



Abstract
Purpose: Children from low-income families and ethnic minority groups are associated with an increased risk of developing dental disease and are often enrolled in the Women, Infants and Children (WIC) nutritional program. It has been an intention of the Michigan Department of Community Health (MDCH) Oral Health Program (OHP) to collaborate with WIC to provide preventive oral health resources and education to their population. This project focused on achieving the goals outlined in the Michigan 2010 State Oral Health Plan.
Methods: An 18 question survey was designed to identify gaps existing in oral health counseling in Michigan WIC agencies. The survey was disseminated to 56 MI WIC agencies.
Results: WIC providers perceive oral health risk assessment to be important and are asking oral health questions during certification and re-certification appointments. Seventy-nine percent of participants indicated they never had training in oral health counseling, and 79% are interested in learning more about oral health. Agencies are interested in obtaining oral health education resources for their clients.
Conclusion: The 2010 State Oral Health Plan's goals recognized the need for oral health related resources and education within community-based programs like WIC. The results of the survey support the need for additional oral health counseling and associated resources in WIC agencies. This information will be used to help the MDCH OHP find ways to address these gaps.
Introduction
The mission of the Michigan Department of Community Health's (MDCH) is to “protect, preserve, and promote the health and safety of the people of Michigan with particular attention to providing for the needs of vulnerable and under-served populations.”1 The Special Supplemental Nutrition Program for Woman, Infants, and Children (WIC) is a federally-funded program that provides nutritious food supplementation, education, screening and referral to health and social services.2 WIC partners with the health care community, receiving referrals from private and public health care providers. WIC also refers participants for immunizations, substance abuse counseling/treatment, prenatal care, smoking cessation programs, lead screening, and in Michigan, refers children to the Healthy Kids Dental/MI Child dental services program.2 The MDCH Oral Health Program (OHP) has been strategically interested in working with WIC to identify the needs associated with oral health education and available recourses.
The purpose of this study was to investigate WIC providers' perceptions of oral health counseling and availability of associated resources. The aim was to assist the MDCH OHP in identifying gaps in oral health counseling training and needed health education resources for WIC providers.
MDCH
The MDCH designs programs to improve health outcomes and the quality of life.3 The OHP focuses on improving the oral health of all Michigan citizens. WIC is a health and nutrition program that has demonstrated positive health outcomes for pregnant women and their children.3 It has been a strategic goal of the MDCH OHP to increase collaboration with community–based programs like WIC to provide preventive oral health resources and education to their population (Deming, personal communication, January 2012).
WIC Nutritional Program
The at-risk low-socioeconomic population served by WIC is comprised of pregnant, breastfeeding and non-breastfeeding postpartum women in addition to infants and children up to 5 years of age.2 WIC's objective is to improve fetal growth and development, improve health and development of infants and children, and increase access to health related services.2 It is the third largest nutrition assistance program in the U.S. with 10 million participants and a reported annual expenditure of $6.8 billion in 2010.2
Michigan Department of Community Health State Oral Health Plan
The MDCH, Michigan Oral Health Coalition and numerous stakeholders across Michigan developed the 2010 State Oral Health Plan. The purpose of the plan was to provide goals and objectives to increase access to oral health care and evaluate progress towards meeting both national and state health objectives.4 The plan identifies strategies that can be implemented to improve oral health, opportunities for research, encourages development of preventive and restorative programs to reduce disparities, provides vital resources of information for lawmakers, and empowers local advocacy groups to pursue policies to improve oral health.4
The plan has 10 goals with accompanying action steps. Two goals are applicable to the WIC population. The MDCH OHP recognized the importance of partnering with WIC to achieve the following 2 goals.
Goal 2: Implement evidence-based preventive practices that maintain optimal oral health for Michigan communities. Action Step: Research evidence-based dentistry to maintain optimal oral health for Michigan's communities to include:
Research and promote prenatal and postpartum oral health care
Infant oral health
Mandatory oral health exams prior to school enrollment and prior to 5th grade with a mechanism for referral to insure comprehensive care
Adult dental access
Elderly dental access
Special populations access4
Goal 4: Provide information about the availability of comprehensive and culturally sensitive oral health education resources. Action Step: Partner with organizations (e.g., WIC, Head Start, Maternal Infant Health, Children's Special Health Care Services, Area Agencies on Aging/Healthy Aging Initiative, special needs organizations, Disability Council, National Institute of Dental and Craniofacial Research, etc. to provide resources to support comprehensive and culturally sensitive oral health education and prevention activities.4
The Pregnant Patient and Oral Health Issues
The WIC population has an increased risk for oral diseases for several reasons. The inability to access or afford regular dental care can lead to untreated tooth decay and periodontal disease.5 Untreated oral health issues will place an individual with an increased risk of other health problems. Pregnant mothers experience temporary adaptive changes to their bodies causing an increased production of various hormones making her more susceptible to gingival and periodontal diseases.6 According to the 2010 State Oral Health Plan, 25% of pregnant women did not see the dentist at all during pregnancy, and 38% visited the dentist just once in the previous year.6
Investigators have reported a potential association between preterm delivery/low birth weight and the presence of inflammation.7 Some studies suggest that pregnant patients with existing or developing oral conditions like gingivitis or periodontitis and poor oral hygiene are at great risk for preterm delivery/low birth weight infants.8-10 Morning sickness or nausea is quite common for many pregnant women. The gastric acid entering the oral cavity after vomiting may cause lingual enamel erosion on the maxillary anterior teeth.11 After several episodes the enamel may break down resulting in an increased risk for dental caries.
Early Childhood Oral Health Issues
The Centers for Disease Control and Prevention report that dental caries is the most prevalent infectious disease affecting children in the U.S. with WIC children being at higher risk.12,13 Forty percent of children have decay by the time they begin school.14 Early childhood caries (ECC) is defined as beginning soon after tooth eruption and progressing rapidly.13 ECC affects the general population but is 32-times more likely to occur in infants who are of low socioeconomic status, who consume a diet high in sugar and whose mothers have a low education level, such as children of mothers enrolled in WIC.13
Dental caries is a preventable disease. Determining caries risk in children, providing education on oral health matters to their parents and caregivers, and controlling demineralization are important in prevention.15 Interventions, especially through public health initiatives are important, practical and an inexpensive way to help reduce the occurrence of dental caries in children.15 WIC is one such public health initiative.
Oral Health Counseling
Oral health counseling consists of providing advice and utilizing persuasive approaches to positively impact a person to adopt a health conscious lifestyle.16 Health care providers, such as those who work with the WIC program, can help clients make decisions about behavior change and provide them with necessary resources. A study by Butani et al assessed attitudes towards oral health counseling by Illinois WIC providers.5 Twenty-seven percent of the participants reported that they had some form of oral health training, mostly through continuing education programs, while 61% reported feeling either “very comfortable” or “comfortable” in discussing oral health issues with their clients.5 The 3 top reasons for being “somewhat comfortable” or “not comfortable at all” were lack of oral health knowledge, busy workplace and lack of confidence in addressing oral health issues.5
When the WIC participants were asked the question “how often in the last three months was any time spent discussing oral health,” 60% reported spending some or little time discussing oral health with their clients, and only 13% reported having these discussions with all of their clients.5 Results of this study show that WIC providers are interested in offering oral health counseling and resources to their clients. However, it is important for providers to receive appropriate training to be more comfortable and knowledgeable about oral health concepts to improve the oral health status of their clients.5
Oral health counseling is an important component of WIC programs. Training and appropriate resources for WIC providers are essential to adequately address oral health issues. Agency collaborations, such as those developed by the MDCH OHP and WIC, can execute initiatives that focus on improving the health of the WIC population. Therefore, the purpose of this study was to investigate WIC providers' perceptions of oral health counseling and availability of associated resources. The aim was to assist the MDCH OHP in identifying gaps in oral health counseling training and needed health education resources for WIC providers.
Methods and Materials
An 18-question survey consisting of multiple choice and open ended questions was developed in collaboration with the administration of the MDCH Oral Health and WIC Programs (Table I). The study protocol was presented to the MDCH Institutional Review Board for review and received exemption status.
To determine content validity, a survey pilot testing process was conducted with 3 WIC staff members. Modifications to the survey were made based on feedback. The final survey was emailed to a convenience sample of all 56 WIC coordinators in Michigan, each being asked to identify 1 competent professional authority (CPA) or registered dietician (RD) staff member from their agency to complete the survey. The CPA or RD are providers that have the majority of the health related interaction with the WIC clients and were determined to be best suited to participate in the survey.
An email introduction/invitation was sent that included the purpose of the project, the intended significance, informed consent and a link to participate via SurveyMonkey. The survey was open to participants for 3 weeks with reminder notifications emailed twice. The survey results were analyzed by obtaining descriptive statistics, specifically the number of respondents and percent of respondents, for each survey item.
Results
Out of the 56 surveys sent, 48 were started. However, 46 surveys were actually completed resulting in a response rate of 80%. Participants were well distributed throughout the state. The numbers of respondents to each question are reported with the related results.
The majority of the participants were RDs (42%) or CPAs (42%). Thirty-five percent of the participants were WIC Coordinators and 20% were registered nurses. A small percentage were nutritionists, clerks or techs. In addition, 6 in the “other” category included 3 breastfeeding coordinators, 2 WIC supervisors and 1 enrollment eligibility specialist.
Oral Health Counseling
Seventy-nine percent of the participants indicated they had no prior training in oral health counseling. Those who had were asked how they obtained this training, indicating to choose all that apply. Of those who had training, 2 had prior oral health counseling education during their college/university coursework and 1 obtained training during a continuing education (CE) course. The majority, 6, listed “other” as their response with 1 of the participants being a dental hygienist and the others identified that they had participated in an in-service taught by a dental professional.
Oral Health and the WIC Client
Participants were asked about the certification process that the mother completes at the initial appointment and every 3 months thereafter. During these appointments, several specific certification questions are used to determine health risks related to the mother and her children. The findings are then used to design a unique education session for each family. The survey question asked if the dentally related questions already included are adequate for assessing oral health risk. The majority of the participants indicated that the subject matter of the questions used during a certification and recertification appointment are adequate (Figure 1). Thirty-two percent responded “other” and felt that topics such as asking if the child has seen a dentist, sugar intake frequency and identifying problems that effect eating are helpful in determining oral health risks.
WIC Survey Questions
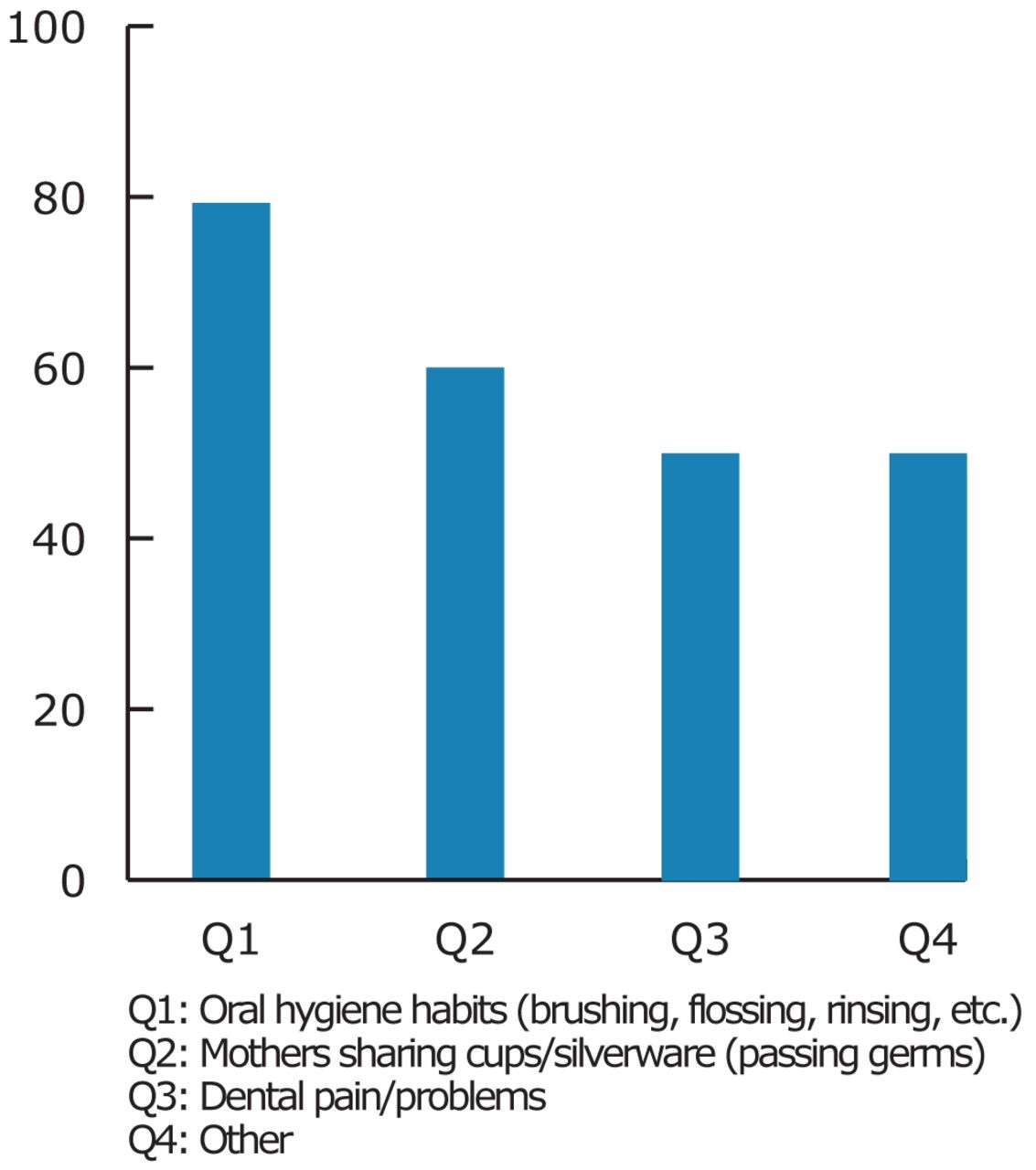
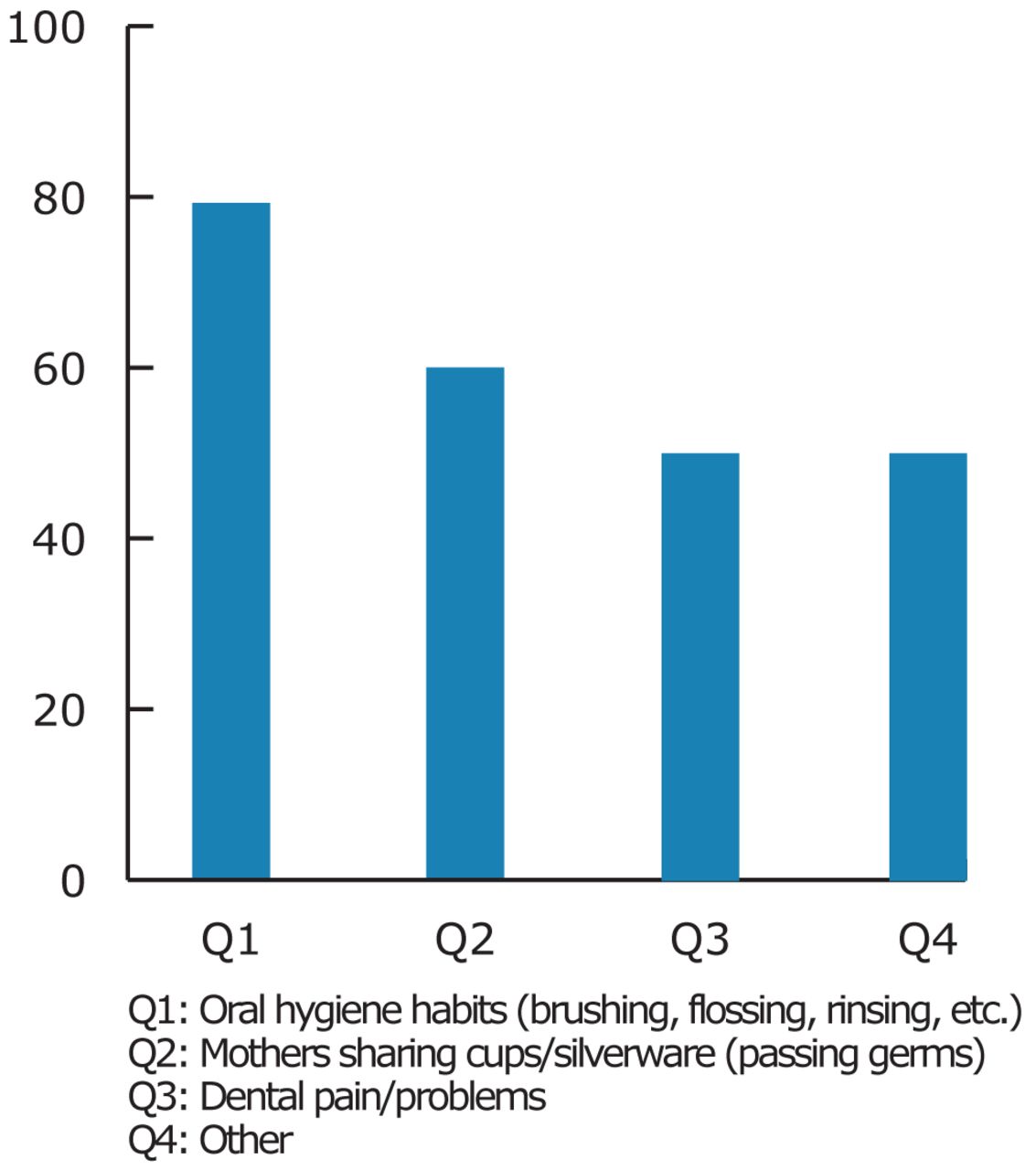
Participants were asked to identify other dental-related risk topics to help make referrals. The most pertinent risk factors were oral hygiene habits (79%), sharing utensils (61%) and dental pain (49%) (Figure 2).
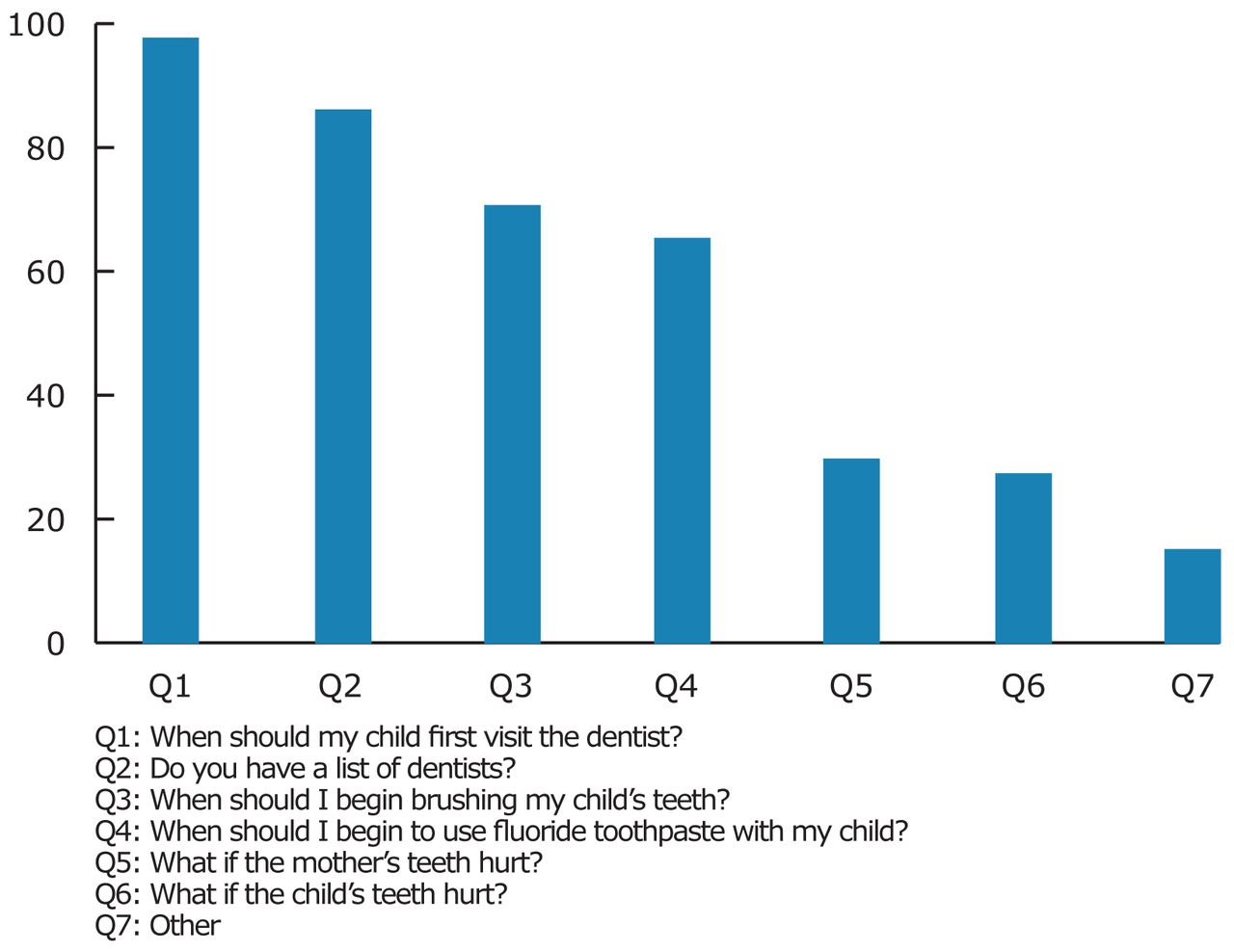
WIC clients often have their own questions about oral health. Figure 3 shows that 98% of WIC providers have been asked when the child's first dental visit should occur. The “other” responses included questions about children having tooth problems, dental clinics for the uninsured, Medicaid dental coverage for mother and child, and when to give fluoride drops to infants.
Oral Health Counseling Training
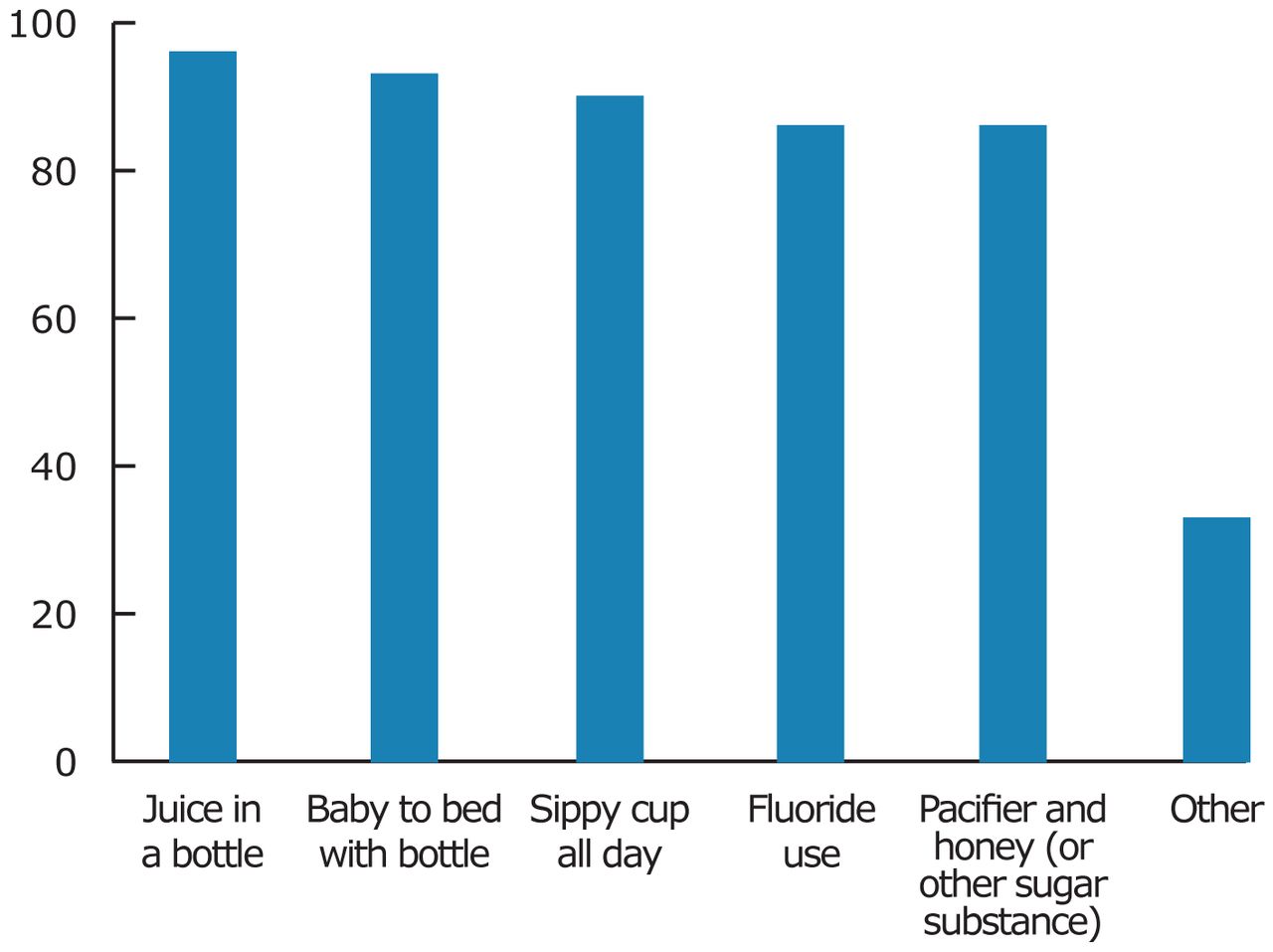
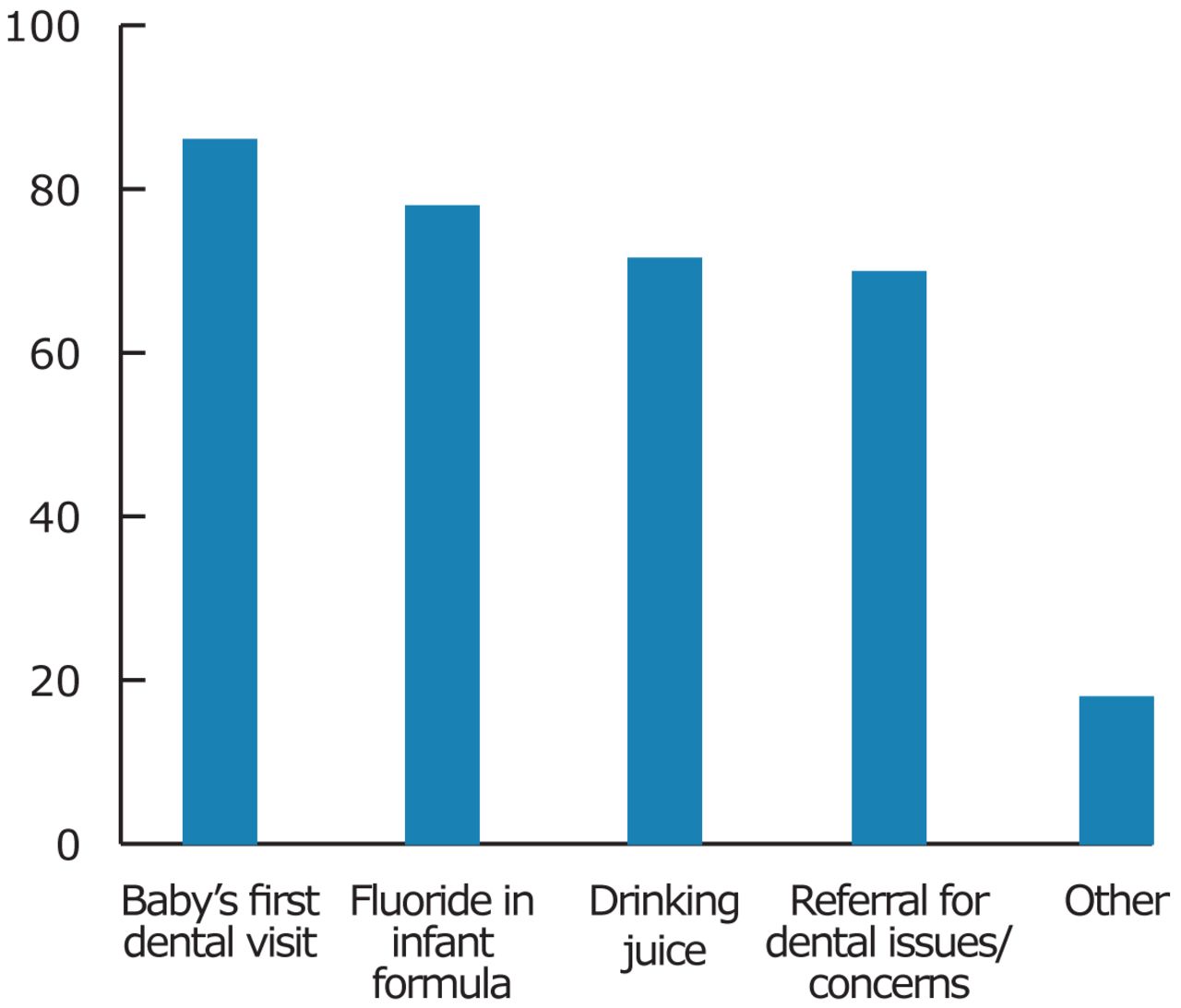
Seventy-nine percent of the participants indicated they were interested in additional oral health training. Of the training topics listed, the baby's first dental visit (87%) and fluoride in infant formula (78%) were most requested (Figure 4). In the “other” category, participants listed fluoride counseling, care of infants' oral health and pregnancy oral health, bottle use over 1 year/baby bottle tooth decay, the importance of regular dental visits, and proper brushing techniques.
Participants were asked about the preferred delivery method of additional training. Figure 5 shows that 72% would prefer webinars/web casts and 70% online learning modules. Almost half (46%) prefer training at the WIC Annual Conference.
Oral Health Resources
One of the responsibilities of the WIC agency is facilitating access to dental care. Eighty-one percent of the participating WIC agencies have a list of licensed dentists who would accept referral patients. When asked about the availability of patient education materials, 69% indicated they have the resources. If the participant identified materials would be helpful they were then asked to list what topics. Topics they would like to have in resource materials are sippy cup risks and baby bottle tooth decay, first dental visit/importance of regular care, fluoride recommendations, referral list to dental offices that accept Medicaid, and how to brush properly. Those that identified they had educational materials indicated that most were available only in English. However, some agencies had resources in Spanish, Arabic, Albanian, Hmong and Bengali.
Fifty-three percent of survey participants have access to toothbrushes and toothpaste for the WIC clients. Many purchase these with their agency's funds and some receive donations from local vendors, local dentists or outreach programs.
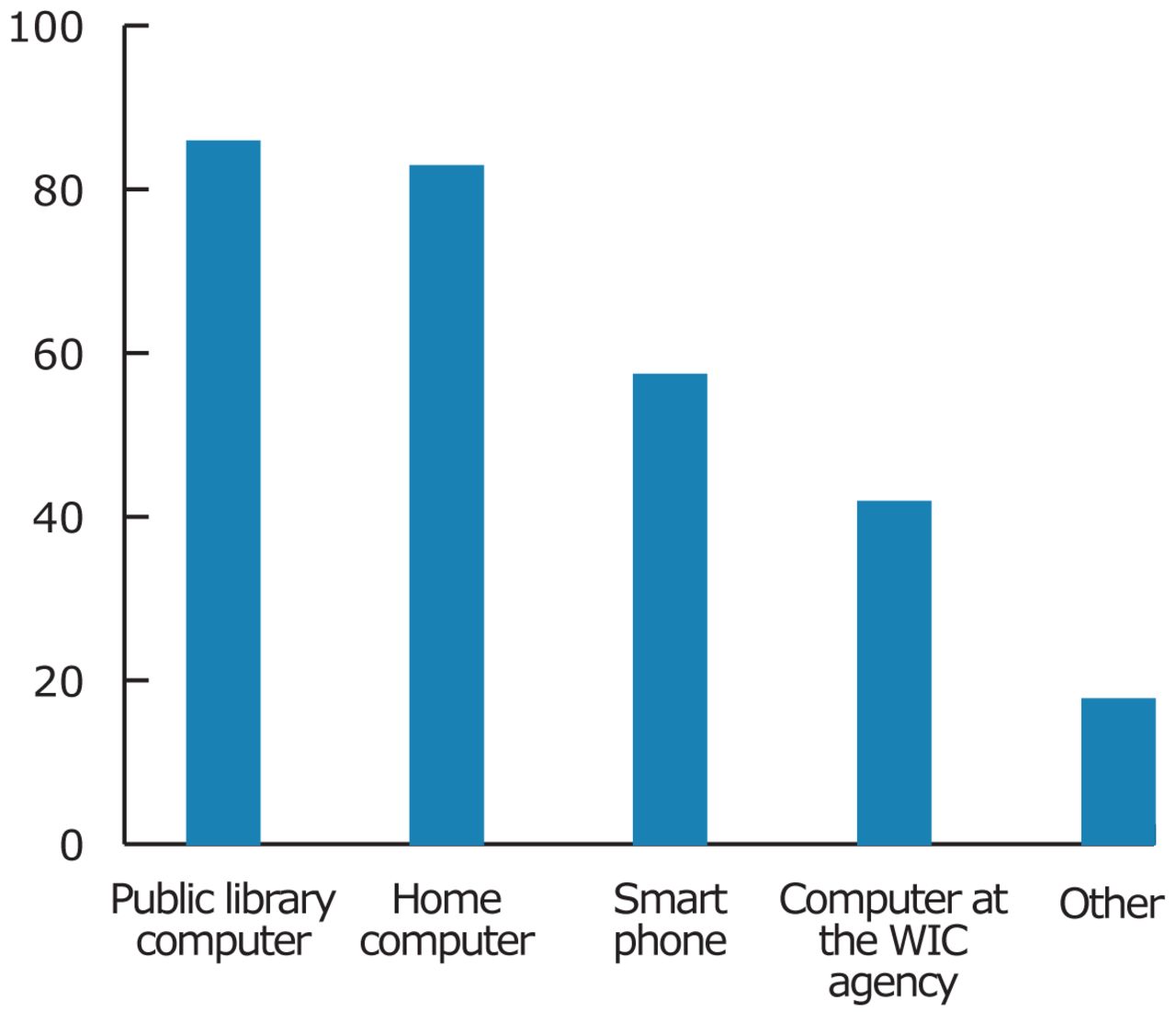
When asked if clients have access to electronic devices that could be used for education purposes, 85% noted their clients have access to computers at a public library, home computers (83%), smart phones (54%) and 41% have a computer at the WIC agency (Figure 6). Seventeen percent indicated their clients have no electronic devices, or have friends with a computer. The majority (96%) of WIC staff members have directed clients to online resources such as WICHealth.org lessons for general health information. Seventy-one percent of participants have a resource sheet or website to access if clients ask oral health related questions.

In Routine Certification and Recertification Appointments, are the Following Questions Adequate for Assessing Dental/Oral Helath Risk (percentage) (n=47)?
Are You Interested in Other Dental-Related Risk Questions to Make Referrals (percentage) (n=43)?
Discussion
The survey identified a gap between oral health counseling and WIC programs. A majority of the participants indicated that they had no prior training in oral health counseling. If WIC providers do not have proper training in oral health counseling it can have an effect on their comfort level in educating their clients about oral health or have the expertise/resources to do so. It is significant that agencies are interested in additional oral health training. A majority prefer this by means of webinars/web casts which would not require travel for participation. Another respondent recommended that the training should be archived for future usage. The MDCH OHP will be able to use the findings to help address the gaps existing in oral health counseling at WIC agencies. In addition, it will assist in achieving the goals included in the 2010 State Oral Health Plan, which are to collaborate with WIC to provide preventive oral health resources and education to their vulnerable population.4
Participants indicated significant interest in additional oral health training and identified a list of possible topics. Information on how to alter clients' attitudes on the importance of regular dental checkups for their children was requested. Other concerns correspond to the frequent patient questions/concerns about fluoride, bottle use and additional information on the baby's first dental visit. This information can assist the MDCH OHP in identifying possible training topics to offer to WIC providers. Additional training could also increase the confidence of WIC providers in addressing oral health issues.5
A majority of survey participants indicated that additional oral health risk assessment questions should be asked during WIC certification and recertification appointments. Having a thorough oral health risk assessment of the clients would help WIC providers deliver individualized patient education and resources during appointments. WIC providers are interested in addressing the oral health needs of their clients and having additional risk-related questions would support their ability to do so.5
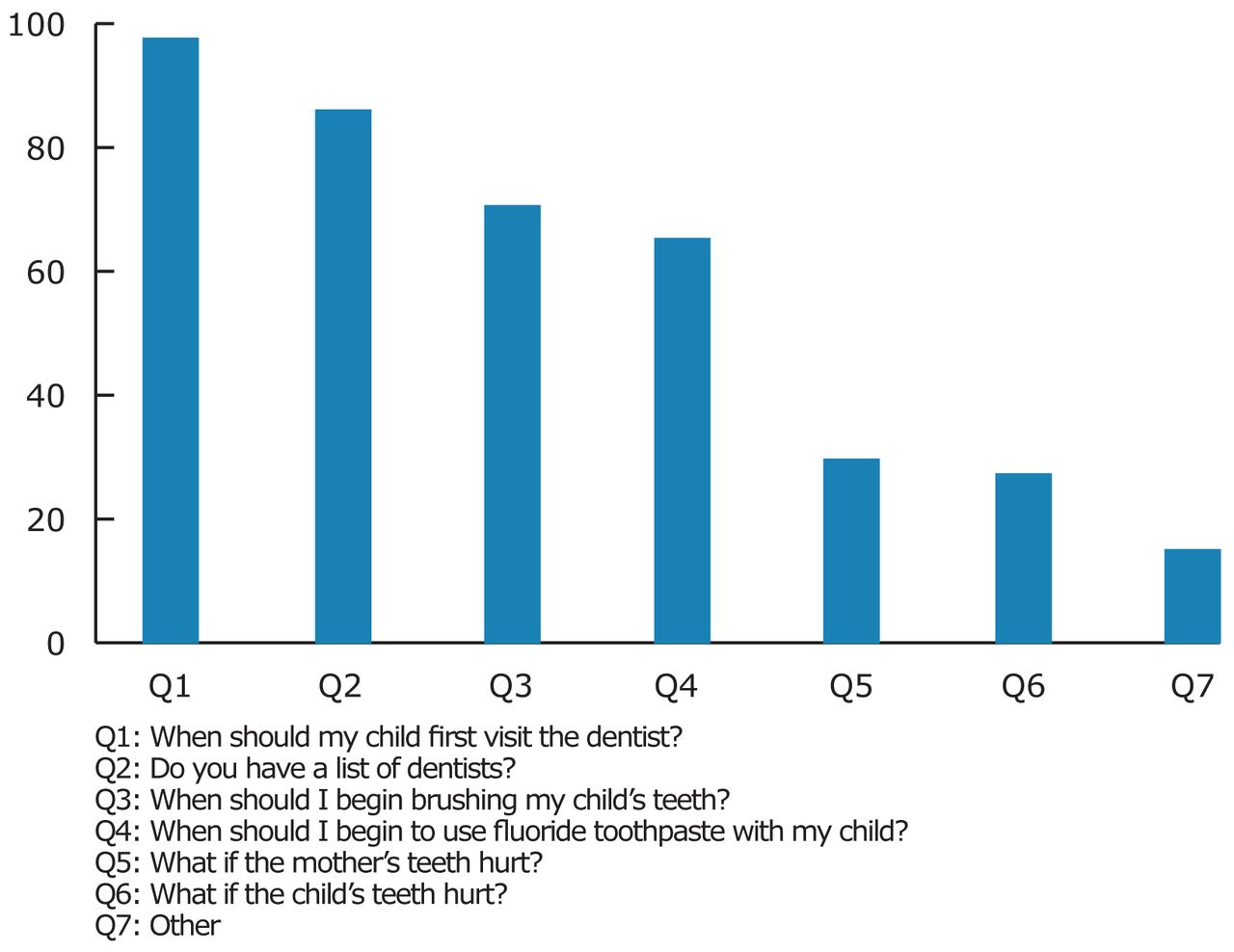
What Questions and Concerns From WIC Clients Related to their Dental/Oral Health Have You Experienced (percentage) (n=47)?

Topics Requested for Additional Oral Health Training (percentage) (n=37).
Many WIC providers find clients ask questions about how to find an oral health care provider for their children. The findings showed that a dental provider referral list available for dissemination to patients would be helpful. However, 81% said that they already have a list of dentists for referrals. It is unclear why this discrepancy exists. It could be possible that the referral lists are out of date, providers on the list are not convenient for the clients, or the providers are not taking new patients. It is recommended that the MDCH OHP explore this issue and, if needed, create a current list of referral dentists in each county for associated WIC agencies.
In addition to dental referrals, patients inquire about fluoride recommendations. Clients ask questions about fluoride supplements, the safety of fluoride and fluoride toothpaste. It is recommended the MDCH OHP provide an evidence-based fluoride recommendation reference sheet designed for pregnant women, infants and children. This supports the need for public health interventions that are important, practical and inexpensive in the reduction of dental caries.15
Survey participants would also be interested in additional oral health resources like pamphlets and toothpaste/toothbrushes for their clients. Many agencies obtain their own toothpaste/toothbrushes for their clients either through their own funding or via donations. However, all participants indicated they would like to have these supplies available to disseminate to WIC clients. Finding a sustainable source of funding for these supplies is recommended.
A majority of agencies have oral health brochures. However, the need for additional topics related to frequent client questions/concern was indicated. In addition, obtaining language appropriate information would be a recommended area for the MDCH OHP to explore.
Participants indicated that many of their clients have access to the Internet. Whether this is through personal devices, at a public library or at the agency, online oral health resources specific to WIC needs could be a beneficial means of education for clients. An oral health online resource list would be valuable to develop and disseminate to WIC agencies. Because most WIC staff members direct clients to online resources, such as WICHealth.org lessons, it is recommended that the MDCH OHP explore this website and consider contributing oral health related lessons.
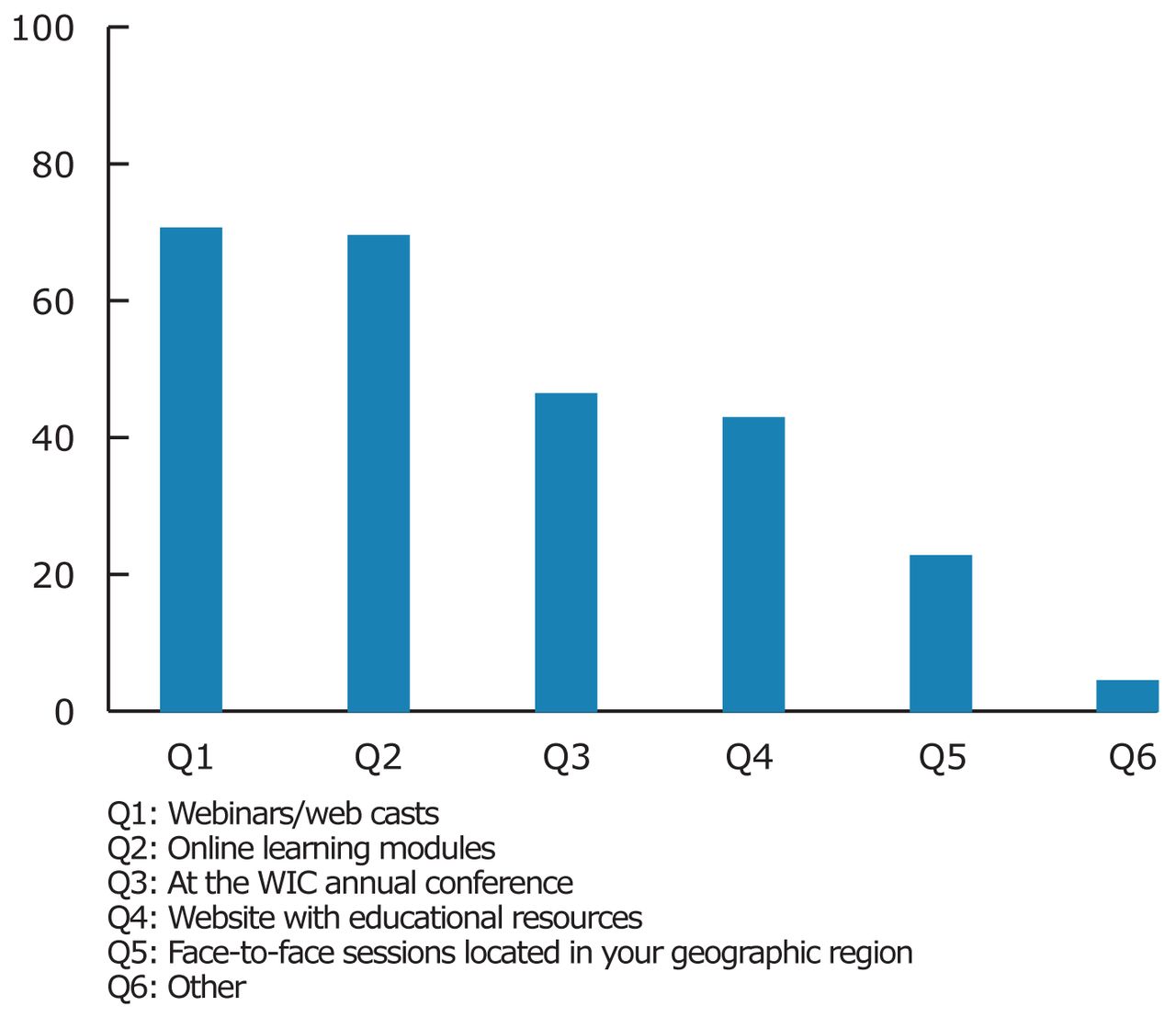
How Would Your WIC Agency be Interested in Having this Training Provided (percentage) (n=48)?

Do Your WIC Clients Have Access to Any of the Following (percentage) (n=46)?
Upon beginning the survey, each participant was asked to identify their role at their agency. In reviewing the results, this question was determined to have limitations for 2 reasons. Some respondents had multiple roles at WIC so it was unknown which was their primary responsibility. Also, this question did not inquire about participants' direct contact with WIC clients at certification/recertification visits. Thus it is unclear what basis they had for their responses about oral health risk assessment and client oral health questions later in the survey.
Additional oral health counseling training and associated resources has been identified as a need by WIC providers. Dental hygienists' educational background and knowledge about nutrition and health behavior change would position them well to assist in developing lessons, resources and/or to serve within WIC. This interprofessional collaboration could be of benefit to the MDCH OHP, WIC clients and providers, and could also serve as an enhanced career opportunity for dental hygienists. Recommended areas of further study include the investigation of interprofessional collaboration initiatives with WIC agencies and their impact on providers and clients.
Conclusion
The Michigan 2010 State Oral Health Plan goals recognized the need for oral health related resources and education within community-based programs like WIC. This study supports collaboration between WIC and the MDCH OHP to find ways to improve the oral health status for low-income families. The results of the survey indicate a gap exists in oral health counseling in Michigan WIC agencies and acknowledges that providers are interested in additional oral health training and resources. These recommendations will assist the MDCH OHP in developing a plan to address these issues. Additional research is suggested to assess the specific WIC related oral health counseling/resource needs for each geographic area in Michigan. Assessing each area will provide a better understanding on how to appropriately address the needs for that population and how to provide applicable training for WIC providers.
Acknowledgments
The authors would like to thank Susan Deming, RDH, RDA, BS, Education and Fluoridation Coordinator-Michigan Department of Community Health Oral Health Program who served as the project advisor. Appreciation is also extended to Jean Egan, Training, Evaluation and Compliance Unit-WIC and Kaitlin Skwir, Michigan WIC Staff Training Staff, and Christine Farrell, RDH, BSDH, MPA, MDCH Oral Health Program Director, who served as project consultants. In addition, the authors are grateful to Jane Halaris, RDH, BS, MA, for her assistance in the initial review of this study's documentation.
Footnotes
-
Tiffany A. Mendryga, RDH, BSDH, is a 2012 graduate of the University of Michigan Dental Hygiene Degree Completion Program. Anne E. Gwozdek, RDH, BA, MA, is Director of the Dental Hygiene Graduate & Degree Completion Programs in the Department of Periodontics and Oral Medicine at the University of Michigan School of Dentistry.
-
This study supports the NDHRA priority area, Health Promotion/Disease Prevention: Investigate how environmental factors (culture, socioeconomic status-SES, education) influence oral health behaviors.
-
This project won 1st place in the ADHA Sigma Phi Alpha Journalism Award Competition, June 2013, under the baccalaureate or degree completion candidate category. Award provided by a generous grant from Johnson & Johnson Healthcare Products, Division of McNEIL PPC, Inc.
- Copyright © 2014 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}