



Abstract
The purpose of this case report is to present the clinical impacts and outcomes of a patient who applied a non-professionally (‘do it yourself’ (DIY)) orthodontic treatment to correct a midline diastema post orthodontic relapse. The patient presented for preventative dental hygiene care with a chief complaint of pain and swelling surrounding teeth #8 and #9. The patient reported that a midline diastema appeared after she lost the orthodontic retainer and used rubber bands every night for approximately four years to close the diastema. The DIY orthodontic treatment of the maxillary central incisors caused rapid and severe bone loss, loss of function and pain for the patient. This case highlights the negative impact on periodontal health with DIY orthodontic treatment, ultimately resulting in extraction and implants to restore function and esthetics. It is important that dental and allied oral health professionals are aware of DIY orthodontic trends on social media in order to educate and counsel patients on the consequences to their oral health.
INTRODUCTION
Studies have found that maxillary diastemas are common in children.1,2 Some cases of diastemas may correct themselves as adjacent teeth erupt, while other more severe diastemas will require orthodontic intervention.2, 3 Most adults have reported that maxillary midline diastema is unappealing and others have reported that individuals with a midline diastema are perceived as less intelligent, less beautiful and of a lower social class.4, 5 Diastemas arise due to several factors and are often multifactorial in etiology. Some common factors include genetic factors, abnormal size, shape, and number of teeth, tongue muscle defects, abnormal frenum attachments, and periodontal defects.4, 6, 7 Unfortunately, even with orthodontic treatment, midline diastemas are considered unstable and 60% of the midline diastema orthodontic cases relapse.3 Another study showed that 75% had stability with a fixed retainer.8 This evidence algins with the treatment pathway of fixed retainers instead of removable retainers.8
Due to cost of orthodontic treatment, occurrence of midline diastema relapse, and esthetics effects of maxillary midline diastemas, there has been a rise in ‘do it yourself’ (DIY) orthodontics especially in recent years due to the effects of the Covid-19 pandemic and influence of social media.9,10 Individuals may not decide to elect orthodontic care due to cost and length of treatment and elect home treatments, by an outside non-dental party or by themselves using household items.9,10 Common items used for DIY orthodontics include wires, string, rubber bands, or placing glue in over the counter mouth guards. These DIY orthodontics trend can be dangerous due to lack of observation and guidance by a trained dental professional. The purpose of this case study is to discuss the use of DIY orthodontic methods utilized by a 21-year-old female who presented to the University of Minnesota, School of Dentistry (SOD) Dental Hygiene (DH) clinic for preventive care and a chief complaint of pain and swelling around teeth #8 and #9.
CASE DESCRIPTION
A 21-year-old African American female patient presented for a routine prophylaxis at the University of Minnesota SOD DH clinic. The patient was a college student who worked parttime during the school year and required time off from work to attend dental appointments. She had been a patient of the SOD since are 14 but had elected to complete her orthodontic treatment at a clinic outside of the SOD system in 2018. The patient did not disclose the rationale for a private orthodontist and there was no documentation in the electronic health record (EHR). The patient has dental insurance coverage, but has a co-pay for most treatments, and verbally expressed a concern for procedures not being covered. The medical and dental history included asthma, which was controlled with an albuterol inhaler, use of electronic cigarettes, bruxism and grinding. The frequency of electronic cigarette use was documented in the patient EHR stating that the patient used a 6.5 mL packet (2,000 puffs) containing 50 mg of nicotine salt every three days.
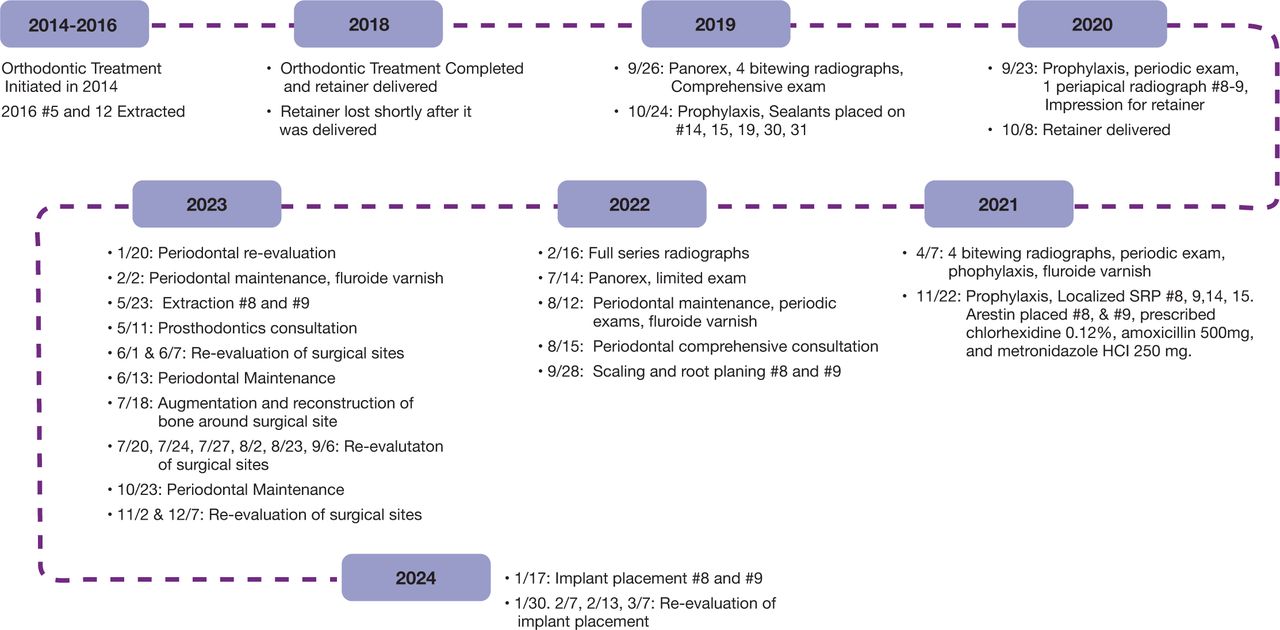
The dental care timeline is shown in Figure 1. Since this patient had been seen for many years in the SOD clinics, a complete record was available. In addition, chart notes regarding caries risk, periodontal classifications and recommendations dating back to 2015 are shown in Table I. The first EHR documentation of the patient’s pain and swelling on teeth #8 and 9 was noted at the dental hygiene recall visit in September 2020. The patient reported losing her retainer shortly after completion of orthodontic treatment and disclosed using a rubber band around teeth #8 and #9 to close her midline diastema after viewing a video on social media platforms.

Dental care timeline 2014 - 2024
Periodontal classification during dental hygiene visits 2015 - 2023
Clinical findings were a Class I mobility #8 and an erythematous fibroma on the buccal and lingual surfaces between #8 and #9. Endodontic testing for #9 was positive to percussion, palpation, and mobility. An orthodontic consultation took place during the appointment, and the patient was discouraged from using rubber bands to close the diastema; a treatment plan was made to fabricate and deliver an Essix retainer to stabilize tooth #9. It is unclear as to why this type of retainer was recommended considering the bulbous gingival tissue surrounding tooth #9. Oral hygiene recommendations included: brushing twice a day with a powered toothbrush, daily flossing, and rinsing with an antimicrobial mouthwash (ListerineÒ, Kenvue; Summit, NJ, USA) to improve home care habits; the patient agreed to these self-care goals. She returned to the SOD for impressions to initiate fabrication of a retainer for stability and reported that her teeth felt “loose.” Endodontic testing was completed again by the endodontist; no abnormal responses were noted on teeth #7-10, but teeth #8 and #9 presented with Class 1 mobility. The Essix retainer was delivered a few days later.
In April 2021, dental faculty recommended that the patient discontinue wearing the Essix retainer due to the bulbous tissue surrounding teeth #8 and #9 and transition to a Hawley retainer. In addition, a periodontal consultation referral was provided due to poor home care and advancing periodontal clinical findings. Again, oral hygiene strategies were discussed to emphasize the importance of developing good home habits to improve oral health and the self-care goals were discussed. The patient did not obtain the recommended retainer.
A periodontal consultation took place seven months later; the diagnosis included a periodontal classification of Stage III Grade C unstable, due to bleeding. The treatment plan included localized scaling and root planing (SRP) #8, 9, 14, and 15, splinting #8 and #9, occlusal adjustment to remove excursive inference, oral hygiene instruction, tobacco cessation counseling, instruction to minimize biting with anterior teeth, and counseling to stop using rubber bands to close the diastema between #8 and #9. Extraoral images were also taken to document the clinical condition. (Figure 2) After the completed treatment, the patient returned in February 2022 and reported continued smoking and pressure to use rubber bands on teeth #8 and 9. A full mouth intraoral radiographic series was taken and a referral to the periodontal clinic for additional assessments due to the rapid progression of bone loss. (Figure 3).

Clinical presentation of the patient (2021)

Periapical radiographs of tooth #9 from 2020 and 2022
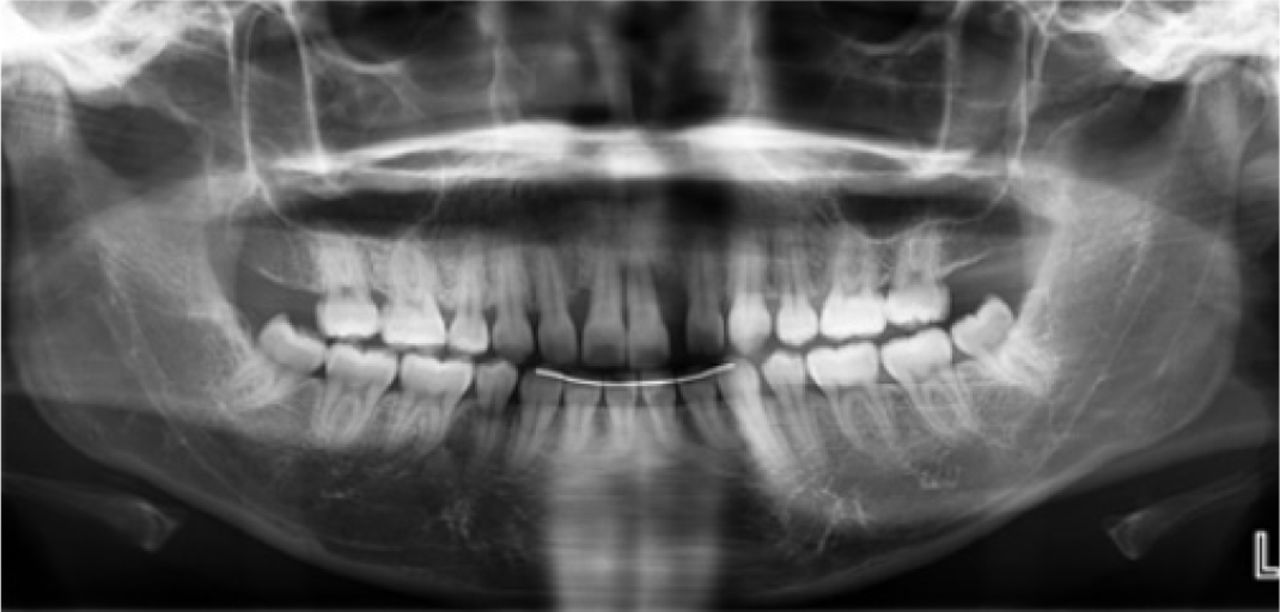
The patient presented for a periodontal maintenance in the DH clinic in July 2022 rather than an appointment in the periodontic clinic. Completed assessments in the DH clinic included intra-extra oral clinical examination, caries and periodontal risk assessments, full mouth periodontal charting, plaque index and calculus detection and diagnostic panoramic imaging (Figure 4). The patient was classified with periodontitis localized Stage IV Grade C with heavy subgingival calculus. Specific to #8 and #9, Class 3 mobility was present on #8 with exudate upon probing of the mesial-facial of #9. Localized erythematous tissue buccal and lingual of #8 and #9 with significant inflammation of the incisive papilla was documented (Figure 5). The patient was reappointed for completion of the scaling and root planning, and a periodic examination in August 2022.

Panoramic radiograph (7/14/2022)

Clinical presentation #8 and #9 lingual (7/14/2022)
Differential Diagnosis
The differential diagnoses for this case was periodontal disease considering the clinical presentation of advanced bone loss (65-80%) around #8 and #9. The three contributory factors for this periodontal case included non-compliance with a removal retainer resulting in DIY orthodontics, poor home care, lack of compliance with self-care and professional care, and tobacco use. Non-compliance of the removal retainer and the midline diastema relapse was considered to be the main influence for the patient’s elected DIY of rubber band use for #8 and #9. This was considered to be a component of the differential diagnosis, escalating the progression of bone loss.11-14 Rubber band use also added trauma to the area causing pain to the incisive papilla limiting the patient’s ability to perform adequate oral hygiene self-care. Etiological factors of periodontitis are associated with microbial dysbiotic plaque biofilm.15,16 The patient’s lack of oral self-care and longer periodontal maintenance recall intervals were considered for the increase of inflammation observed. Periodontal therapy for the removal of subgingival calculus and disruption of plaque biofilm with ultrasonic scaling and hand instrumentation has been established in the literature to reduce to be the gold standard to manage periodontitis.17-20 Oral hygiene self-care of biofilm removal is necessary for the prevention and management of periodontal disease.21,22 Additionally, tobacco use has been well established as a significant factor in the initiation, extent, and severity of periodontitis and has also been related to poorer outcomes of periodontal therapy.23
Diagnosis and Treatment
The patient presented for a periodontal consultation in September 2022. The definitive diagnosis included severe and extensive bone loss extending to the apical ⅓ of the roots on teeth #8 and 9. The periodontal recommendations included extraction of #8 and #9 and replacement with implants. Treatment sequencing included extractions to be performed as soon as possible to prevent further progression of infection and bone loss, guided bone regeneration with the possible need of a connective tissue graft (CTG), followed by dental implants.
Extractions of #8 and #9 and a CTG were completed in April 2023. Endodontic assessment was also performed on teeth #7 and #10; both teeth were determined to be vital with a good prognosis. During the extraction of tooth #9, it was determined that there was a residual rubber band affixed to the apical one-third of tooth #9; significant granulation tissue was present surrounding the rubber band. Post- surgical instructions included the use of acetaminophen and ibuprofen regimen for pain management, chlorhexidine rinse and amoxicillin for microbial control.
The patient next presented for a DH care appointment in April 2024. The health history update included that the patient stopped smoking electronic cigarettes as of February 2023. Additionally, sequencing of the dental hygiene care plan was confirmed with the periodontal clinic and following a consultation regarding the presence of significant granulation of tissue present under the buccal flap adjacent to the extraction sites and in mesial gingival tissues adjacent to #7 and #10. It was determined to continue to allow the patient to heal prior to their next re-evaluation appointment for implant placement.
The expected outcomes of treatment include slowing the progression of bone loss and periodontal infection in the affected area and restoring the function, esthetics, and occlusion of the maxillary central incisors. Risks include sinus damage, infections, damage to adjacent teeth, as well as failure of osseointegration.22 Outcomes of successful treatment also include pain relief that should help promote the patient’s ability to perform effective home care in the maxillary anterior region. Using appropriate education strategies regarding home care and the risks of DIY orthodontic treatment, along with developing patient-provider rapport, the patient and provider can work collaboratively to maintain the periodontal stability.
DISCUSSION
This unique patient case highlighted the combination of non-compliance with a removable retainer, poor oral self-care, and periodontitis; with confounding factors of financial barriers, oral health literacy, social media trends, and lack of multidisciplinary care to determine how best to treat this periodontally involved patient. The financial barriers expressed by the patient impacted the ability to consent to the proposed treatment plan and scheduling a follow-up appointment when the orthodontic retainers were lost. This case demonstrates the impact of low health literacy, and the lasting negative outcomes of the dangerous trends and misinformation shared on social media platforms. Social media influencers have promoted performing DIY orthodontic treatment on themselves, but also encouraging viewers of their social platforms that this DIY strategy could work for them as well.17 A recent study reported that 43% of orthodontic videos were posted by non-dental professionals (“laypersons”) and 38% were from DIY companies.25 This misinformation outpaced the 16% of educational videos posted by dentists or orthodontists.25 Having access to consult with properly trained dental professionals is essential in order to promote evidence-based care and products, and provide the necessary information to make decisions about their oral health. This case demonstrates the multifaceted complexity of financial barriers, low health literacy, and vulnerable populations influenced by misinformation on social media platforms. The combination of effective communication strategies to share evidence-based information, provide education, tobacco cessation and collaborative support from multiple dental providers during the extensive treatment plan was required.
CONCLUSION
This case report highlights a patient’s desire to close a diastema between teeth #8 and #9 to maintain esthetics after losing her orthodontic retainer and experiencing relapse of a midline diastema. The patient reported barriers to obtaining a new retainer and discovered a DIY option to move teeth. Social media played a significant role in promoting DIY orthodontics using rubber bands. Although a seemingly simple remedy, this practice led to exacerbated periodontal disease, pain, loss of function due to tooth movement, subgingival retention of a rubber band, extraction of #8 and #9 and the placement of dental implants to restore function. This case demonstrated the potential poor outcomes patients can experience with DIY orthodontics and the significant impact of misinformation that social media can play on vulnerable patient populations. It is important for oral health professionals to be aware of DIY orthodontic trends on social media in order to educate and counsel patients on their consequences.
IMPLICATIONS FOR DENTAL HYGIENE PRACTICE
This case study highlights the impact of a DIY orthodontic treatment and increased patient risk factors resulting in tooth loss in a young adult.
Social media trends that promote unregulated DIY orthodontic treatment to improve esthetics are dangerous to the public.
Dramatic or sudden changes in oral health status may indicate a greater underlying condition, habit, or disease progression.
Footnotes
NDHRA priority area, Client level: Basic science (dental hygiene diagnosis).
DISCLOSURES
The authors have no conflicts of interest to disclose.
- Received July 23, 2024.
- Accepted November 10, 2024.
- Copyright © 2025 The American Dental Hygienists’ Association
This article is open access and may not be copied, distributed or modified without written permission from the American Dental Hygienists’ Association.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}