,33 Low serotonin levels are the most widely acknowledged biochemical irregularity found in people with FMS and are of particular interest due to their affect on delta sleep and pain modulation.18,22,23,33-35 Serotonin and norepinephrine play a role in stopping pain response by hindering pain pathways. When individuals with FMS have decreased levels of these neurotransmitters their pain is prolonged.20,22 Dopamine plays a critical role in modulating pain perception in the CNS by inhibiting pain pathways and inducing natural analgesia during acute stress. During chronic stress the body tries to restore homeostasis and dopamine eventually becomes decreased due to overcompensation of the negative feedback loop, leading to a hyperalgesic state.
Both genetic and environmental factors may be involved in the development of FMS. Research suggests the high occurrence of FMS in families may be attributed to genetic factors.36-38 Women who have a relative with FMS are more likely to have the syndrome; however, it is unclear whether this is due to genetics, shared environmental factors or both.39
Environmental triggers such as mechanical or physical trauma and psychosocial factors have been correlated with the development of FMS.33 A study by Bennett et al suggests chronic stress is the most perceived triggering event of FMS onset (41%) followed by emotional trauma (31.3%).19 Trauma and stress may alter the pain modulatory response in the brain, which could contribute to the enhanced pain perception. Acute illness, serious infection, physical injury, surgery, motor vehicle accidents and other pain conditions are also commonly reported physical stressors.19,33 Psychosocial factors, such as a catastrophic event or abuse (emotional, physical or sexual) have also been associated with onset of symptoms.19,33 However, research on the relationship between physical and emotional abuse and the diagnosis of FMS have been inconsistent.40,41 Havilan et al revealed a correlation between both sexual assault/abuse and physical assault/abuse and FMS diagnosis; however, life-threatening trauma, emotional abuse/neglect and major life stress were not found to be associated with FMS diagnosis.42
Treatment
Treatment of FMS focuses on symptom management and improving quality of life. A holistic approach that integrates physical, psychological and behavioral factors with the implementation of pharmacological and non-pharmacological strategies is helpful in managing FMS.1-3,18-21,33,35 Medications approved by the Food and Drug Administration for the treatment of FMS include pregabalin (Lyrica®; Pfizer, New York, NY), duloxetine (Cymbalta®; Eli Lilly and Company, Indianapolis, Ind.), and milnacipran (Savella®; Forest Laboratories, New York, NY).1,3,21 Non–pharmacological therapies for treatment of FMS include patient education, exercise, and cognitive behavioral therapy. Additionally, acupuncture, hypnotherapy, balneotherapy (medicinal baths), biofeedback, ultrasound, relaxation therapy and tender point injections have been reported as treatment options; however, evidence is lacking to support the effectiveness of these therapies.18,33
Oral Concerns
Most patients with FMS report symptoms of facial pain, including discomfort in the muscles of mastication, temporomandibular joint (TMJ), neck, ear and jaw.43 A study by Alonso-Blanco et al investigated the differences in prevalence and localization of referred pain areas of active trigger points between 20 women with myofacial temporomandibular joint dysfunction (TMD) and 20 women with FMS. Results revealed participants with FMS had larger referred pain areas than those with TMD for the sternocleidomastoid and suboccipital muscles.44 Leblebici et al sought to determine the correlation between FMS, TMD and masticatory myofacial pain. A group of 31 people diagnosed with FMS and a group of 21 people diagnosed with TMD completed a questionnaire and underwent a clinical examination, which included bilateral manual palpation of the masticatory muscles. The questionnaire consisted of questions about prior head and neck trauma, parafunctional habits, muscle fatigue, crepitus of the TMJ, restricted mandibular movement, jaw pain and prior TMD treatment. Results revealed 80% of patients with FMS had masticatory myofacial pain and TMD.45 This data supports previous research that indicated the high rate of involvement of the stomatognathic system in the course of FMS.46 Myofacial pain in fibromyalgic persons has also been noted in several other studies, ranging from 40.9 to 85%.43,47,48 A study by Pimentel et al revealed facial muscle pain has been reported to be 31-times more prevalent in people with FMS than those without the syndrome.43 Additionally, in a study conducted by Fraga et al, masticatory muscle pain was reported by 93.3% of people with FMS in at least one masticatory muscle.47 A study by Wolfe et al revealed jaw pain specifically was self-reported by 35.4% of individuals with FMS.49
Many patients with FMS also experience symptoms of TMD. A study by Pimentel et al investigated the prevalence of clinical features of TMD in people with FMS. Forty women with FMS were compared to 40 healthy controls using the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD). Results indicated 77.5% of the subjects with FMS met the diagnostic criteria for RDC/TMD Group I (muscle involvement) compared to 10% of the control group.43 Previous studies have also shown fibromyalgic persons have a high prevalence of signs and symptoms of TMD, ranging from 67.6 to 93.4%.45-48,50-52 Additionally, studies suggest FMS may be a predisposing factor for the onset of TMD,43,47,48,53,54 especially considering there are more individuals with FMS who have TMD than people with TMD who have FMS.45,46
Routine treatments of TMD may not benefit people with FMS because the comorbidity of these 2 conditions may result from the alteration in pain perception. Failure of the dental hygienist to acknowledge the underlying FMS diagnosis may lead to lack of appropriate treatment. Occlusal splints often recommended for patients suffering from TMD, have not been shown to be beneficial for treating myofacial pain in people with widespread pain.55 However, tactile stimulation in the form of massage has had a positive effect on clinical signs and subjective symptoms of TMD, as well as widespread pain in FMS patients who were unaffected by routine TMD treatment.56
Additional oral manifestations prevalent in FMS patients include limited mouth opening, pain upon opening and masticatory pain.43,50 Muscle and joint pain during opening and closing is prevalent with FMS.43 The prevalence of limited mouth opening has been reported to be 10 times higher in people with FMS than controls with the average maximum voluntary mouth opening for FMS patients at 41 mm, compared to 44 mm in the control group.43 The exact cause is unknown, but it is likely muscle pain during jaw movements contributes to lower range of motion during mouth opening.
Xerostomia is another common oral manifestation associated with FMS. Medications such as antidepressants, hypnotics, muscle relaxants, analgesics and anticonvulsants used to treat FMS may contribute to xerostomia.17 A study by Rhodus et al investigated the prevalence of oral symptoms in patients diagnosed with FMS. Sixty-seven women with FMS and matched controls completed a questionnaire and underwent an oral examination. The questionnaire included questions about subjective symptoms of glossodynia (oral burning), xerostomia, dysphagia (difficulty swallowing), taste abnormalities and TMD. Results revealed approximately 70% of subjects with FMS experienced xerostomia.51 Only 27.5% of FMS subjects who experienced xerostomia were taking xerogenic medications, therefore research suggests a high prevalence of xerostomia in this patient population even when controlling for xerostomia-inducing medications.51 FMS patients may experience increased caries rate, periodontal disease, dysphagia, dysgeusia (distortion of taste), mouth ulcers and candidiasis due to xerostomia.17
Glossodynia is commonly accompanied by xerostomia and dysgeusia and is experienced by approximately one-third of fibromyalgic persons.51 Glossodynia may represent hyperalgesia and allodynia resulting from nervous system sensitization.51 The neurological mechanisms responsible for glossodynia may also contribute to chronic pain in FMS. Treatment of glossodynia can be difficult due its unknown etiology. Glossodynia is a side effect of certain medications; however, it may also be caused by nutritional deficiencies, hormonal imbalances or depression.57 Tricyclic antidepressants may benefit people with FMS and glossodynia because they can be used to treat depression, which may play a role in the development of oral burning and manage chronic pain.2,17,33,57
Dysgeusia is also experienced by FMS patients.51 It is unclear whether dysgeusia represents a true oral manifestation of FMS or is a side effect of medications. Xerostomia can induce dysgeusia because normal salivary flow and concentration are essential for taste. If dysgeusia is drug-induced, patients can consult their physician about substituting another medication in place of the one causing taste disturbances.58
Patient Management
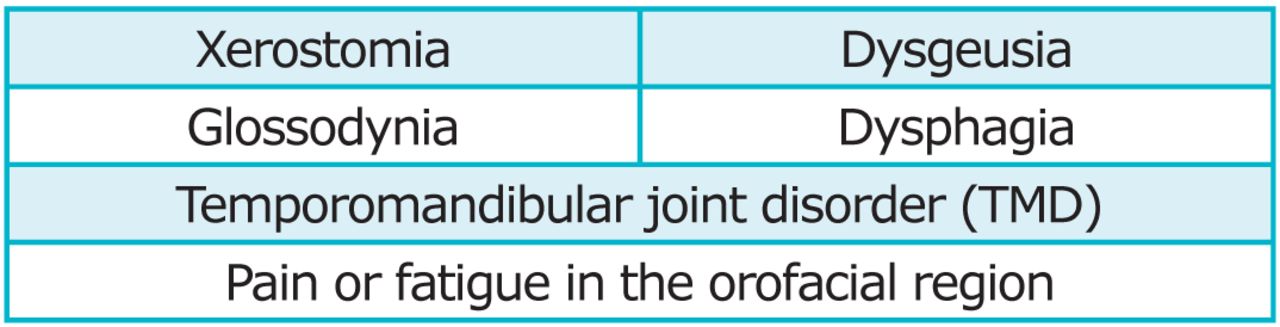
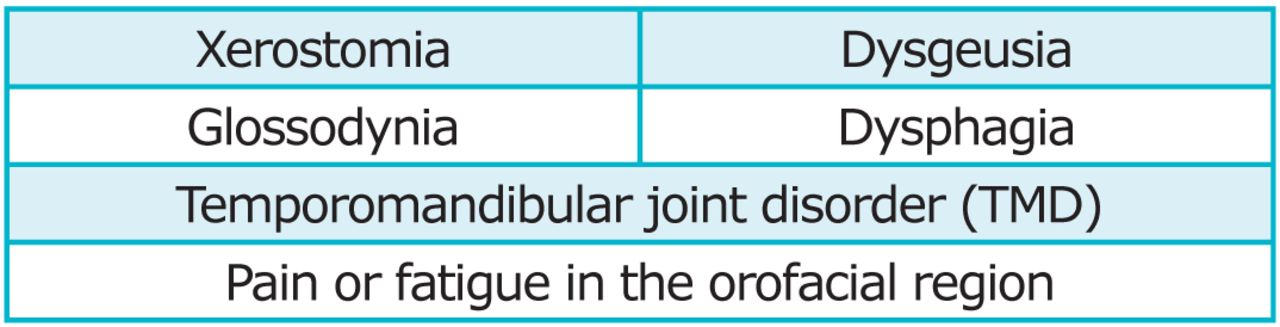
A detailed history of FMS should be documented including date of diagnosis, course of the syndrome and all current medications. Patients should be questioned about orofacial pain and headaches that may be indicative of TMD, as well as possible oral manifestations of FMS including xerostomia, glossodynia and dysgeusia (Figure 5). When performing an extraoral exam, the dental hygienist should be cognizant of possible patient discomfort in the regions of the TMJ and muscles of mastication. Additionally, if FMS is not diagnosed and suspected, the dental hygienist should refer the patient for further medical evaluation.17
Dental hygienists should consider adaptations during the process of care to ensure patient comfort and an efficacious appointment. Patients should be queried about what time of day they feel best and scheduled accordingly. Many FMS patients experience pain and stiffness that is more severe in the morning; therefore, a late morning or early afternoon appointment may work best. However, patients with FMS may cancel at the last minute complaining of pain, fatigue or lack of restful sleep. Additionally, FMS patients may not be able to tolerate long appointments due to jaw tiredness and pain. If possible, offer to break up the patient's treatment plan to accommodate shorter appointments. To promote efficiency during the appointment, a dental hygiene assistant and 4-handed dentistry is recommended. Patients should also be asked to complete medical history forms prior to arrival. To conserve energy and help prevent post exertional malaise following the appointment, a disabled parking space should be available and FMS patients should be treated in an operatory close to the reception area.
A stress-free treatment environment is ideal since stress can exacerbate the pain response in FMS patients.18,19 Strategies to help manage stress during the appointment include developing a trusting relationship between the patient and the practitioner, effective pain management strategies, and, for some patients, nitrous oxide-oxygen sedation. Muscle relaxants may also assist patients with keeping the mouth open wider and more comfortably for a longer period of time also reducing stress. Moreover, FMS patients may find breathing or relaxation exercises helpful prior to and during the dental hygiene appointment to reduce stress.
Preventing oral infection is important since infection increases stress on the body, which consequently exacerbates symptoms of FMS.19,50 Frequent recare appointments should be encouraged to help prevent oral infection and monitor oral self-care. Caution should be used when prescribing antibiotics, as they may increase therapeutic levels of other medications FMS patients may be taking such as citalopram (Celexa®; Forest Laboratories, New York, NY) and zopiclone (Imovane®; Sanofi-Aventis, Bridgewater, NJ).17 Some FMS patients may benefit by taking anti-anxiety medication or muscle relaxant prior to their dental hygiene appointment to help reduce emotional stress or anxiety. Since FMS patients often experience heightened pain sensitivity and fatigue, modifications may be necessary to ensure patient comfort and adequate pain management. Both topical and local anesthetic agents are recommended to manage discomfort during scaling and root debridement. Anesthetic agents with vasoconstrictors should be avoided for patients taking amitriptyline (Elavil®, AstraZeneca, London, UK), venlafaxine (Effexor®, Wyeth Pharmaceuticals, Madison, NJ) or duloxetine because they may create a hypertensive crisis.17 Some patients may require intravenous sedation for more extensive treatment. Prolonged periods of jaw opening should be avoided and frequent breaks may be necessary for jaw rest. During dental hygiene care, practitioners will find a mouth prop or bite block most effective as this can provide additional support for those who have limited mouth opening or fatigue easily.
Because jaw pain may persist after the dental hygiene appointment, FMS patients should be encouraged to eat a soft diet, use warm compresses in the jaw region (unless heat exacerbates their symptoms) and use analgesics such as tramadol (Ultram®; Janssen Pharmapeuticals, Titusville, NJ) or muscle relaxants such as cyclobenzaprine (Flexiril®; McNeil Consumer and Specialty Pharmaceuticals, Fort Washington, Penn) and tizanidine (Zanaflex®; Acorda Therapeutics, Ardsley, NY).17 NSAIDs (e.g., aspirin and ibuprofen) should not be recommended for patients taking selective serotonin reuptake inhibitors because they may increase the risk of prolonged bleeding.17
Patients with FMS are often hypersensitive to stimuli such as noise, heat, cold, touch and light.1,21,23 These normally non-painful stimuli may produce pain for people with FMS. Therefore, patients should be consulted about the impact of extraneous noise, such as background music, televisions and powered scalers so these can be eliminated or minimized if bothersome. A blanket or warm neck roll should be readily available if the patient gets cold. A cervical pillow can be used to support the neck better than the conventional dental chair headrest and reduce pressure on tender points located on the back of the head and neck. Additionally, since some FMS patients experience hypersensitivity to light, oral care professionals should be conscientious of not shining the dental light in the patient's eyes and tinted eyewear should be provided.
Patient Education
In order to reduce stress and improve FMS symptoms, oral care professionals should encourage their patients to live a healthy lifestyle. Poor nutrition can increase the production and secretion of stress hormones and decrease the secretion of insulin, which can lead to a lowered resistance to infection such as periodontal disease.57 Dietary counseling can be utilized when appropriate to promote healthy eating habits. Data suggests tobacco smoking may exacerbate clinical features of FMS patients.59,60 As part of encouraging a healthy lifestyle, tobacco cessation should be recommended.
Due to the debilitating effects of FMS and comorbidities, patients may have difficulty performing oral self-care. Extremities of FMS patients often feel swollen, with upper extremities more impacted than lower extremities; therefore, oral self-care may be negatively affected.61 Additionally, FMS often co-occurs (up to 25 to 65%) with other rheumatic conditions, and as a result of these conditions, some patients may experience dexterity issues.62 FMS patients with impaired manual dexterity may find powered toothbrushes, flossing devices and interdental brushes helpful.62 However, the noise from a powered device may be a problem for FMS patients with heightened sensitivity to sound. Another option is the Surround® toothbrush, which can be recommended if finances or noise prevent the purchase or use of powered devices or the patient fatigues easily.63 For some patients, modifying the toothbrush by extending or enlarging the handle may also be helpful.63 These modifications can also be performed on floss handles and interdental brushes.
Depression is another common finding with FMS patients that may have a negative effect on oral health due to lack of self-care. Dental hygienists should be compassionate and provide encouragement to FMS patients realizing self-care may not always be a priority or may be difficult to accomplish. Clinicians must be cognizant of the psychological toll FMS takes on many individuals, as well as its overall debilitating effects. Due to the high prevalence of cognitive issues resulting in decreased mental alertness and memory (fibro fog), patients may benefit from written self-care instructions and educational materials they can take home to reinforce important concepts.
Patients should be educated on the difference between the chronic, widespread FMS pain and acute pain from an oral disease or infection. Patients may attribute dental pain to symptoms of FMS and not seek immediate care, resulting in minor dental disease escalating to major. Therefore, frequent recare intervals are critical to ascertain oral disease status on a regular basis. Additionally, with frequent recare, dental needs may be identified early, and be provided before more extensive treatment is required, which may be difficult for the patient to withstand.
Dental hygienists should encourage FMS patients with xerostomia to take an active role in the management of their symptoms to minimize risk of adverse oral effects. Strategies to help alleviate xerostomia include using saliva substitutes and sialogogues, and avoiding alcohol and caffeine consumption. Saliva substitutes can be used to replace moisture and lubricate the mouth for short term relief. Sialogogues are any agent, over-the-counter or prescription, that aid in more long term relief by stimulating new saliva. Prescription sialogogues such as pilocarpine (Salagen®; Eisai, Woodcliff Lake, NJ) and cevimeline (Evoxac®; Daiichi Sankyo, Parsippany, NJ) can be recommended for patients who do not have medication-induced xerotstomia. Chewing sugar free gum with xylitol is also typically recommended for patients with xerostomia to stimulate salivary flow; however, many FMS patients experience pain upon mastication and therefore this management strategy would be contraindicated. Xylitol mints and lozenges could be suggested as they provide both caries benefit and improve salivary flow without stressing masticatory muscles.
Conclusion
FMS is a common disorder that encompasses symptoms of chronic, widespread musculoskeletal pain, fatigue, cognitive deficiency and sleep disturbances. Oral manifestations of FMS are common and affect the oral and overall health of the patient. Dental hygienists must be knowledgeable about oral signs and symptoms of FMS in order to educate their FMS patients on management strategies and oral self-care modifications. Additionally, dental hygienists should be prepared to make appropriate adjustments when treating patients with FMS to ensure hygiene care is rendered in a comfortable and effective manner.
Footnotes
-
Amber Walters, BSDH, MS, is an adjunct assistant professor. Susan L. Tolle, BSDH, MS, is a university professor. Gayle M. McCombs, BSDH, MS, is a university professor and Graduate Program Director, Director, Dental Hygiene Research Center. All are at Old Dominion University School of Dental Hygiene.
-
This study supports the NDHRA priority area, Clinical Dental Hygiene Care: Assess the use of evidence-based treatment recommendations in dental hygiene practice.
- Copyright © 2015 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}