



Abstract
Purpose: Health care and dental providers must be prepared to address the oral health needs of mothers and children in order to reduce the burden of dental disease in these populations. The purpose of this study was to describe the curriculum and clinical experiences related to prenatal and pediatric oral health in the university and community college dental hygiene programs in the United States (US).
Methods: Dental hygiene program directors (PDs) from across the US were invited to participate in a cross-sectional electronic survey regarding the prenatal and pediatric oral health curriculum at their institution. In addition to program characteristics, the survey included items pertaining to curriculum and competencies, content delivery methods and hours spent, locations for clinical experiences, collaboration efforts, and professional policy guidelines. Responses were summarized, and descriptive analyses were conducted to examine program competency and curriculum by program type.
Results: A total of 124 PDs responded to the survey for a 37.9% response rate; over half (54%) were based in community colleges. Overall, most PDs indicated prenatal (77.3%) and pediatric oral health (66.1%) as a part of their program’s core curriculum. However, prenatal oral health was a core competency for 52% of the respondents and less than half (46%) considered pediatric oral health a core competency. Most programs (>75%) reported teaching professional policies and guidelines. Universities reported more hours for prenatal and didactic and clinical experiences than community colleges. The most common barrier reported for prenatal and pediatric clinical experience was the lack of patients (55% and 35%, respectively).
Conclusions: Most dental hygiene programs are utilizing a variety of methodologies to incorporate prenatal and pediatric content into the curriculum and students are being exposed to professional guidelines and recommendations for these populations. However, patient care experiences for prenatal and pediatric patients were low due to lack of patients.
Introduction
Providing oral health educational and clinical guidance to women during the prenatal period is essential for promoting positive maternal and infant oral health outcomes. Prenatal oral health is an integral part of women’s health and affects the health status of their child. Children whose mothers had untreated dental caries, or tooth loss were three times more likely to have a dental caries experience compared to their counterparts.1 Dental caries, gingivitis, and periodontitis are common diseases women may encounter during pregnancy.2 Roughly 60-75% of pregnant women experience some form of periodontal disease.3 If untreated, these diseases may put both the mother and newborn at risk for preterm birth and low-birth weight.4
Preventive oral care is safe and recommended throughout all trimesters of pregnancy.5 However, using data from the state of Virginia, researchers found that less than half of the expectant mothers utilized dental care during pregnancy.6 Similarly, although it is recommended that children have their first dental visit by age one, the proportion of children aged 0-4 years, regardless of insurance type (i.e., Medicaid/CHIP or public) who receive a dental visit, is lower as compared to children aged 5-18 years.7 To minimize dental problems such as early childhood caries (ECC), a common chronic oral disease among children,8 health care and dental providers must address the oral health needs of mothers and children. In 2015-2016, 21.4% of children aged 2-5 years had a dental caries experience and 8.8% of those children had untreated tooth decay.9 Dental hygienists are ideal providers to promote oral health through education and the provision of preventive services to prenatal and pediatric patients.10 Moreover, dental hygienists can increase access to care among these vulnerable groups by providing care in health care settings such as hospitals, medical offices, and public health clinics. Currently, 39 states allow dental hygienist to work in these medical settings.11 While the dental hygiene workforce is expanding beyond the traditional private practice settings, studies have shown that dental hygienists report requesting more continuing education courses focusing on prenatal12 and infant and toddler oral health13 and early childhood caries14 as well as recommending more didactic and clinical experiences in the dental hygiene curricula.13
Dental hygienists must be prepared in their formal education and training with didactic and clinical experiences to demonstrate competence in providing care to diverse patient populations at all levels of development. Specifically, the Commission on Dental Accreditation (CODA) Standards for Allied Dental Education, standard 2-12 states, “Graduates must be competent in providing dental hygiene care for the child, adolescent, adult, geriatric, and special needs patient populations.”15 However, providing care specifically to prenatal patients is not clearly defined within the standard description.
Given the broad scope of the dental hygiene standards, each dental hygiene program may provide varying levels and number of prenatal and pediatric clinical experiences for students. Schroth et al. found that Canadian dental hygiene programs reported an average of 3.5 hours devoted to prenatal oral health and an average of 5.5 hours was allocated to infant and toddler oral health within in the curriculum.16 Previous studies have suggested a closer examination of current dental hygiene curricula and CODA standards to ensure graduates have the necessary skillsets to provide care in diverse patient care settings.17-18 There is a gap in the literature regarding prenatal and pediatric oral health education among dental hygiene programs in the US. The purpose of this study was to describe the curriculum and clinical experiences related to prenatal and pediatric oral health and to determine differences by the type of dental hygiene program.
Methods
A cross-sectional survey was used to explore and describe prenatal and pediatric (infants and toddlers) oral health curriculum and clinical experiences among U.S. dental hygiene programs. A contact list of the 332 entry-level dental hygiene (DH) program directors (PDs) was obtained, and the email addresses were confirmed from the institution’s webpage. Programs were excluded (n=5) if the contact person could not be identified, required a separate IRB to participate, or if the program was inactive. An anonymous electronic survey link (Qualtrics; Provo, UT, USA) was sent to a final sample of 327 DH program directors with four weekly reminder emails from September – October 2018.
Survey Instrument and variables
The survey questions were adapted with permission from a previous study that examined prenatal, infant and toddler oral health curriculum among Canadian dental and dental hygiene programs.16 The survey included content related to prenatal and infant and toddler oral health in the following areas: curriculum and competencies, curriculum hours and methods for delivery, locations for clinical experiences, collaboration efforts, and professional policy guidelines. In addition to above listed topics, the survey also included questions about program characteristics (community college, technical college, university DH program without dental school, and university DH program with dental school), number of full-time faculty members, number of students accepted into the entering class each year, and the number of entering classes accepted within a 12 month period, clinical experiences with performing pediatric oral health assessments (OHAs) and applying fluoride varnish, settings for OHAs and fluoride varnish applications, and interprofessional pediatric service-learning experiences. The final survey consisted of 41 items that were examined for content and face validity as well as reliability by an expert panel of dental hygiene educators. The Human Subjects Committee at Old Dominion University deemed this study as exempt.
Data Analysis
The PDs’ report of prenatal and pediatric oral health curriculum and clinical experiences for their students were examined by program type: community colleges (CC) (community and technical colleges) and universities (university/college without a dental school and university with a dental school). Descriptive analyses were conducted for summarizing sample characteristics. Chi-square, Fisher Exact, and Likelihood Ratio were used to test differences between categorical variables. Mann-Whitney U t-tests were used to examine differences in continuous variables (i.e., hours of didactic and clinical experiences related to prenatal and pediatric curriculum content between the two program types). All analyses were conducted using a statistical software program (SPSS v.26; IBM, Armonk, NY, USA) and the alpha was set at 0.05.
Results
A total of 124 PDs responded to the survey for a response rate of 37.9%. Over half of the respondents, were affiliated with a community college (54%, n=67) and most (72.8%, n=83) reported having 1-5 faculty members within the program. A majority (82.3%, n=93) accepted one DH class per year, with 42.9% (n=48) reporting a class size of 21-30 students (Table I).
Dental hygiene program characteristics (n=124)
Prenatal Oral Health Curriculum and Experiences
Over three-fourths (77.3%) of respondents indicated prenatal oral health as a part of their program’s core curriculum while just about half (51.6%) reported it as a core competency. For specific professional policies and clinical guidelines relating to prenatal oral health taught, nearly all respondents (90.5%) reported discussing the relationship between periodontal disease and preterm birth and low-birth weight. When asked whether the curriculum included information on the role of maternal/prenatal nutrition on infant and toddler oral health, (86.7%) of respondents reported in the affirmative, and 89.5% reported discussing the vertical transmission of cariogenic bacteria from mother to infant. However only 22.9% of the respondents indicated that over half of their students received at least one or more hands-on experience(s) with prenatal patients (Table II). Although the curriculum and prenatal experiences varied between community colleges and universities, none of the differences were significant at p<0.05.
Prenatal oral health curriculum and experiences (n=124)*
Hours of Didactic and Clinical Experiences and Barriers
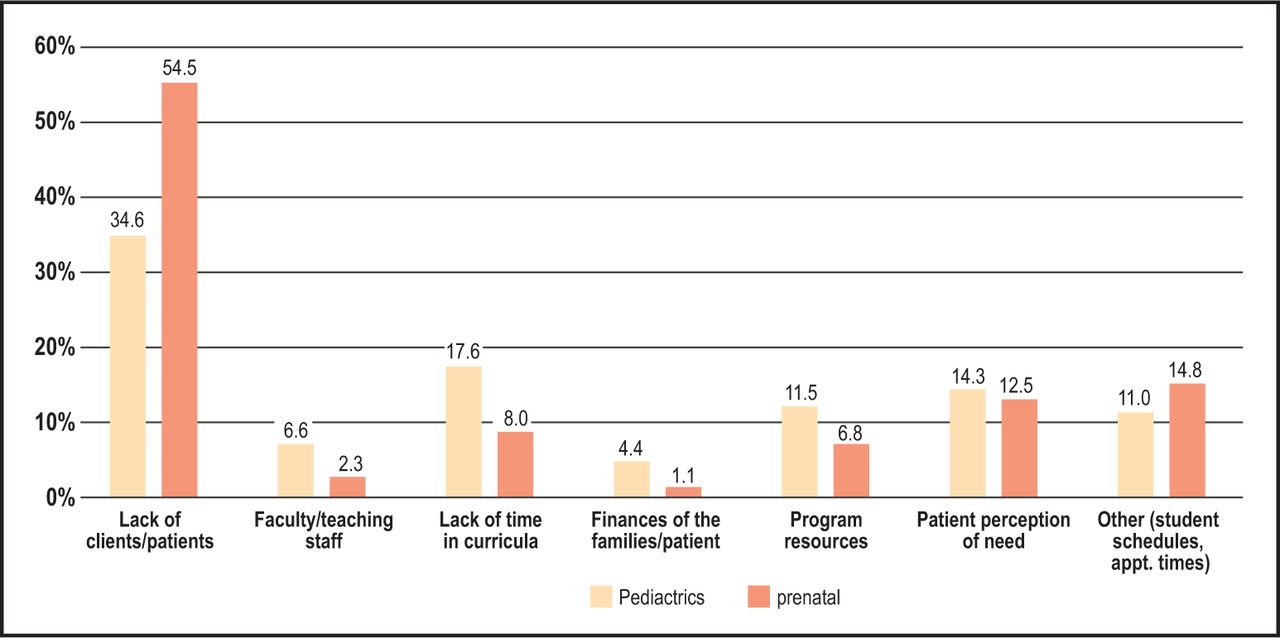
Overall, universities reported more mean hours for all forms of didactic and clinical experiences than community colleges. Specifically, respondents from universities reported the highest number of mean hours for clinical patient care experiences versus community colleges (28.93 hrs vs.5.92 hrs, respectively). However, there was wide variation among reported hours in both groups. When examining only universities, there were more mean hours reported for video or web-based learning (8.23hrs) than didactic instruction (5.80hrs) for prenatal care (Table III). The three most common reported barriers for prenatal clinical experiences included lack of clients/patients (54.5%), students’ schedules and appointment times (14.8%) and, patient perception of need (12.5%) (Figure 1).
Hours of didactic and clinical prenatal and pediatric curriculum content for all programs* (n=124)

Reported barriers to providing clinical experiences to prenatal and pediatric patients.
Pediatric Oral Health Curriculum and Experiences
Over two-thirds (66.1%) of all respondents reported having pediatric oral health as part of the DH core curriculum, while less than half (45.7%) reported pediatric oral health as a core competency. Over half of the respondents (56.8%), reported teaching the recommendation of the first dental visit by age one in their curriculum and 41.2% reported that over 75% of their students received one or more hands-on experience(s) with pediatric patients. When stratified by program type, 50% of community colleges and 60% of universities reported that more than 50% of their students received at least one hands-on experience with pediatric patients (p<0.05). When respondents were asked about students’ performance of oral health assessments (OHAs) and applying fluoride varnish, nearly 20% reported that students were lacking this experience (Table IV). In terms of collaborative efforts, only 41.4% reported that their students have interprofessional learning experiences related to pediatric oral health. Respondents from universities had higher reports of interprofessional education (IPE) opportunities (48.6%) compared to community colleges (37.7%). Of those who reported collaborative efforts, over one-quarter (28.4%) reported that these experiences occurred in public health settings such as Head Start programs (data not shown). Lastly, when asked about additional elective training opportunities related to pediatric oral health, only 1 in 5 programs reported having additional elective training opportunities (Table IV).
Pediatric oral health curriculum and experiences for all programs* (n=124)
Hours of Didactic and Clinical Experiences and Barriers
With regards to the mean hours dedicated to delivery formats of pediatric oral health content, patient care experiences were higher for university than community programs (22.2hrs vs. 7.82hrs, respectively). This was followed by clinical observation only (9.32hrs vs. 5.80hrs) and didactic approaches (6.50hrs vs. 4.11hrs) (Table III). Similar to prenatal content, there was wide variation in pediatric content hours both between and within program types. The top three reported barriers included lack of clients/patients (34.6%), lack of time in curricula (17.6%), and patient perception of need (14.3%) (Figure 1).
Professional Policies and Clinical Guidelines
In general, most respondents reported teaching various pediatric oral health professional policies and clinical guidelines within dental hygiene programs. More than 90% reported discussing the following: infant oral health care, the definition of early childhood caries, caries-risk assessment tools, amount of toothpaste to use, the relationship between bottle-feeding practices and oral health, and the recommendation for the first dental visit. Interestingly, while 91.7% of respondents reported discussing the relationship between bottle-feeding practices and oral health, only 74.1% reported discussing breast-feeding practices and oral health.
When examining differences of the professional guidelines and policies by program type, respondents from universities, had higher reports of discussing infant oral health care, amount of toothpaste use, bottle-feeding practices and oral health, and the recommendation for the first dental visit than respondents who represented community colleges, but without statistical significance (Table V).
Professional policies and clinical guidelines for prenatal and pediatrics for all programs* (n=124)
Discussion
This exploratory study provides an overview of prenatal and pediatric oral health content and clinical experiences delivery within the DH programs in the US. The following key findings were observed: respondents from both university-based and community college-based programs reported more curriculum and core competencies related to prenatal oral heath content than pediatric oral health content; the average hours dedicated to didactic and clinical experiences for both prenatal and pediatric content was higher for university than community college programs; and reports of hands-on prenatal experiences were low for both program types (universities and community colleges).
Reports of prenatal oral health curriculum content and core competency was higher than pediatric oral health content in this study. Although the prenatal population is not explicitly mentioned in CODA standards, this finding suggests that DH programs are aware of maternal oral health importance and are incorporating prenatal oral health content in their curriculum as suggested by best practice approaches.10 On the other hand, the lower report of core competencies related to pediatric oral health may be a result of the broad term “child” that is used in the CODA standard 2-12. According to the American Academy of Pediatrics, the term “child” includes all children under the age of 12 years.19 Since the standard does not specify an age range for children, DH programs may have varying definitions and requirements for child patients. This study examined the pediatric content as it relates to infants and toddlers; many DH programs have may have competencies for children aged five years and above but not for zero to five years. Perhaps a closer evaluation or clarification of the current CODA standard may be necessary to highlight the competency requirements for infants and toddlers and to ensure that students are competent and confident to deliver DH care throughout the life span.
In general, the average number of hours reported for the delivery of prenatal and pediatric didactic content and clinical experiences was higher among universities. This difference may be attributed to resource availability and connectedness with other allied health programs. For example, dental hygiene programs that are affiliated with a university and particularly a dental school, may have more opportunities for intraprofessional and interprofessional collaborations; as well as the ability to provide innovative methods of delivery and clinical experiences. For example, the University of North Carolina Chapel Hill developed a Prenatal Oral Health Program (pOHP) to provide prenatal oral health training for pediatric dentists and obstetricians and gynecologists.20 The program later evolved and included senior dental hygiene students who worked collaboratively with dental students to provide preventive services to pregnant patients.20 The researchers observed an overall increase in dental hygiene students’ knowledge and confidence to screen and counsel pregnant patients after completion of the pOHP.20 Similarly, Claiborne et al., created a service-learning experience for dental hygiene and nurse practitioner students to collaborate and deliver oral health education, oral screenings, and fluoride varnish application to pre-school age children attending a university-based child development program.21 The activity provided a space for both dental hygiene and nurse practitioner students to visualize their roles individually and collectively as it relates to pediatric oral health.
While there are documented collaborative efforts to provide prenatal and pediatric experiential clinical experiences;20-21 the current study found that the reported percentage of students with one or more hands-on experiences for prenatal and pediatric patients was low for both university and community college programs. Prenatal hands-on experiences were the lowest for both program types. This finding aligns with the respondents’ reported barriers for prenatal clinical experiences; the highest reported barrier was a lack of clients/patients. This may be related with lower use of dental services among pregnant women. There are oral health knowledge gaps and many women do not feel that it is safe to receive routine dental care during pregnancy.22,23 Dental hygiene programs are in an ideal position to offer education and routine dental care to pregnant patients while also providing students with impactful clinical experiences. To increase prenatal patient experiences, DH programs can consider partnering with public health clinics or the Women Infant and Children (WIC) programs and create experiential learning opportunities for their students.
Regarding pediatric experiences, one in five respondents reported that their students did not have experience performing oral health assessments (OHAs) and applying fluoride varnish. In addition, fewer than half reported IPE experiences. These experiences are essential for DH students as fluoride varnish is a common preventive dental service that DHs can provide and one that is often provided in settings outside of dentistry.24 Interprofessional experiences can expose dental hygiene students to other allied health professionals.17-18 One weakness identified in the dental hygiene curriculum is the minimum number of IPE opportunities reported in the entry-level curricula.17,25 Despite programmatic barriers to providing IPE experiences, dental hygiene programs are attempting to collaborate with other disciplines such as nursing to provide opportunities for students,26 which is an ideal collaborator profession to address prenatal and pediatric oral health.
This study had limitations. First, this was a cross-sectional design; and is subject to recall and reporting bias. Program directors had to recall information about the entire program curriculum related to prenatal and pediatric oral health; specifically, they had to approximate number of hours for different methods of delivery for both prenatal and pediatric didactic and clinical experiences. The hours reported may be the total hours dedicated in the curriculum but may not be reflective of all students receiving the experience (i.e., clinical related experiences), which is evident in the responses related to hands-on clinical experiences. Despite these limitations, this was the first study to the researchers’ knowledge to examine prenatal and pediatric oral health curriculum and clinical experiences within entry-level dental hygiene programs in the US. In addition, findings from the current study identifies the gaps in DH curriculum that should be addressed and improved upon while also highlighting the content areas where DH programs are successfully incorporating required content.
Conclusions
Although, DH programs vary in content and clinical experiences, it is evident that most programs are utilizing different methodologies to incorporate prenatal and pediatric content into the curriculum. In addition, DH students are being exposed to prenatal and pediatric oral health professional guidelines and recommendations. However, patient care experiences for prenatal and pediatric patients among both universities and community college programs are low due to several reported barriers, including a lack of patients. To develop a well-trained DH workforce, it is essential to identify opportunities to strengthen the prenatal and pediatric content and provide clinical experiences to the students. Integrating IPE opportunities and identifying health care professional collaborators providing care to prenatal and pediatric populations may be some strategies to increase patient encounters for DH students and better prepare them for addressing oral health among these populations.
Footnotes
This manuscript study supports the NDHRA priority area, Professional development: Education (evaluation).
- Received May 12, 2021.
- Accepted September 29, 2021.
- Copyright © 2022 The American Dental Hygienists’ Association





{kind=link}