



Abstract
Purpose: Research has shown an increase in dental hygiene (DH) students’ knowledge and attitudes toward teledentistry (TD) after TD training in states with permissive but not restrictive DH scope of practice policies. The purpose of this study was to identify self-reported knowledge and attitudes regarding TD among the DH students at the University of North Carolina (UNC) at Chapel Hill before and after an educational intervention and student recommendations for TD curriculum placement.
Methods: A faculty presentation and video demonstration, followed by small group discussions and a large group debriefing session were conducted at the UNC Adams School of Dentistry in March 2019. Participants were invited to complete a survey before and after the educational session. McNemar’s matched pair test was used to compare the proportion of the participants’ pre- and post-test responses.
Results: Survey participants (n=30) included first year and second year DH students. There was significant difference (p<0.001) between pre and post self-reported knowledge of TD as well as a significant difference in participant’s response (p= 0.012) about facilitating consultation with health care specialists through TD in NC. There was a significant difference in favorable responses (p=0.0394) that TD could increase reimbursement to dentists to enhance the provision of more services in NC. Students identified didactic courses (43%), simulated cases (47%), and integration into the DH community rotations (66%) as potential ways to incorporate TD into curriculum. Most students (93%) identified DH restricted scope of practice as a barrier to TD implementation in NC.
Conclusion: The educational session resulted in increased self-reported knowledge and demonstrated positive attitudes toward the adoption of TD into multiple facets of DH curriculum. A major barrier to its adoption into practice is the DH restricted scope of practice in NC.
Introduction
Teledentistry (TD) is the use of technology to communicate health information, provide oral health care services, screen, and educate remotely between oral health care providers and patients.1 This dental care delivery system was derived from a larger movement using telehealth technologies in the field of medicine.1 Historical developments in TD have led to multiple modalities of care including synchronous video conferencing between patient and provider using audiovisual aids, asynchronous store-and-forwarding of collected data to the provider, remote patient monitoring (RPM) of continually collected health data, and information gathered through mobile devices, or mobile health (mHealth).2
The United States Department of Health and Human Services highlights that vast oral health disparities exist across the nation, pointing to the need for development of new approaches to dental treatment that address access to care barriers among populations.3 Consequently, TD has demonstrated its usefulness in answering this national call by significantly impacting the way oral health care is delivered to disadvantaged populations such as children, prisoners, the elderly and those with intellectual and developmental disabilities who have limited access to traditional dental care.4-6 There are many examples of dental professionals that have successfully utilized TD to deliver patient care including those in oral medicine, oral and maxillofacial surgery, orthodontics, prosthodontics, endodontics, periodontics, pediatric dentistry, and general dentistry, including allied dental professionals.7,8 There is also noted evidence of TD being cost-effective due to decreased travel expenses for patients, increased patient care for providers and overall reduced cost of dental neglect through educational and preventive services.8,9 The validity of TD has been demonstrated through studies covering pediatrics, general dentistry, radiology, endodontics and orthodontics where diagnoses were consistent between TD and in-person visual examinations.10 While all states and Washington D.C. reimburse providers for at least some form of telemedicine services, only eight states were reimbursing for TD services as of 2019.11,12 (Note: this does not include COVID-19 policy changes because most are temporary during the declared national state of emergency.) The American Dental Association (ADA) released the first two Current Dental Terminology (CDT) codes addressing TD services in 2017. The availability of these codes may motivate further commercial and government reimbursement for care and services provided through TD.2
Teledentistry also holds merit in the formal education of dental professionals at multiple levels of study including entry-level and undergraduate dental hygiene (DH), Doctor of Dental Surgery (DDS), and Doctor of Dental Medicine (DMD) and graduate students.13-16 However, schools that are currently using TD to train students to meet oral health care needs are located in states (Nebraska, California, Minnesota, and Arizona) that have more permissive policy (accommodating use of TD) regarding scope of practice for dental hygienists and Medicaid reimbursement. Permissive scope of practice allows for expanded functions, general supervision or independent practice protocols, or a DH diagnosis. North Carolina (NC) has a more restrictive climate regarding these same policy matters. For example, NC law does now allow for expanded DH functions and requires most DHs to practice under direct supervision, with general supervision newly granted in 2020 to those who meet strict qualifications.17,18 The direct supervision regulation does not allow for DHs to use asynchronous TD in a community setting to perform preventive services and have the DDS conduct a remote examination. Therefore, if DHs cannot practice utilizing TD in this manner, they will not experience how to practice with TD during their clinical education. Another example is that in some states, DHs are not permitted to administer local anesthesia. They may learn about pain control methods and theory as part of their education, but do not actually administer local anesthesia as a part of the curriculum.
Some studies have shown an increase in knowledge and attitudes of DDS and DH students after TD training in these more permissive states, however there is little evidence of TD training or resulting increased knowledge or attitude changes in policy restrictive states such as NC. Therefore, the purpose of this study is to fill this gap by identifying the knowledge and attitudes of TD among the DH student population at the University of North Carolina (UNC) at Chapel Hill. A key emphasis was placed on understanding students’ perspectives on how TD should be adopted and included into their curriculum.
Methods
Overview
This study (#19-0242) was conducted at UNC Chapel Hill (UNC-CH) was considered exempt by the UNC-CH Institutional Review Board (IRB). A longitudinal mixed methods study was used and incorporated a survey (Qualtrics; Provo, UT, USA), small group discussions, and a large group debriefing session. The intervention consisted of a video of a faculty presentation and synchronous TD demonstration, small group discussions and a large group debriefing session. The data collection process included a pre- and post-intervention survey, and notes from the large group debriefing session. The study population included students enrolled in the first or second year of the DH program at the UNC Adams School of Dentistry (ASoD). Students who did not complete both the pre- and post-intervention surveys or failed to attend the intervention were excluded from analysis.
Intervention
The intervention was a pre-recorded lecture by the Director of Teledentistry at UNC ASoD, Dr. Shaun Matthews. The lecture defined TD and related terms, discussed models of delivery, access to care statistics in NC, and laws governing TD events. The role of DHs using TD while working under general supervision, was emphasized with the example of the evidenced-based, California Virtual Dental Home model8 and was contrasted with the NC practice act requirement of direct supervision of DHs. A recorded, synchronous, post-operative consultation between a provider and patient was played, and Medicaid reimbursement for TD services was reviewed. Examples of TD’s potential use in in the DH curriculum were also presented.
Survey instrument
Survey questions were developed from previously completed studies regarding TD, access to oral health care, and pre-licensure curriculum.15,16,19 Permission was received from Northern Arizona University to use part of their survey regarding the value of TD in the DH curriculum.16 All of the surveys had been pilot tested previously, adding to the validity of this study. Pilot testing for both pre- and post-intervention surveys was completed by three DH students who were not attending the TD educational session. Minor modifications were made based on their feedback.
The 19-item pre-intervention survey included three demographic questions (i.e. age range, gender, program year) and one clinical experience question. There was one question each about DH’s current TD knowledge, use of TD, and TD governing policies, two questions about adoption of TD into the DH curriculum, and ten questions regarding how TD can improve access to oral health care. Further, there were two questions whether TD should be adopted into DH curriculum. In addition to the pre-survey questions, the post-intervention survey included two items addressing how TD should be implemented into curriculum, one question each regarding barriers to curriculum implementation, and expected utilization of TD upon entering DH practice after graduation for a total of 23 questions. The curriculum methodology and post-graduation practice questions were limited to the post-survey because it was felt students would not have enough knowledge of TD to provide a response in the pre-survey. All items used either yes/no/I don’t know categories or Likert Scales. Likert scales were used to assess knowledge (1= no knowledge to 5= very knowledgeable), attitude (1= not at all to 5= a great deal), and curriculum (1= poor to 5= excellent). Additionally, the pre- and post-surveys included four coding items with one letter or number answers to create a personal identification known only to the participant, which were used by the researcher to do a matched paired analysis of pre-and post-intervention answers.
Implementation
Students were recruited through email and paper flyers advertising the TD program and participants were asked to sign-up prior to the presentation. The intervention took place in two separate sessions, one for first year and another for second year DH classes. Two hours were allotted for each session. The sessions began with obtaining informed consent followed by the administration of the voluntary digital survey to assess their self-reported knowledge and attitudes about TD prior to the intervention. The survey link and QR code were displayed via a projector for ease of access via smartphone or computer. All consenting participants watched a forty-minute pre-recorded presentation about TD, followed by a ten-minute question and answer session where the facilitator (CM) answered all questions asked by the students. Participants were divided into small groups of 3-6 students. Each small group, guided by the facilitator (CM), discussed the following questions for thirty minutes. 1) Do you think TD has or does not have the potential to help alleviate the oral health crisis in North Carolina? Why or why not? 2) What and how would you like to learn about TD while in school? 3.) Identify challenges and potential solutions to implement TD in DH curriculum.
All participants reconvened as one group to share their answers to the same questions in an open forum debrief, guided by the facilitator, for thirty minutes. A non-participant student notetaker recorded the main discussion themes. At the conclusion of the session, participants completed the post intervention survey.
Data Analysis
All participants included in the analyses were matched for pre-post survey responses using unique identification characteristics. Data from the matched pair responses were used for statistical analyses. The demographic variables were tabulated and summarized. Categorical variables with 5 Likert-scale response options were dichotomized with categories 1-2 combined as “no” and 3-5 as “yes.” “I don’t know” responses were interpreted as having negative connotation and categorized as “no”. Descriptive analyses were performed for each categorical variable and the distribution of these categories for the pre- and the post-intervention surveys were compared and reported. Due to the relatively small cell counts for each of the contingency tables, exact McNemar’s matched pair test was used to compare the proportion of the participants’ responses to the pre-post survey questions for each binary outcome. Sensitivity analyses were conducted to assess whether DH students’ responses had any differences pre-to-post intervention. The standard 5% statistical significance level was used for all statistical tests. A software program (SAS version 9.4, SAS Institute Inc.; Cary, NC, USA) was used for the statistical analysis.
Results
Seventy DH students were invited to participate while thirty students attended the session and completed the pre-and-post intervention surveys for a participation rate of 43% (n=30). The analytic pre-post survey sample included 10 first year and 20 second year DH students. The majority (77%) of study participants were between the ages of 18-24 with 23% of the sample aged 24-34 years. All of the participants (100%) identified as female, compared to 99% of the students enrolled in DH classes. Most (96%) held residency in NC.
Self-reported knowledge and attitudes
Participants’ responses regarding TD and its impact on access to care in NC following the educational intervention are shown in Table I. The proportion responding “yes” increased in all categories except one, where it remained the same. Responses regarding TD facilitating consultations with health care specialists in NC increased significantly from pre-to-post intervention (p= 0.012). There was also a significance difference in favorable responses (p=0.039) to the concept that TD could increase reimbursement to dentists and enhance the provision of more services in NC.
Pre- and post-survey perspectives on potential advantages of teledentistry (n=30)
Comparison of pre-and-post-survey responses showed a significant difference in self-reported knowledge of TD among students in the analytical sample (p<0.001) as shown in Table II. There were no significant pre-post differences (p=0.999) among students’ attitudes regarding the DHs’ role in the delivery of services through TD (Table II). Based on post-survey responses following the intervention nearly all participants “agreed” or “strongly agreed” (93%) that they gained knowledge that they could use in the future.
Response distribution for pre-and post-intervention for teledentistry knowledge, attitude and curriculum application (n=30)
Participants were asked what barrier, among six choices, needed to be addressed first in order to adopt TD into practice. A majority of students (63%) reported that the state dental practice act requiring direct supervision of DHs in NC was the first barrier to address. The second barrier, cited by 30% of participants, was the lack of TD focused continuing education.
Teledentistry curriculum
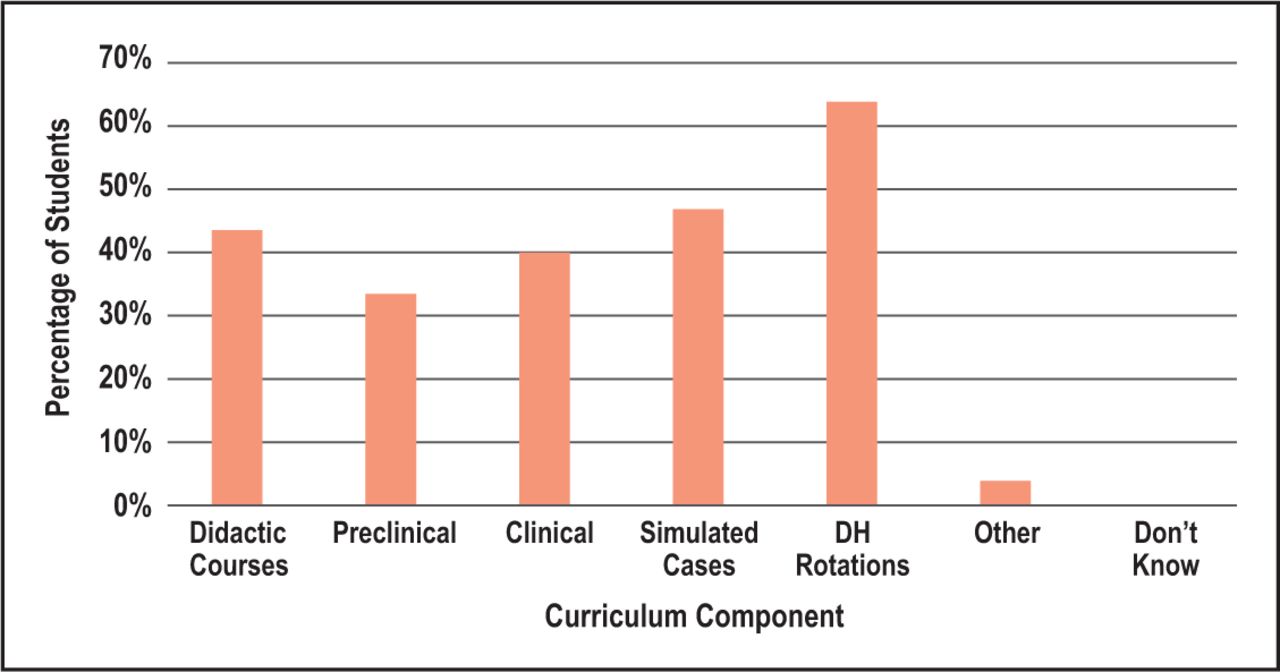
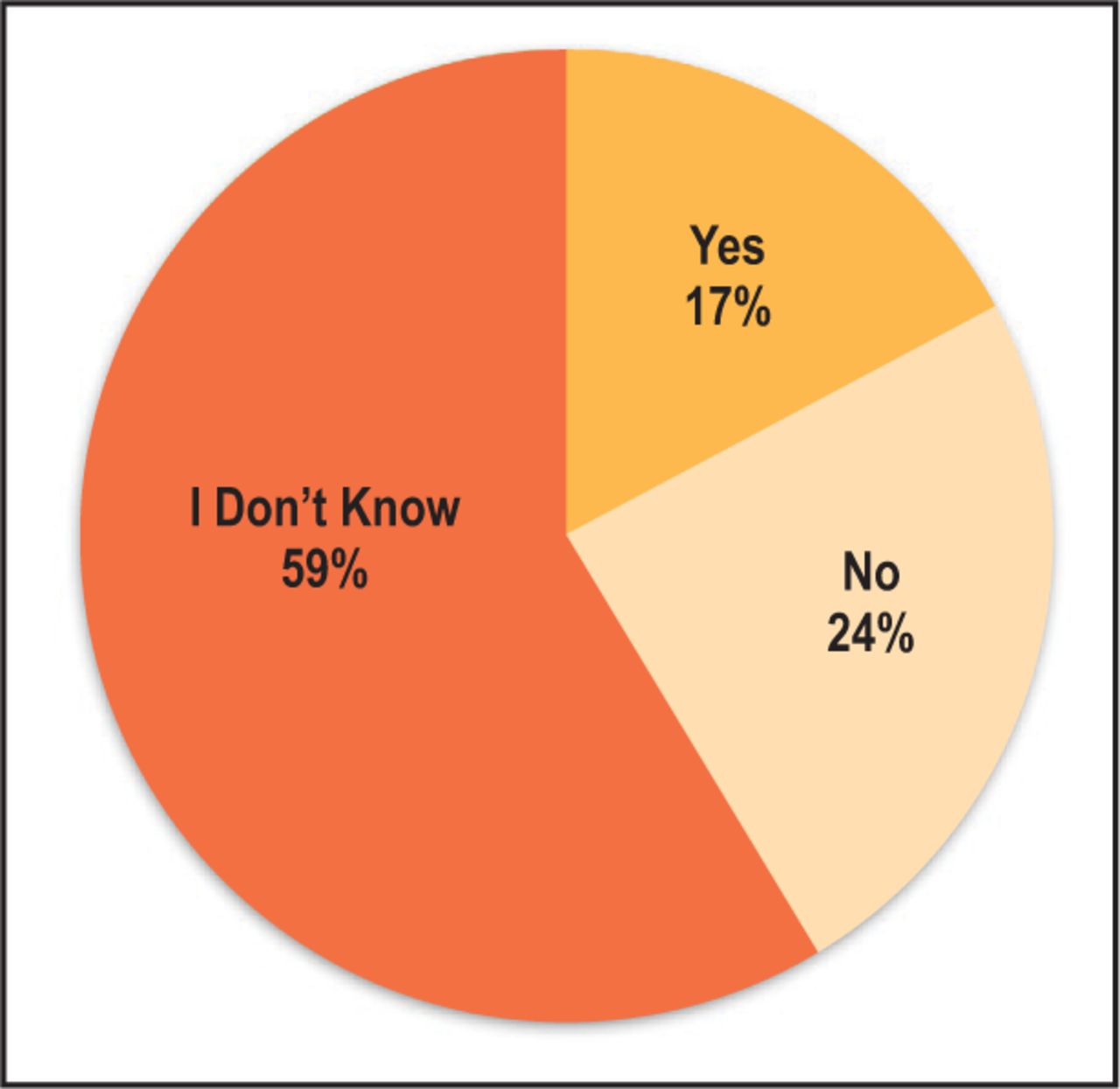
Participants’ attitudes regarding the inclusion of TD in DH curriculum were high both before and after the intervention. Prior to the intervention, 80% of students thought that there was a “good”, “very good” or “excellent” value in including TD in curriculum while 87% felt strongly following the session (Table II). No significant attitude changes regarding adopting TD into the DH curriculum (p = 0.727) were identified, likely due to the high proportion already in favor of its inclusion pre-intervention. Nearly half of the participants concluded that TD could be taught in several ways: using simulated cases, in didactic courses and clinical practice (Figure 1). Over half of the student participants thought that TD experience could be integrated into DH extramural community rotations. The DH extramural rotations include students traveling to community settings (pre-schools, elementary/middle schools, nursing homes) to provide oral hygiene education and conducting screenings for oral disease among elementary school children. Barriers to the implementation of TD into the curriculum included cost of required technology, lack of perceived instructor technical skills, lack of student interest and restricted scope of practice for DHs. It is noteworthy that the analyses showed a slight, non-significant increase in self-reported desire to implement TD in NC (p=0.726) but 57% of the respondents indicated that they were unsure if they would practice using TD as a part of patient care delivery after graduation (Figure 2).

Incorporation of teledentistry instruction in dental hygiene curriculum
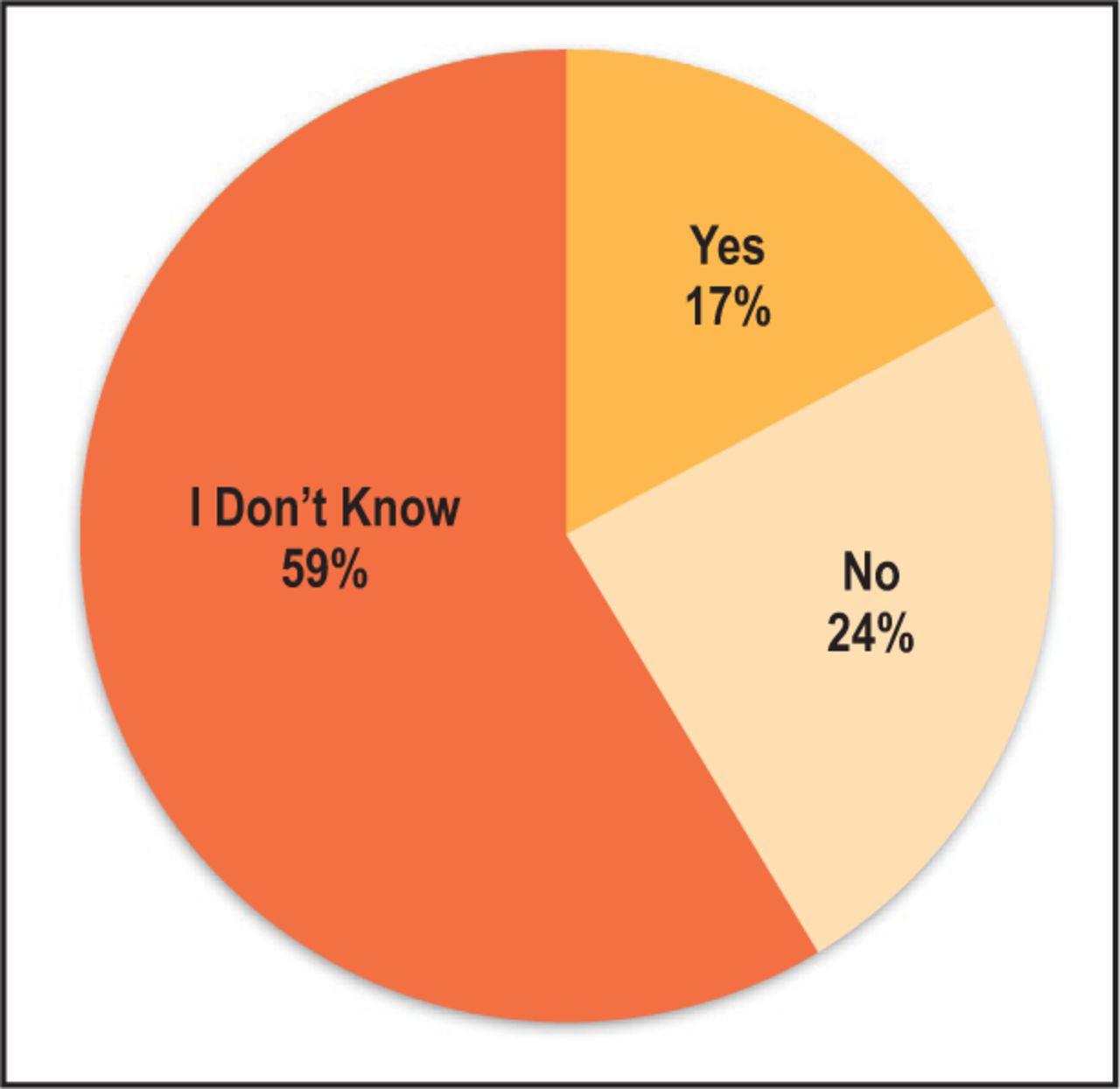
Participants’ expectation of using teledentistry for patient care after graduation (n=30)
Discussion
This study identified the self-reported knowledge and attitudes toward TD among a DH student population at UNC ASoD, where TD was not part of the DH education program and had limited adoption in the state. A key emphasis was placed on understanding students’ perspectives on how TD should be adopted into their entry-level curriculum.
Knowledge
Though there are some studies that pertain to the inclusion of TD in DDS curriculum,13,14 only a few advocate its inclusion in DH curriculum.15,16 Learning about the multiple aspects and benefits of TD led to an increase in self-reported knowledge that students could use in the future. This knowledge gain through an educational intervention is supported by another study at the University of Nebraska Medical Center.13 Third-and-fourth year dental students demonstrated knowledge gains regarding TD after completing didactic and hands-on TD training. Basic TD concepts including definition, technology, applications, scheduling, conducting consultations and record keeping were delivered through training modules.13 These same TD concepts could be included in DH education programs.
Curriculum
Overall, participants in this study were in agreement regarding the value of including TD in the DH curriculum with DH students at Northern Arizona University (NAU).16 On a scale of 1-5 (1 being poor and 5 being excellent), UNC students scored the value of TD in DH curriculum at an average of 4 (very good) while NAU students scored it at 4.3 (between very good and excellent). While minor, the difference in attitude between the two groups may be because DHs in Arizona have a less restrictive practice act and are able to utilize TD at a higher rate compared to NC.
Per current knowledge, this study was the first attempt to seek students’ opinion on why and how TD should be taught in DH curriculum. A major theme from the debrief session was that TD should be taught through didactic lectures, followed by practice with hands-on training. However, the post-intervention survey revealed that a higher proportion of participants thought that TD was more appropriately taught through didactic coursework than through most types of hands-on training (i.e. preclinical and clinical practice, simulated cases). Perhaps this difference is due to the limited use of TD following licensure in NC because of the restrictive practice act.
Most participants felt TD could be used to enhance their community rotation experiences. Currently, DH students at UNC ASoD perform caries screenings elementary schools under the supervision of a public health DH. With TD, this experience could be enhanced by using technology to take intraoral photos of carious teeth for follow-up and referral to a dentist for treatment and could be modeled after the TD-assisted, affiliated practice model created at NAU.16 This model allowed training of DH students to use TD equipment such as Nomad x-ray units, intraoral cameras, and electronic health records (for store-and-forwarding of data). Students then conducted screenings of pre-school aged children at multiple local Head Start centers and the data was sent to a contracted pediatric dentist for diagnosis and treatment planning. The project was supervised by NAU DH faculty and volunteer dentists were present. Additionally, the UNC survey found that students thought that TD could be implemented more easily in the school setting because of all the available technologies (i.e. electronic health records, computers, intraoral cameras, portable radiographic equipment, etc.).
Opportunities for dental professionals to use TD have expanded during the COVID-19 pandemic.20 At the start of the pandemic, the American Dental Association recommended that dentists postpone elective treatment and perform only emergency and urgent dental care. As NC, among other states, began to open dental offices at limited capacity, dental consultation and triage delivered through virtual means to provide consultation and triage could help patients determine if their concerns constitute true dental emergencies or if they were less urgent.21 This guidance helped prevent patients from seeking dental care at overwhelmed emergency departments and urgent care centers unless necessary.
With students in favor of incorporating TD into practice and curriculum, they can be afforded the opportunity to learn patient care skills with TD during the pandemic. Students could first be trained in how to use TD by virtual seminars with a TD expert, followed by practice with a simulated patient, then clinical patients. For example, the DH students could complete a synchronous video consultation with patients providing oral hygiene instructions, caries risk assessments, nutritional or smoking cessation counseling, while having a school faculty member virtually present. Students should also learn from TD initiatives, like the UNC ASoD virtual oral health care helpline, launched in March 2020. The helpline aimed to virtually address patients’ dental concerns to prevent patients without true dental emergencies from seeking dental care at overwhelmed emergency departments and urgent care centers.22 The exposure of oral health care professionals to TD during this pandemic will likely favor its continued use afterward. Because the pandemic environment has enabled increased provider experience with TD workflow and technology and an understanding of its ability to grant access to and improve quality of care, there will be a greater opportunity to incorporate TD into DH curriculum.
Access to Care
Generally, TD has been shown to increase access to care via consultations involving general and specialty dentists.7,14,23 Additionally, in general health care, telehealth consultations have been shown to increase access to medical specialists.24 The UNC results indicated that students think TD should be used to increase access to oral health care in NC and facilitate consultation with health care specialists. Furthermore, students concluded that access to preventive care (oral hygiene education, counseling, risk assessments, prophylaxes, and fluoride) could be expanded using TD. The majority of students also reported that TD could be used to increase efficient use of clinicians’ and patients’ time and reduce patients’ travel costs. In other studies, TD has been successful in providing cost-savings for patients’ travel expenses and provider equipment purchase, operation and time.9,25 During the debriefing session, participants emphasized the value of TD-based care to augment traditional, in person care, not as a replacement.
Barriers to Implementation
The greatest barrier to implementing TD into curriculum identified by 93% of students was the NC state DH practice act requiring direct supervision of DHs. Less than one-fourth of DH students indicated that they expected to be able to use TD after graduation and licensure. The debriefing session revealed that this attitude may prevail until the NC practice act is changed to allow for widespread general supervision. Dental hygiene students do not see the value of learning a skill they cannot use upon entering practice. A study of key NC stakeholders by Weintraub et al. also concluded that the main barrier to TD implementation in NC is the direct supervision requirement.19 Minnesota has created a supportive policy environment for DHs to practice under general supervision that has further allowed for TD integration into DH curriculum at Minnesota State University Mankato.15,26 Additionally, the Virtual Dental Home utilizes DHs in a range of community settings, under general supervision, and has made a substantial impact regarding access to care in California.8
Lack of student interest was another frequently cited barrier to the implementation of TD into curriculum. During the debriefing session, students discussed the importance of educating other students and dental faculty about the benefits of TD in providing access to care to underserved populations. Faculty development programs are of great importance to ensure that all faculty have current understanding and use of TD technology. Students also felt that TD must show a clear return on investment to be an attractive DH curriculum addition.
Limitations
This study is limited by a relatively small convenience sample size from one program in NC. The study participants were more likely interested in learning about TD than non-participants, and these factors may impact the generalizability of the findings. Further study could be conducted among dental and dental hygiene students from other programs both within NC and out of state to understand their attitudes toward TD. Additionally, evaluation of knowledge and attitudes of faculty members in is needed. Subsequent provision of TD information and training to address gaps in knowledge would help to improve delivery of TD for dental education programs in NC.
Conclusion
The educational session resulted in increases of self-reported knowledge of TD and positive attitudes that TD implementation could help alleviate access to care issues. Findings also demonstrated positive attitudes toward the adoption of TD into multiple facets of DH curriculum. Education and hands-on TD training are valuable curriculum tools in the future practice of oral health care professional students. Easing the direct supervision requirement of for dental hygienists in NC could help support the incorporation of TD into common practice and the DH curriculum.
Acknowledgments
The authors would like to acknowledge Nigel Shaun Matthews, DDS, MD, clinical associate professor at the Indiana University School of Dentistry and the former Director of Teledentistry at the University of North Carolina at Chapel Hill, Adams School of Dentistry, for his contributions to this project and for his leadership in advancing teledentistry in NC.
Footnotes
This manuscript supports the NDHRA priority area of Professional development: Education (evaluation).
- Received August 23, 2020.
- Accepted February 18, 2021.
- Copyright © 2021 The American Dental Hygienists’ Association





{kind=link}
{kind=link}