



Abstract
Purpose: Sjögren's syndrome is a systemic autoimmune disease affecting approximately 3 million Americans, primarily perimenopausal women. The syndrome is characterized by dysfunction and destruction of exocrine glands leading to oral and ocular manifestations, xerostomia and keratitis sicca. Sjögren's syndrome commonly remains either undiagnosed or is diagnosed years after the onset of symptoms. Diagnosis is based on the concurrent presence of various signs and symptoms of the disease as established by 6 diagnostic standards set by the American European Consensus Group standards: oral symptoms, ocular symptoms, evidence of oral signs, evidence of ocular dryness, evidence of salivary gland involvement with positive Anti-Ro/La autoantibodies and a positive gland biopsy. Currently no definitive test or cure exists; treatment is predominately palliative and supportive.
Conclusion: With an aging population and heavier reliance on medications and treatments which cause xerostomia, oral health professionals are likely to encounter a higher incidence of xerostomia and Sjögren's syndrome more than ever before. The dental professional must recognize the signs and symptoms of xerostomia, include Sjögren's syndrome in their differential diagnosis, and communicate those findings and concerns to other health care providers, including the primary care physician, rheumatologist and ophthalmologist for evaluation in a timely fashion. This article discusses the dental professional's role in formulating a preventive oral health plan: meticulous oral hygiene instructions, dietary counseling, a complement of chemotherapeutic agents and more frequent recall care to avoid oral complications and improve quality of life. Dental hygienists can help patients understand the wide range of products available to substitute or stimulate salivary flow, prevent or remineralize early carious lesions and relieve candidal and bacterial infections. Ultimately this collaboration of care by the dental and medical professionals will benefit the Sjögren's syndrome patient and lead to better patient outcomes.
Introduction
There are currently over 80 types of autoimmune diseases.1 Autoimmune diseases mistake healthy tissues in an individual as an infection and then attempt to attack and destroy it. Sjögren's syndrome is one such example in which the body attacks the exocrine or secretory glands, most commonly the salivary and lacrimal glands.2 Sjögren's syndrome is one of the most common autoimmune diseases that affects approximately 3 million Americans, primarily women (9:1 compared to men) over the age of 50.3 The onset of the disease is insidious; diagnosis is often delayed for 5 or more years. Researchers are not certain why some people develop Sjögren's syndrome. Certain genetic traits may place some individuals at a higher risk of developing the disorder, and it appears that a triggering mechanism, such as infection with a particular virus or strain of bacteria, is also necessary. Stress and hormonal factors may play a role in the pathogenesis of Sjögren's syndrome since the disease predominately manifests in perimenopausal women.4
Sjögren's syndrome is subclassified into primary Sjögren's syndrome, consisting of dryness of the mouth (xerostomia) and eyes (keratoconjunctivitis sicca), and secondary Sjögren's syndrome, which is also associated with other systemic autoimmune rheumatic diseases, such as rheumatoid arthritis, lupus or scleroderma.3 Research suggest that Sjögren's syndrome is manifested in 25 to 35% of rheumatoid arthritis patients.5,6 Both primary and secondary Sjögren's syndrome share the same cardinal signs and symptoms, xerostomia and keratitis sicca; therefore, they are treated similarly.
Dental professionals are frequently the first practitioners to detect the signs of Sjögren's syndrome. Saliva is essential for the preservation of oropharyngeal health. It aids in swallowing, oral cleansing, speech, digestion and taste. Hyposalivation or chronic xerostomia can impair the patients' quality of life. Early diagnosis and treatment is vital for preventing oral complications. Intervention and treatment are of pivotal significance, including referral to other health care professionals, i.e., ophthalmologist and rheumatologist, for diagnosis and systemic intervention. Treatment is predominately palliative and supportive. With an aging population and their heavier reliance on medications and treatments, which may cause xerostomia, oral professionals are likely to encounter a higher incidence of xerostomia and Sjögren's syndrome more than ever before. An understanding of xerostomia and its management is essential to consummate patient care. Subsequent paragraphs will explore manifestations, testing, diagnostic criteria, palliative treatment and methods to monitor and maintain the health of a patient diagnosed with Sjögren's Syndrome. The objective of this literature review is to summarize Sjögren's syndrome research focusing on oral manifestations and management of dental treatment options.
Oral Manifestations
Sjögren's syndrome is characterized by dysfunction and destruction of the exocrine glands associated with lymphocytic infiltration and immunological hyperactivity.2 Research suggests that 88% of Sjögren's syndrome subjects had a reduced salivary flow rate, followed by complaints of xerostomia in the 75 to 92% range.2 Patients with Sjögren's syndrome have a range of major salivary gland involvement, mainly parotid enlargement, but also isolated submandibular gland enlargement.7
Oral manifestations are encountered with high frequency mainly due to the hypofunction of salivary glands resulting in decreased salivary secretion. Loss of the lubricating, buffering and antimicrobial properties of saliva lends to an amplified incidence of the following conditons:8
Dental erosion
Dental caries
Mucosal friability
Dry cracked or peeling lips
Angular cheilitis
Dry plaque laden coarse tongue
Erythematous tongue
Mucositis
Ulcers
Oral candidiasis
Halitosis
Oral/dental infection
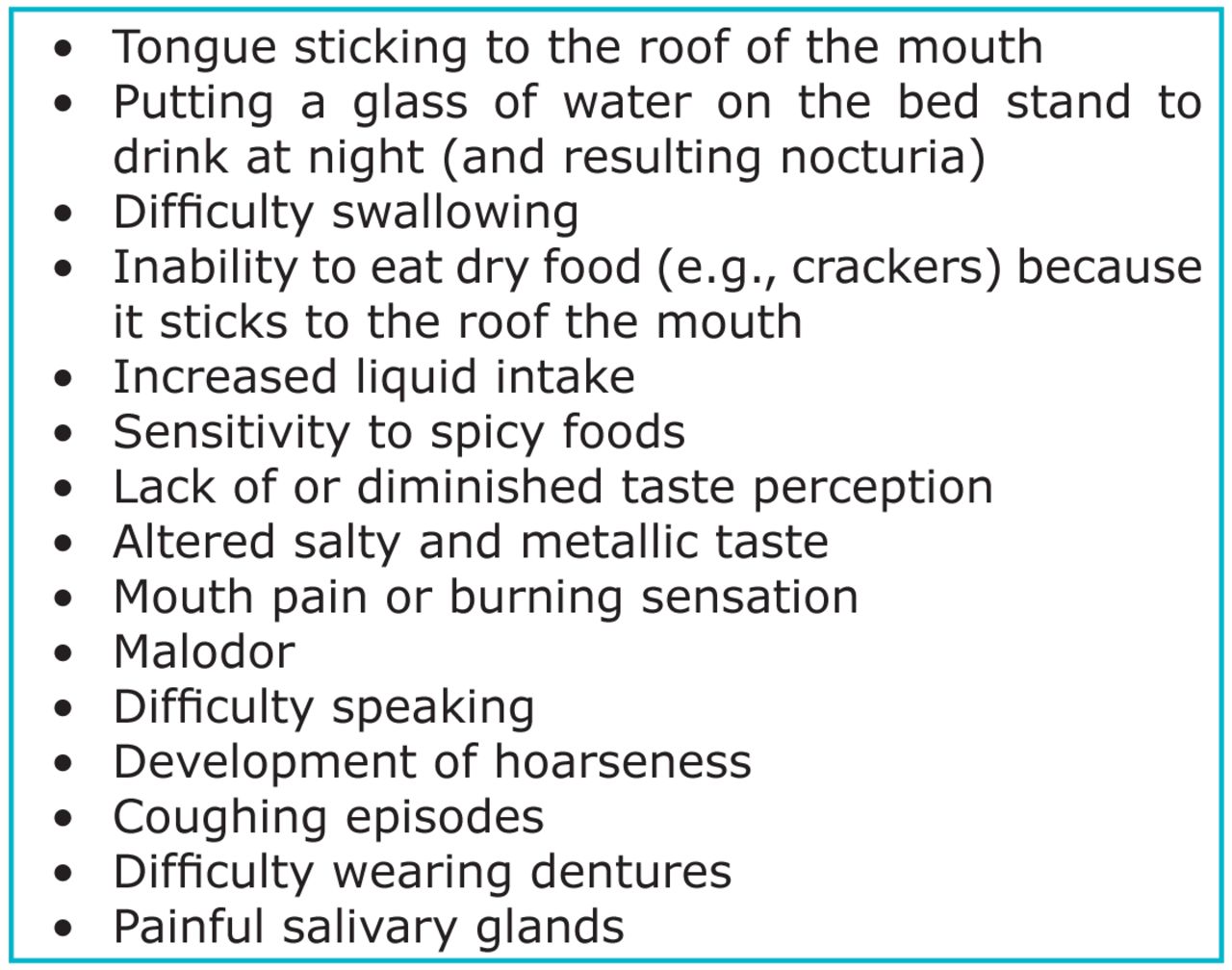
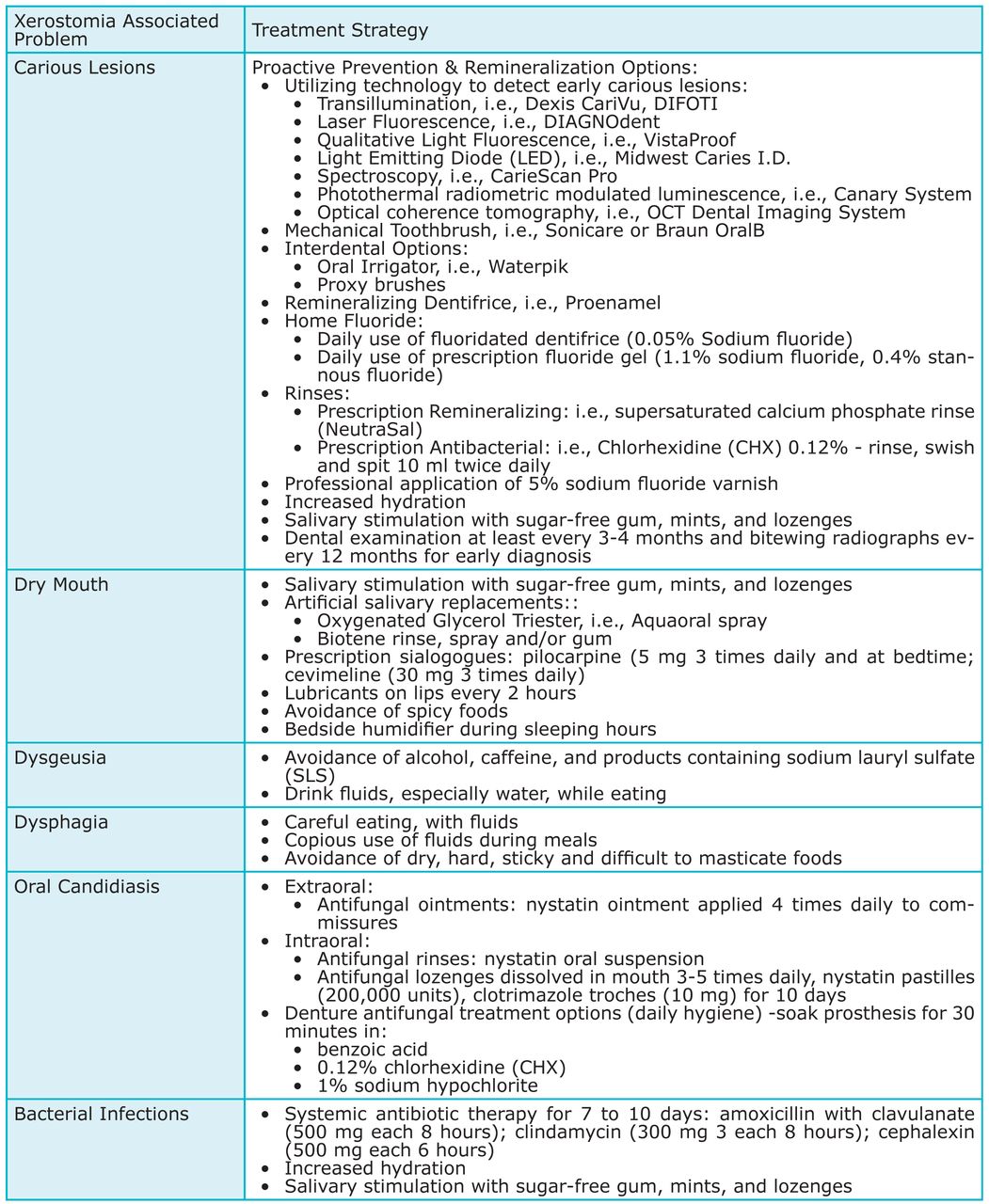
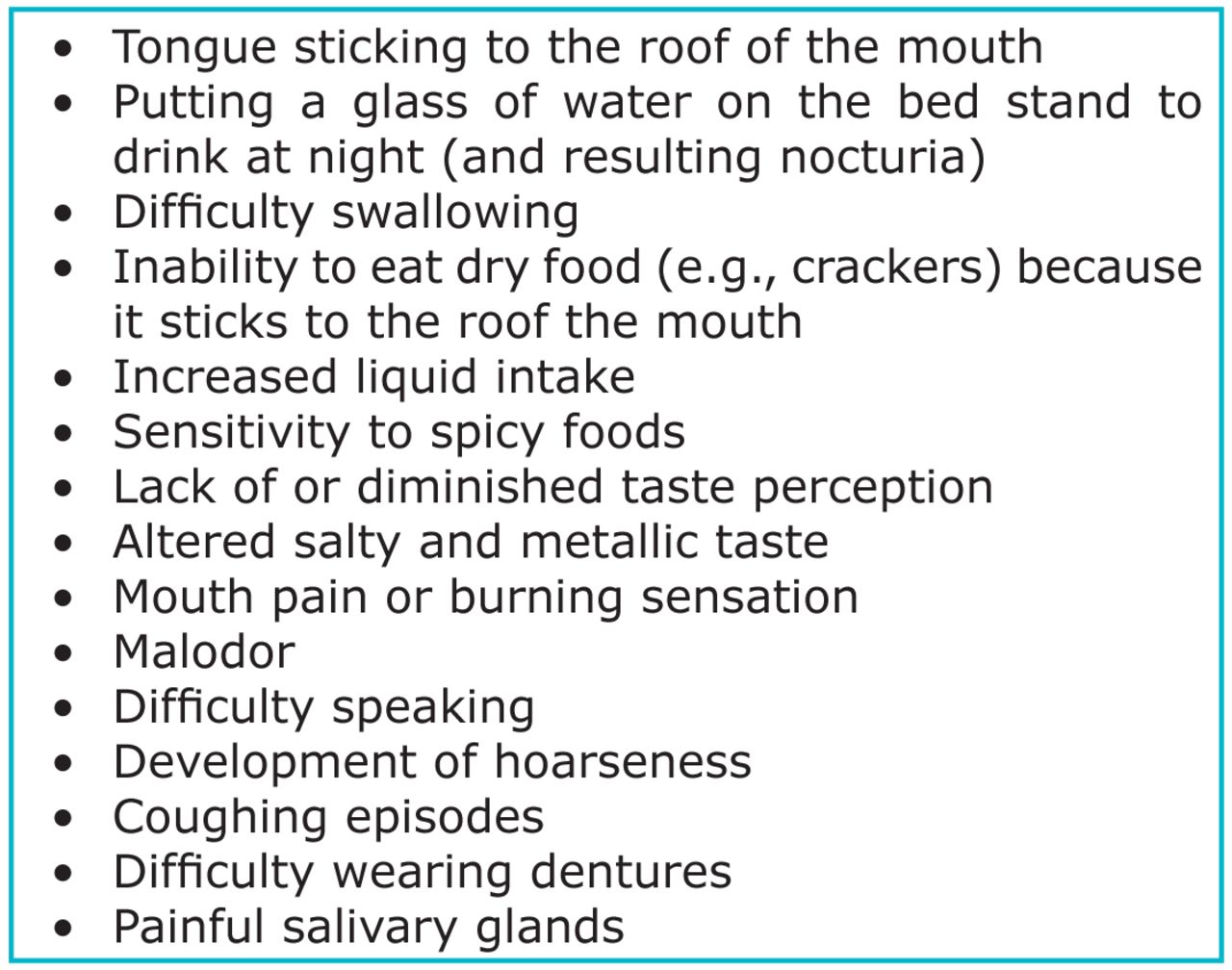
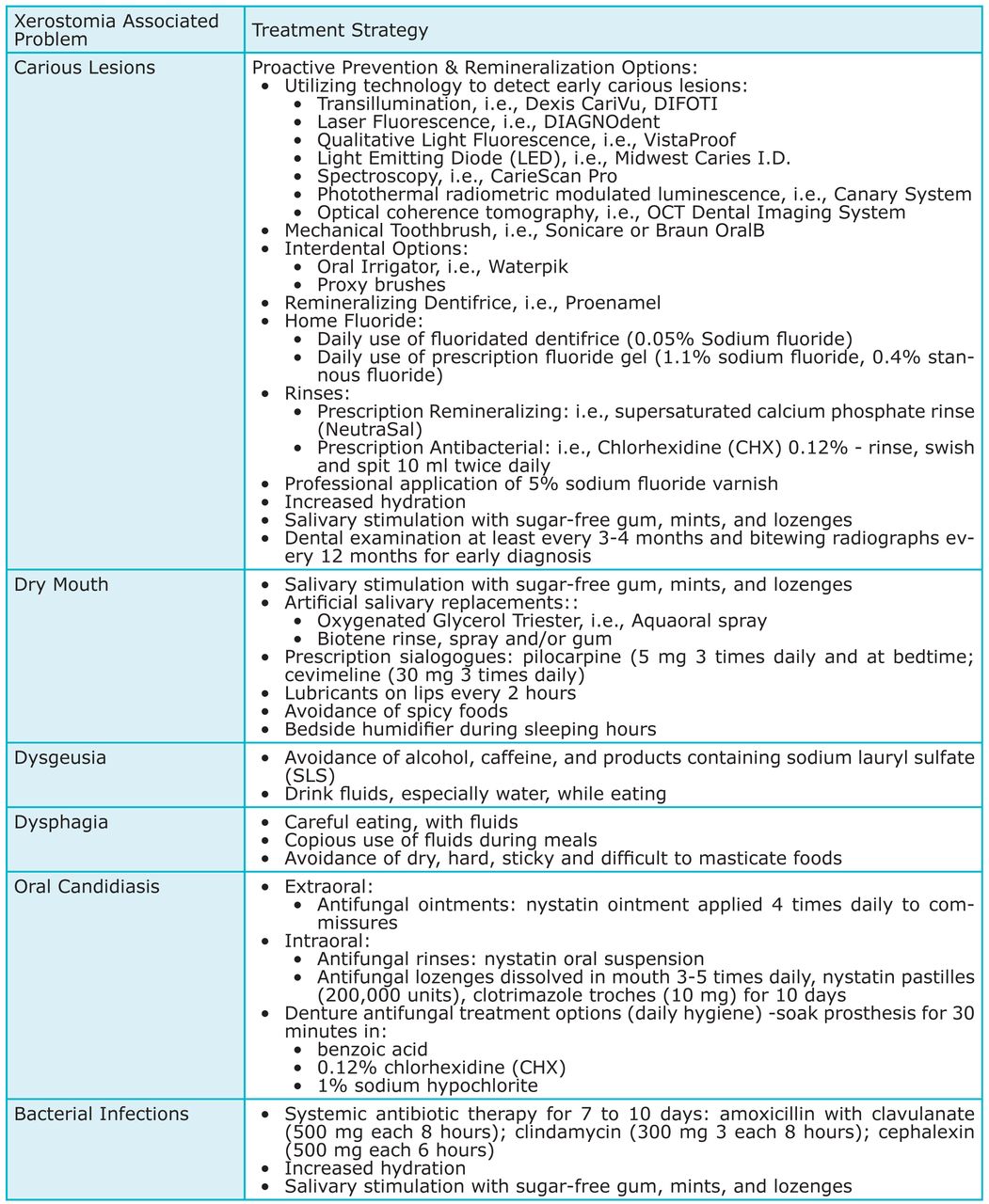
Chronic xerostomia impairs taste, chewing, swallowing, speaking and sleeping. The dental professional should document the initial symptoms (Figure 1) and recognize the multiple oral manifestations of Sjögren's syndrome.8 The dental professional therefore should have a good understanding of oral manifestations as well as viable treatment options for the Sjögren's syndrome patient (Figure 2).9
Diagnosis and Treatment
Unfortunately, testing and diagnostic criteria for identifying Sjögren's syndrome can be confounding. Diagnosis is difficult and evasive since the clinical signs and symptoms mimic other autoimmune diseases such as lupus and multiple sclerosis.10 Numerous, commonly used medications cause xerostomia and may also mimic some signs and symptoms of Sjögren's syndrome. Furthermore, there is no single test that will confirm diagnosis. Diagnostic standards used are the American European Consensus Group criteria. The criteria consists of 6 different domains:4
Oral symptoms
Ocular symptoms
Evidence of oral signs
Evidence of ocular dryness
Evidence of salivary gland involvement with a positive anti-ro/la autoantibodies (ana)
A positive gland biopsy
Diagnosis of Sjögren's syndrome is based on the concurrent presence of various oral signs and symptoms of the disease. Researchers at the Sjögren's Syndrome Foundation suggest that reaching a diagnosis takes on average 5 years from the onset of symptoms.11
Common Oral Complications
The first and foremost complication of Sjögren's syndrome is Xerostomia, and dental caries is the most common clinical manifestation. Specifically, root and incisal caries, which are seldom seen amongst the general population, are of greater concern for those with Sjögren's syndrome.7 The dental caries process involves dental biofilm and the associated species of bacteria which colonize tooth surfaces. Streptococci bacteria are most deleterious, in terms of dental caries; Sjögren's syndrome sufferers have been reported to have higher numbers of cariogenic and acidophilic micro-organisms in comparison with those found in age matched control individuals.10 In otherwise healthy people with adequate salivary output, bacteria are dislodged and expelled from tooth surfaces by the mechanical process of chewing, tongue movement and salivary flow; however, for those suffering from Sjögren's syndrome, low salivary flow does not permit the oral self-cleansing which buffers, lubricates and performs essential antimicrobial duties. One study found Sjögren's syndrome individuals with “excellent oral hygiene” who received routine 3 to 4 month recall dental treatment, and used fluoride containing dentifrices, still had elevated levels of dental caries along with premature toothloss.10
Another common, painful and often chronic complication of Sjögren's syndrome is oral candidiasis.2 Signs include Angular Cheilitis, atrophy or loss of fili-form papillae on the dorsal tongue or erythema of the tongue and other mucosal surfaces; diagnosis should be verified by positive potassium hydroxide slide and/or positive culture.2,5 A study investigating the prevalence and quantity of oral yeasts and their association with oral candidiasis in Sjögren's syndrome patients receiving regular dental care demonstrated an increase in oral yeast levels, primarily candida albicans, among participants in southern China with a “satisfactory” level of oral cleanliness.12 Results also suggest that oral yeasts were present in 84% of primary Sjögren's syndrome and 63% of seconday Sjögren's syndrome versus 7% for control subjects; interestingly, none of subjects presenting with oral candidiasis experienced any symptoms.12 A positive correlation between yeast colonization and removable dentures was also demonstrated.
Systemic Complications
The magnitude of this syndrome has far-reaching concerns beyond xerostomia, dental caries and oral candidiasis. The development of non-Hodgkin Lymphoma and central and peripheral neurological complications are extremely concerning. Non-Hodgkin Lymphoma is the most serious complication of Sjögren's syndrome.13 Compared to the general population, the lifetime risk in cohorts of unselected patients in longitudinal studies is estimated to be 5 to 15% or roughly 20-times increased risk.3,13 A predictor of lymphoma development in Sjögren's syndrome is persistent enlargement of parotid glands.3 Diffuse large B-cell Lymphoma and mucosa-associated lymphoid tissue Lymphoma make up the most common types.13 While Sjögren's syndrome manifests primarily in females (9:1), male patients with primary Sjögren's syndrome seem to have a slightly higher risk of Non-Hodgkin Lymphoma compared to female counterparts.13 A parotid biopsy may be indicated for the Sjögren's syndrome patient whose main complaint is persistent parotid gland swelling and lymphoma is suspected.3
Neurologic and systemic manifestations are among the many afflictions to which Sjögren's syndrome sufferers are vulnerable. Clinically significant neurologic manifestations affect approximately 20% of patients and may be an early manifestation.14 Patients with primary Sjögren's syndrome often present with non-specific general symptoms including non-inflammatory muscle and joint involvement, severe debilitating fatigue, weakness, neuropathies and fibromyalgia-like indicators.15,16 Primary Sjögren's syndrome has many clinical parallels with multiple sclerosis. Peripheral neuropathies, especially sensory disturbances, are the most commonly reported. Primary Sjögren's syndrome patients with sensory neuropathy complain of distal, often symmetrical, paresthesia and/or neuropathic pain including burning feet sensations.16 Cranial nerve involvement is another complication, often impairing the cochlear nerve and causing hearing loss and vestibular symptoms. Sensory trigeminal nerve involvement and facial nerve involvement are also largely described.14 Treatment of primary Sjögren's syndrome-related neuropathies are currently non-codified. Analgesics are generally the first line of defense for mild forms of sensory neuropathies; however, for more profound sensory-motor neuropathies, prednisone, azathioprine, cyclophosphamide and intravenous immunoglobulins may be prescribed.14
Oral Care Treatment and Recommendations
Since Sjögren's syndrome has no cure, treatment is symptomatic and supportive. Without sufficient saliva to restore the oral pH and regulate microbial populations, the mouth can rapidly colonize deleterious bacterial, viral and fungal populations. A personalized treatment plan must be developed for the patient by their health care professionals to treat the various symptoms. A preventive oral health plan should include meticulous oral hygiene instructions to improve quality of life, and avoid complications (Figure 2).
Mechanical toothbushing 2 to 3 times daily with a prescription fluoride gel containing 1.1% sodium fluoride, or remineralizing dentifrice
Interdental aids such as a waterpik or proxybrush in addition to flossing
Dietary counseling
A complement of chemotherapeutic agents
More frequent recall care, 3 to 4 month
Chemotherapeutic products generally fall into 2 categories: salivary substitutes (viscous products applied to the oral mucosa in the form of sprays, gels, oils, mouthwashes, mouth rinses, pastilles or viscous liquids) and saliva stimulants (such as lozenges, chewing gum and mints, which may or may not contain medication).17 Oral health professionals should have a thorough understanding of the range of products available. Patient preference and acceptability is a significant factor when recommending chemotherapeutic products for home use.
A recent study found that patients suffering from xerostomia were 3-times more likely to have difficulty eating and required water when swallowing.18 Water is the most commonly used home remedy for the management of discomfort associated with xerostomia by providing some moisture to the oral mucosa and often aiding in speech and swallowing.3,18 In mild cases, frequent sipping of water, along with dietary avoidance of certain foods and chemicals, such as alcohol, caffeine and sodium lauryl sulfate, commonly found in dental products, may alleviate xerostomia to an acceptable level.17,18 In addition to hydration, patients with Sjögren's syndrome should be advised to avoid dry, hard, sticky cariogenic foods, and especially limit the frequency of sugar-containing foods and drinks.19
Professional application of topical 5% sodium fluoride varnish, and daily home fluorides such as 1.1% sodium fluoride prescription dentifrices are preventive strategies which decrease microbe colonization and strengthen tooth enamel—thus making tooth surfaces more resistant to caries.8 Supersaturated calcium phosphate rinse (NeutraSal), a prescription mouth rinse, is a relatively new treatment option for patients experiencing Sjögren's syndrome-related xerostomia. NeutraSal contains supersaturated amounts of calcium and phosphate ions which can relieve dryness, reduce acidity (pH), and may help prevent caries through remineralization of the teeth.20
The Cochrane Collaboration published in 2011 summarizes 36 randomized controlled trials and compares topical interventions such as lozenges, sprays, mouth rinses, gels, oils, chewing gum or dentifrices for the treatment of xerostomic symptoms.17 Complex saliva substitutes attempt to mimic the protective properties of saliva through the addition of remineralizing and antimicrobial agents.18 The Cochrane Collaboration asserts that while there is no strong evidence that any topical treatment is effective for relieving the sensations of xerostomia, Oxygenated Glycerol Triester saliva substitute spray was found to be more effective than water based electrolyte spray.17 Since no commercial saliva substitute has been developed which accurately replicates all essential qualities of natural saliva, attempts should be made to increase the natural flow of saliva as much as possible.17
Sugar-free gum, mints and lozenges are advisable in those with residual capacity to encourage increased salivary production.17 Products containing cariostatic sugar alcohol, a bacteriostatic agent, such as xylitol or sorbitol, are recommended during waking hours to reduce the sensation of xerostomia and facilitate speech and swallowing.17 The Spry Dental Defense System hosts a line of products incorporating xylitol, including dentifrice, floss, rinse, spray and gum.21 GlaxoSmithKline incorporates a combination of glycerol and xylitol into their Biotene product line consisting of a gel, spray, rinse, dentifrice (also includes sodium fluoride) and gum.19 Manufacturer of Extra Professional Calcium Sugar Free gum, currently available in Australia, suggest that 40 mg of calcium per piece of gum is released within 20 minutes.22 Another gum with recaldent, currently available in the U.S., claims to remineralize hard tissue through the release of both calcium and phosphate in the form of casein phosphopeptide amorphous calcium phosphate.23 If Sjögren's syndrome patients can tolerate gum chewing, it should be encouraged as directed.
Medication induced xerostomia, an inescapable side effect of many commonly prescribed drugs, can compound the oral manifestations of Sjögren's syndrome. Drug substitutions may help reduce the adverse side effects of medications that produce xerostomia, if similar drugs are available that have fewer xerostomic side effects.8 Taking anticholinergic medications during the daytime, opposed to bedtime, can help diminish nocturnal xerostomia when salivary output is diminished during sleep. Lastly, dividing a drug dosage over the course of a day may help avoid the side effects caused by a large single dose.
Systemic saliva stimulants in the form of medication may be considered in cases of severe xerostomia.19 Two muscarinic acetylcholine receptor agonists (pilocarpine and cevimeline) are licensed for the treatment of sicca symptoms in Sjögren's syndrome.18 These systemic agents stimulate the muscarinic acetylcholine receptors M1 and M3 present on salivary glands, leading to increased secretory function.18 Adverse events associated with pilocarpine and cevimeline use include sweating and increased urinary frequency and flushing; however, these drugs are contraindicated in Sjögren's syndrome patients suffering from significant cardiovascular and pulmonary disease.3,16 These medications should not be prescribed by an oral health care professional, but rather by the physician who is intimately involved in patient care and the multiple prescriptions which the patient may already be taking. A rheumatologist may also treat a patient with Sjögren's syndrome with other therapeutics involving cytokines or immunoregulators (e.g., rituximab or hydroxychloroquine) or systemic steroids.19
The decreased buffering capacity, salivary output and the immunocompromised state in persons with Sjögren's syndrome are associated with the increased occurrence of candida infections.10 Treatment includes topical antifungal treatments and may be followed by systemic antifungal agents for persistent or recurrent episodes. A typical regimen includes antifungal cream and a pastille, troche or oral suspension of an antifungal 3 to 5 times daily for 1 week, followed by systemic treatment with an azole (Figure 2).9 For prevention of candidiasis, wearing dentures overnight should be discouraged; dentures should be cleaned and treated daily with benzoic acid, 0.12% Chlorhexidine Gluconate or 1% sodium hypochlorite, as primary Sjögren's syndrome carries a high risk of oral candidiasis and a high frequency of multiple candida infections.19 Management of these conditions requires a multidisciplinary approach, with close follow-up by a dental practitioner familiar with the complexities of salivary gland dysfunction.19
Dry climates, air-conditioned environments and exposure to cigarette smoke may exacerbate symptoms of Sjögren's syndrome.3 Complementary therapies may include the use of bedside humidifiers, which may help to hydrate the environment and diminish nocturnal xerostomia.3,8,19 An alternative therapy for Sjögren's syndrome may also include acupuncture. Acupuncture is an increasingly accepted means for controlling pain, chemotherapy-induced nausea and hot flashes; studies suggest that it may also be beneficial in relieving symptoms of xerostomia after head and neck cancer.24
Conclusion
The role of dental professionals includes the identification of patients who are at risk for oral/systemic diseases. Sjögren's syndrome patients often present first to their oral health professional because of their predominantly oral symptomatology. Prevention, early diagnosis and treatment are crucial to maintaining oral health. The dental professional must recognize the signs and symptoms of xerostomia, include Sjögren's syndrome in their differential diagnosis, and communicate those findings and concerns to other health care providers for evaluation in a timely fashion.19 A preventive oral health plan should include meticulous oral hygiene instructions, dietary counseling, a complement of chemotherapeutic agents, and more frequent recall care. The body of evidence does not support a single palliative product but rather a combination of chemotherapeutic products and encourages the action of sugar-free chewing gum during working hours to stimulate host salivary production.17 Inclusion of commercial saliva substitutes should be tailored to the individual patient's concerns, preferences and oral health needs to help manage the symptom of xerostomia.18
Multidisciplinary management of underlying systemic conditions, such as Sjögren's syndrome, is imperative to help reduce oral complications. Management of the Sjögren's syndrome patient may include the primary care physician, rheumatologist, dental professional, ophthalmologist and gynecologist.16 When health care professionals work together as a team they can improve patient outcomes and quality of life for the patient diagnosed with Sjögren's syndrome.
Footnotes
Deborah L. Cartee, RDH, MS, is an Assistant Professor and Junior Clinical Coordinator in the Division of Dental Hygiene at the University of Maryland, School of Dentistry. Shannon Maker, RDH, BS, and Debra Dalonges, RDH, BS, completed this project in partial fulfillment of the Bachelor of Science Degree Completion Dental Hygiene Program at the University of Maryland, School of Dentistry. Marion C. Mansk, RDH, MS, is an Associate Professor and the Director of Dental Hygiene Program, University of Maryland School of Dentistry.
This study supports the NDHRA priority area, Clinical Dental Hygiene Care: Investigate how dental hygienists identify patients who are at-risk for oral/systemic disease.
- Copyright © 2015 The American Dental Hygienists’ Association





{kind=link}
{kind=link}