



Abstract
Purpose: The purpose of this systematic review is to identify clinical outcomes, health care utilization and costs associated with teledentistry. Relevant databases were searched for articles on teledentistry published until March 2012, reference lists examined and key journals hand searched. Of a possible 58 articles, 19 studies met the inclusion criteria.
Clinical outcomes were generally improved following a teledentistry intervention and satisfaction with teledentistry was consistently high. The few studies examining health care utilization reported mixed findings, but preliminary evidence suggests cost savings for health care facilities.
There is a consistent trend in the literature supporting the efficacy and effectiveness of teledentistry. Further research is needed to identify the effectiveness, efficiency, utilization and costs of teledentistry as it could provide the key to improving access to care.
Introduction
Teledentistry is the use of information technology and tele-communications for dental care, consultation, education and public awareness in the same manner as telehealth and telemedicine.1 Teledentistry can also be used to assist general dentists with specialty work and improve services to underserved populations with no or limited access to care.2,3 Alongside the many branches of telemedicine, the number of teledentistry programs has been steadily increasing.2
Systematic reviews help summarize and critically synthesize the available body of literature and are useful in clinical decision-making and program planning, especially in a newer research area where quality and scope of studies is variable.4 Systematic reviews also help to identify areas in which research is currently lacking.4-7 While there is a growing body of literature on teledentistry, no systematic reviews have been published.
Jennett et al conducted a systematic review of the socio-economic impact of general telehealth.8 Dentistry was one of several areas examined in a brief overview of the types of socio-economic outcomes used in the teledentistry studies and the number of studies demonstrating benefits on those outcomes. This paper provides a systematic review of the scientific literature in order to evaluate the efficacy, effectiveness and costs of teledentistry used for direct patient services, specifically clinical outcomes, health care utilization and costs related to teledentistry. These outcomes were selected to reflect a common objective of teledentistry programs - to provide access to quality services while minimizing costs.
Methods and Materials
Search Strategy
For the present study, teledentistry is defined as the use of communication and information technologies to provide clinical services from a distance. Electronic databases were searched to identify relevant articles. Searches were limited to the English language and publication date from the earliest available date for each database to March 2012. Literature searches were conducted using PubMed/Medline, EMBASE, CINAHL with Full Text, PsychINFO, EBM Reviews (e.g. Cochrane Database of Systematic Reviews, ACP Journal Club, Database of Abstracts of Reviews of Effects, Cochrane Central Register of Controlled Trials, Cochrane Methodology Register, Health Technology Assessment and NHS Economic Evaluation Database), Scopus, Education Resource Information Center (ERIC), Google Scholar and Turning Research into Practice (TRIP). The search strategies included subject headings and subheadings (if available) combined with keyword searching. The search concepts included teledentistry, telemedicine, telehealth, remote consultation, cost effectiveness, outcome, dentistry and dental services.
Selection Criteria
Studies were included if they were designed as an interventional study (experimental and observations based on judgments from teledentistry images), used quantitative or qualitative approaches, and presented findings related to outcomes or costs. There were no restrictions for age or care setting (e.g., home, community or facility).
Studies were excluded if they included only telephone interventions (unless telephone intervention was one group of the study, with a video component in the other, or unless other technologies were paired with the use of the telephone), the technology was smart home monitoring devices, examined telehome care of patients with chronic disease who received only nursing interventions with no dental care objective, reported only the development phase of the technology (i.e., feasibility of the technology in a lab setting), examined only the support for caregivers of patients, were program descriptions or reports not designed as research studies, and were redundant articles which dealt with the same intervention and did not report any new outcomes.
Studies were also excluded if they provided insufficient information to allow adequate interpretation of the study design, measures or results, or if they were only found in abstract form, in abstracts or posters from conference proceedings.
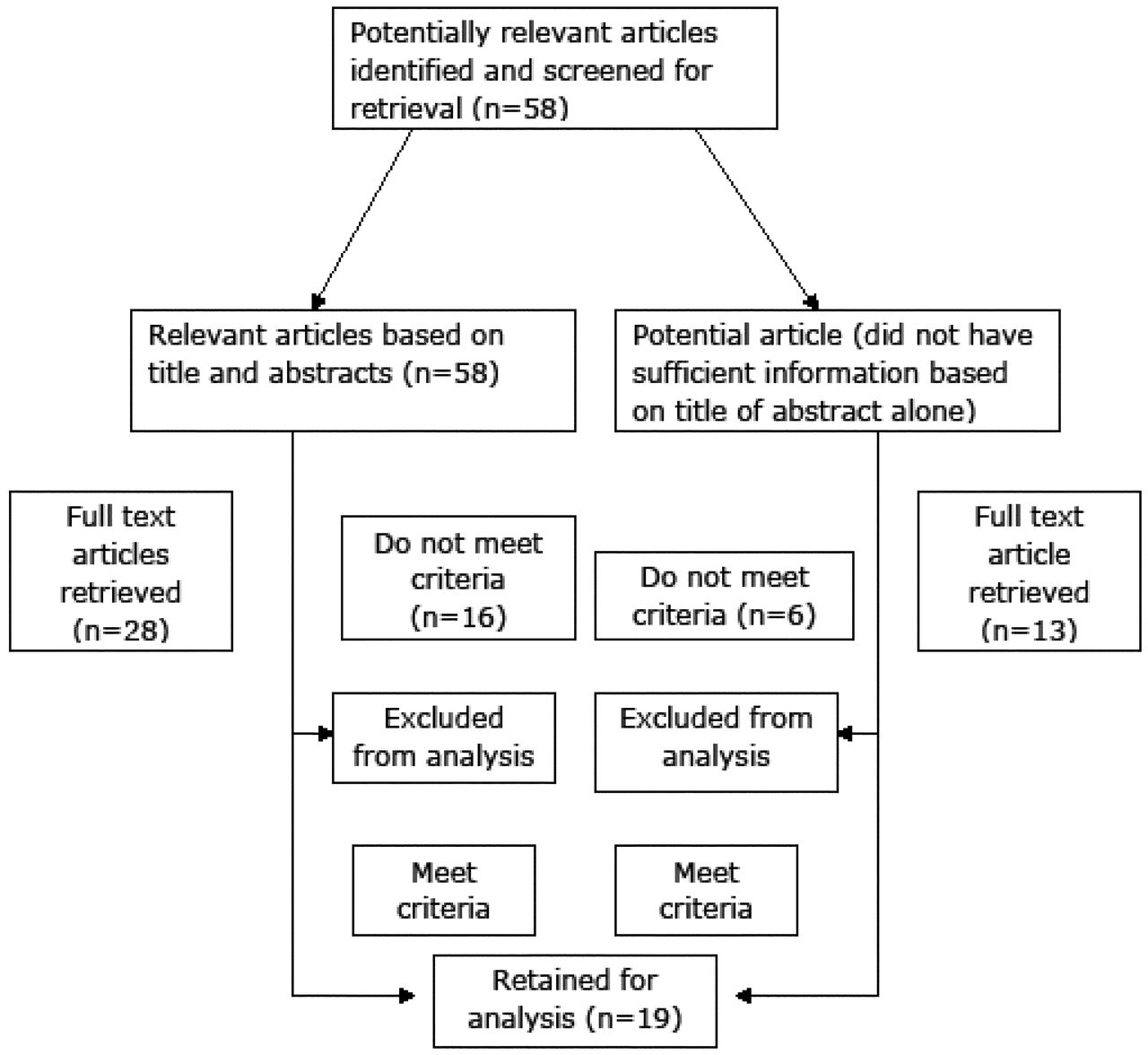
Based on the identified criteria, potential eligible articles were first determined by examining article titles and abstracts from the database searches. Full-text articles were then retrieved and evaluated for relevance. Articles were excluded at this point if they failed to meet the criteria after the full texts were examined. Figure 1 represents the flow chart of identifying relevant articles for analysis. A second researcher reviewed all articles using the same criteria for inclusion and exclusion. The 2 reviewers compared selected articles, discussed differences of opinions holding each selection to the inclusion criteria and confirming the relevance and findings from the selected articles. A total of 19 articles were retained for analysis.
Data Extraction and Outcome Measures
The articles were reviewed and a data extraction form was used to include details pertaining to the

Flow chart of identifying relevant studies for analysis
Clinical: Outcomes related to service delivery, such as attendance and adherence to programs and recommendations, as well as health care provider and staff satisfaction with the program
Health care utilization: Events that occur outside the program's scope and that the program may aim to reduce or increase, such as hospitalizations and admissions
Costs: From the perspectives of patients, providers or organizations, all costs (savings and/or expenses) associated with the use of teledentistry
Results
As Figure 1 indicates, 19 studies were retained after the initial screening of 58 titles, abstracts and the full-text retrieval of pertinent articles.9-27 The search strategy and selection criteria did not limit the type of experimental or observational design.
Clinical
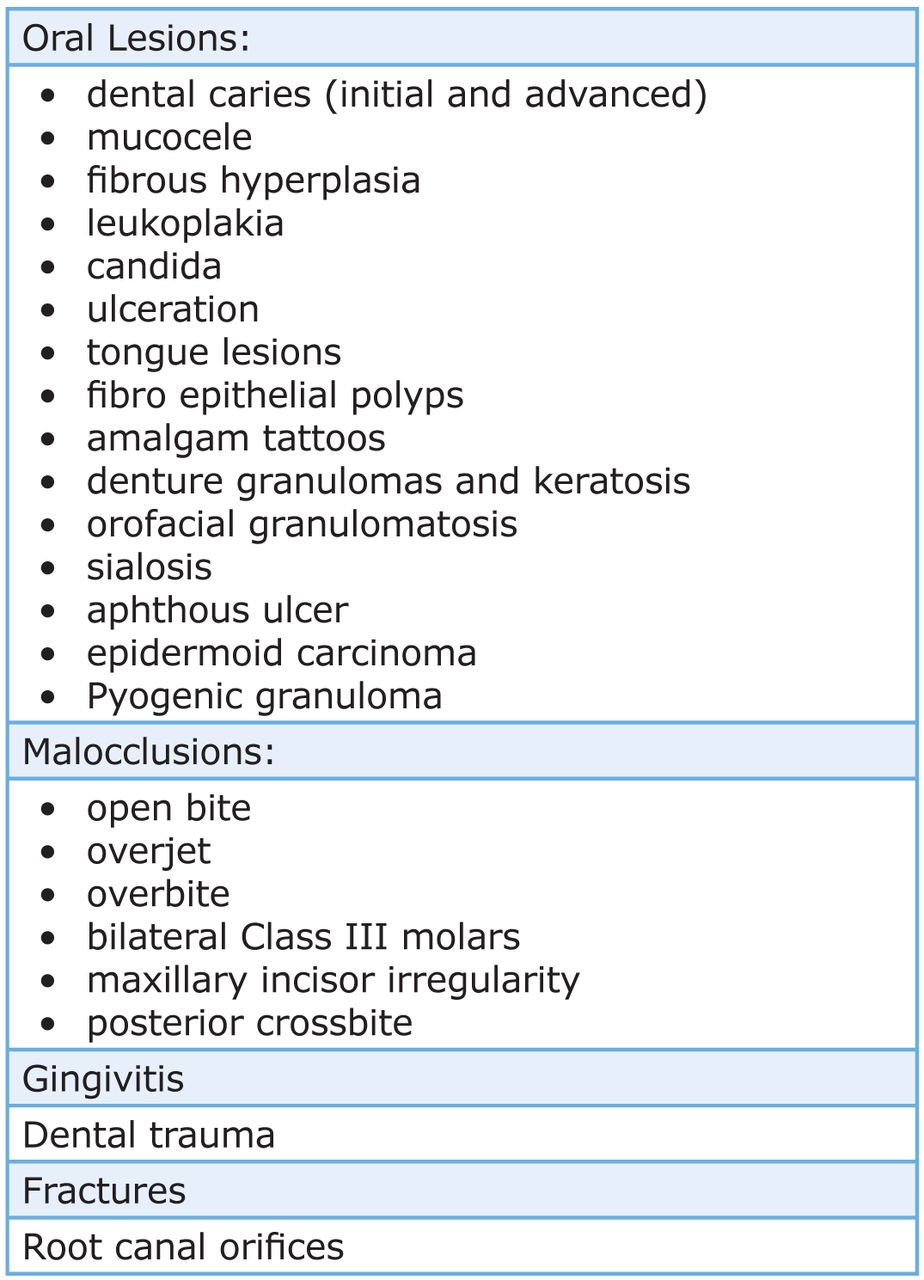
Articles of clinical outcomes focused on validity, accuracy and reliability of teledentistry in screening for dental caries, identification of oral mucosal lesions and orthodontic consults and referrals (Figure 2).
Dental Caries
Five studies comparing clinical and teledentistry screenings for dental caries examined the following: feasibility validity, reliability prevalence and inter-examiner agreement.10,17,20,22,27 Dental caries, restored teeth, missing or extracted were scored as decayed filled surfaces (DFS) deft for the primary dentition, or decayed, extracted, filled teeth (DEFT) for the permanent dentition.10,17,20,22
Clinical screening methods varied among the studies from use of a mirror only to use of a mouth mirror, light and explorer by a calibrated pediatric dentist.17,27 Not only did methods for clinical examination differ, but also the number of intraoral images captured for teledentistry screenings ranged from no specific number reported to 6 images.10,27 Cameras used to capture images and number of teeth captured in an image also varied among the 5 studies.10,17,20,22,27
Type of personnel differed among the studies. In one study, 6 telehealth assistants captured images of children in 6 Head Start centers for transmission to a dental examiner who would screen for DFS to determine prevalence of dental carries.20 In another, a registered dental hygienist and registered dental assistant performed both clinical and teledentistry screenings.10 In another study examining the validity of teledentistry screening, the clinical screening was performed by an experienced dentist using light, mirror and explorer to establish a gold standard against which the teledentistry screening by 4 dentists was measured.22
No statistical difference was found between teledentistry and clinical screening for dental caries. Sensitivity ranged from 98 to 100% . The use of teledentistry screening and clinical screenings for dental caries in young children was shown to be both cost-effective and valid.17,22 The Kappa statistic for reliability between clinical and teledentistry screenings for early childhood caries ranged from 0.58 to 0.61.10,17 Identification of primary teeth in need of restoration resulted in Kappa 0.93.10
There was no significant difference between the use of clinical and teledentistry screenings in assessing prevalence of early childhood caries.27 The mean of DFS with clinical examination was 1.40 (SD=4.07) and with teledentistry was 1.56 (SD=4.15).27
Orthodontics
Teledentistry examination to identify the need for orthodontic referral was found to be as effective as referral from clinical examinations.13 Orthodontic referral rates for teledentistry and clinical examinations were compared. Acceptance by orthodontists of children screened using teledentistry or clinical methods was also reported.13 Sensitivity for referrals using teledentistry was 80% and specificity 73%. Use of teledentistry for referrals resulted in a positive predictive value of 0.92. The negative predictive value was 0.50, which occurred due to half of the children (n=22) that would have been accepted by an orthodontist if a clinical examination had been performed. The Kappa score of 0.46 reflects moderate agreement of orthodontist acceptance of teledentistry referrals. The teledentistry group was less likely to refer an individual who did not need orthodontic care than those who made referrals based on clinical examinations.13
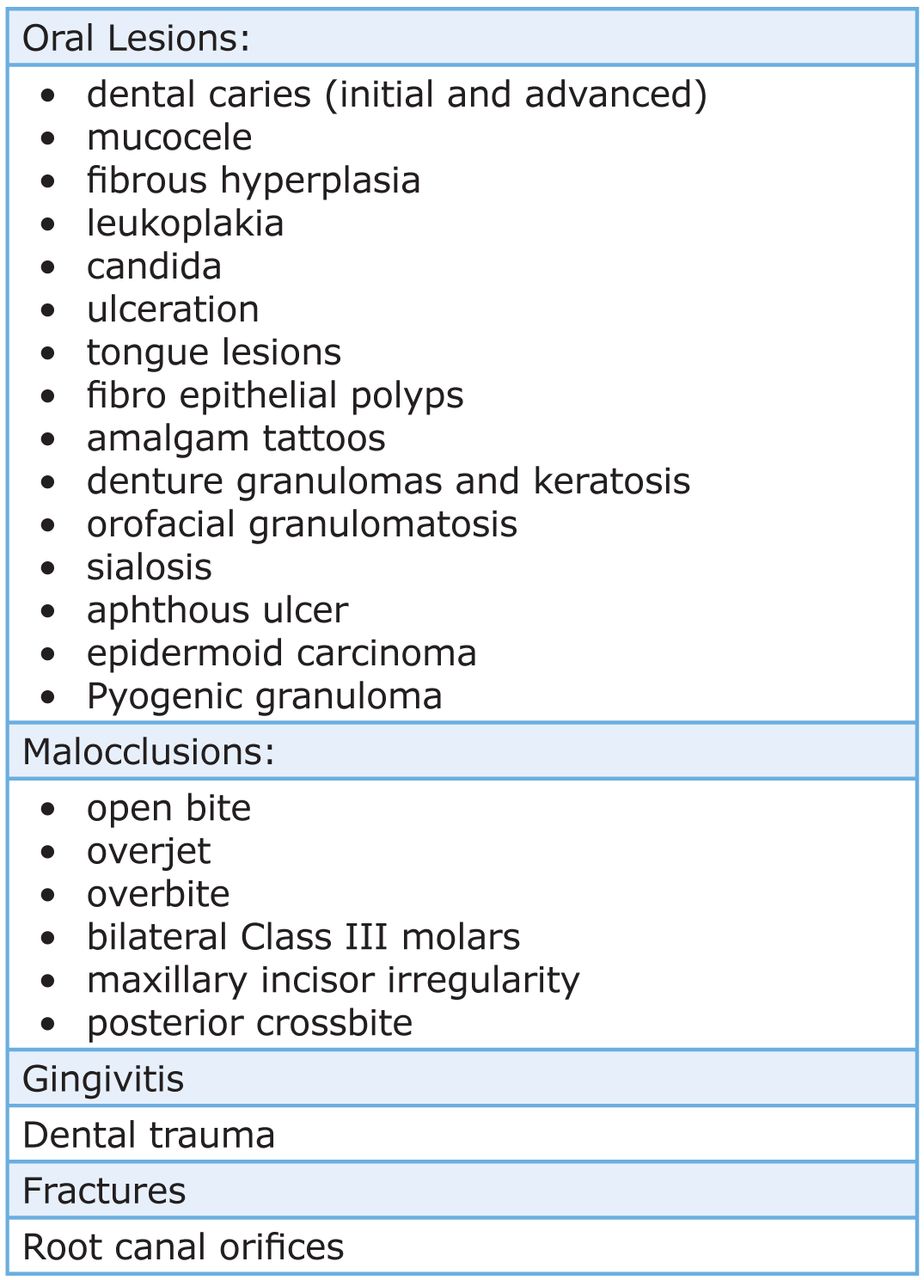
Oral Lesions and Conditions Documented in Teledentistry Assessments
Teledentistry has been used in offsite clinics to assess orthodontic need and to provide instruction for students providing interceptive orthodontics. When compared to a second group of students at a site with face-to-face faculty supervision, the assessment of need and development of interceptive appliances was found to be as effective as the site where faculty were present.19
Endodontics
The accuracy and reliability of teledentistry for identifying canals within extracted molars resulted in moderate agreement among 20 examiners. A total of 88% of canals in the 50 permanent molars were identified correctly from photographs. Dentists with >10 years of experience were more accurate in detecting canals than those with less experience. Accuracy of detection was also greater in mandibular molars than maxillary molars.26
Oral Lesions and Screening for Oral Trauma
Access to an oral medicine specialist or oral pathologist for diagnosis of lesions is often limited, or long waiting periods exist. One feasibility study compared 2 specialists' teledentistry diagnosis of 25 cases to final diagnosis.21 Biopsy was performed in some cases to obtain exact pathology. The 2 examiners agreed on correct pathology in 60% of the cases. In the 10 remaining cases the examiners were not accurate with the diagnosis or they were not in agreement. One examiner correctly identified 88% of the 25 cases.21 In the final analysis, weighted kappa only resulted in fair agreement (K=0.28).
Of 37 patients in Belfast who had been on wait lists for clinical examinations by an oral medicine specialist, teledentistry examinations found 8 patients needing urgent biopsies, and 24 patients with common oral lesions were treated in the community dental service under a consultant's supervision via teledentistry.23
Telemedical centers in Switzerland provide free consultations for triage associated with trauma or other conditions. Looking toward future changes to decrease costs in the Swiss health system that would require all individuals have a teledental or telemedical consult prior to accessing a health care provider, one group of researchers conducted a retrospective study of dental triage data obtained over 7 years to determine the nature and advice provided.24 Of the 371,988 telephone sessions, most were provided by medical personnel, contacts occurred after hours and involved dental trauma to children (n=3,430, average age 8.6 years).24
In summary, there are fewer studies that examined satisfaction outcomes as compared to clinical outcomes. Nevertheless, there is a trend of good attendance at teledentistry programs and good compliance with 5 studies (26%) reporting on satisfaction.12,13,15,18,25 While 4 of these studies reported the clinicians' perspective, only 1 study 25 examined both patient and clinician perspectives.
Overall, the findings are very encouraging, with patients and therapists reporting positive perceived benefits, convenience and usefulness of the teledentistry program. Dental professionals rated overall satisfaction with equipment functioning. Radiographs were rated good, and photos and study models were rated either good or excellent.25 In one study, clinician's found moderate satisfaction with diagnostic information and more concern over equipment security than patient confidentiality.14
Health Care Utilization
A total of 3 studies reported health care utilization outcomes.11,13,27 The commonly reported outcomes include the effect on referral rates, inappropriate referral rates, failed appointments, prevalence of caries and general dental practitioner visits.13,27 Inappropriate orthodontic referrals were lower in the teledentistry group (8.2%) compared to the control group (26.2%). Previous inappropriate orthodontic referral rates were up to 45% resulting in poor use of professionals' and patients' time.13
In a comparative-effectiveness study, the care utilization in preschool urban children enrolled for teledentistry examinations was as effective and accurate as traditional clinical exams for dental caries screening.27 No significant difference was found between groups.
Costs
Two studies presented some type of cost analysis of the teledentistry intervention.11,15 One examined costs from the patient's perspective using a questionnaire to obtain information concerning distance, travel time and cost to visit a specialist's hospital. Cost of time from work and overnight accommodations were also assessed. Travel time resulted in an average of 12 hours lost productivity for those from Orkney and 2.5 hours for patients from Kingussie.11
Ignatius et al's 2005 report studied cost of teledentistry technologies for 26 dental specialist trainees in 8 cities in Finland.15 Costs were calculated for travel, purchase and equipment operation. The use of teledentistry was estimated to save each student at least 43,600 Euros.
Discussion
The findings from the current systematic review are in part supported by those reported by other telemedicine systematic reviews not related to dentistry. These reviews consistently report that there are a few areas of telemedicine, such as teledermatology, teleradiology and telemental health, where there is emerging evidence for the efficacy of telemedicine, but few studies supporting the cost benefits of telemedicine, and no evidence of the long term outcomes of telemedicine.28-33
More specifically, this systematic review of teledentistry showed that although there is heterogeneity between studies in terms of study designs, clienteles, settings and outcomes measured, a trend exists supporting the efficacy and effectiveness of teledentistry. Many quality studies, including studies with control groups, reported similar or better clinical outcomes when compared to conventional interventions. Use of teledentistry resulted in slightly higher DFS scores than those found in clinical examinations of the same children10,17,20,22,27 When screening groups of young children, referral for care based on a false positive is not as detrimental as non-referral based on a false negative.
One study reported the incorporation of a 1 credit hour, 15 week teledentistry course in a dental hygiene program.16 Students' knowledge, attitudes and confidence were evaluated prior to and following the course. Confidence, knowledge and attitudes were significantly different on 9 of the 10 item questionnaire following the course. Including a teledentistry course within the curriculum provides oral care professionals the skills needed to improve access to care.
Overall, satisfaction ratings regarding the use of teledentistry were very high from both patients and therapists, regardless of the patient population, setting or study design. However, certain measurement issues limit the usefulness of the reported data. For example, the tools used to measure satisfaction are for the most part poorly described and not standardized. The underlying satisfaction concept is often vague, making the interpretation of satisfaction findings unclear. Findings are generally limited to satisfaction with the technology, the service received/given, but there are no details of the service delivery or their experience in the program.
The findings in this review are similar to the conclusions arrived at by Mair33 as well as Williams et al34 in their systematic reviews of studies reporting patient satisfaction with telemedicine. Continuing to measure user satisfaction in the current manner will simply confirm previous findings of acceptability of the technology, but will not increase the understanding of the underlying processes of teledentistry use. A better understanding of satisfaction remains an important area for future research in teledentistry.
The use of teledentistry for screening of oral diseases to determine prevalence and treatment needs, and provide access to specialists for consultations, is promising. Oral diseases impact health and quality of life for many. Expanding the roles of dental hygienists and removing practice restrictions would increase the number of oral care providers who could perform screenings, care and referrals using teledentistry.
Reduced costs or better resource utilization is often cited as one of the main goals of teledentistry.11,15 In conducting cost analyses, it is crucial to identify from which perspective the analysis is being conducted - in other words, who is defraying the costs or achieving the savings, be it the patient, caregiver, clinician, health care organization, health care system, reimbursement agency, society and so on. None of the studies presented here calculated costs using the same elements.
While the studies in this review included calculations of costs incurred or saved from an organizational or patient perspective, the costs were not related to clinical or health care utilization outcomes. If outcomes are similar between a teledentistry program and an alternative program, then cost-minimization or the cheaper of the 2 interventions is an appropriate measure of costs. If outcomes are different, then it is more relevant to identify how much more or less a teledentistry program costs compared to an alternative, taking into account the change in clinical outcomes of each program. Cost differentials such as the incremental cost-effectiveness ratio can be useful in this case.
It may also be pertinent to examine whether certain resources or programs will no longer be available if a teledentistry program is introduced, particularly in a context of limited public health care funding. Monetary costs have to be weighed against the quality of life for individuals who remain on long waiting lists for consultations, referrals or care and children with undiagnosed dental caries who suffer with pain from infection, develop sepsis and die as Deamonte Driver in 2007.35
Likewise, costs associated with prolonged waits to receive a diagnosis for certain oral lesions results in increased morbidity and mortality.23 Dental hygienists utilizing teledentistry in underserved or no access areas could screen, provide care and prevent the progression of an oral disease beyond repair or recovery.23
Limitations of this Systematic Review
It is generally accepted in meta-analyses and systematic reviews that clinical trials, particularly RCTs and other quasi-experimental designs, are best suited for assessing the efficacy and cost-effectiveness of an intervention, and thus provide stronger evidence on which to base conclusions.
Common methodological weaknesses in these studies included lack of blinding of dentists, patients or assessors. While in teledentistry it is not always feasible to design studies with patients and dentists who are not aware of group assignment, use of outside assessors reduces the potential for evaluation bias. Many of the studies used convenience samples based on geographical location of patients or patient preference, clearly introducing the possibility of selection bias. A total of 12 studies (60%) had sample sizes of fewer than 20 subjects, and only 1 of the studies provided power calculations.13 Small sample sizes can lead authors to conclude that no significant difference exists between groups, i.e. a Type II error, whereas the study may have insufficient power to identify a significant difference.28,29 Nevertheless, larger studies often remain challenging to carry out, as many of the teledentistry programs are still in their pilot phases and there is often limited availability of the patient population concerned.
Another limitation of this systematic review is that it uses studies published in peer-reviewed journals. It is well documented that there is a publication bias toward studies that have positive findings.36 Therefore, studies that do not demonstrate any effect or report a negative effect of teledentistry may not carry as much weight in the synthesis of the data because they were not identified through the search. Moreover, this review did not include patient assessment studies as the focus was on intervention programs.
Conclusion
This systematic review identified a substantial amount of scientific literature in the relatively new area of teledentistry. Although there is heterogeneity between studies in terms of study designs, settings and outcomes measured, there is a consistent trend supporting the efficacy and effectiveness of teledentistry. Further research in the area of teledentistry, with methodologically stronger studies examining clinical outcomes, health care utilization and costs in greater depth are critical for evidence base. From the data available, teledentistry seems to be a promising path for access to care in rural and urban settings.
Acknowledgments
The authors wish to acknowledge the support of their respective departments in the development of this manuscript.
Footnotes
-
Susan J. Daniel, RDH, PhD, is Assistant Professor, Department of Dental Hygiene. Lin Wu, MLIS, AHIP, is an Associate Professor & Reference Librarian, Health Sciences Library. Sajeesh Kumar, PhD, is an Associate Professor, Department of Health Informatics & Information College of Allied Health Sciences. All authors are at the University of Tennessee Health Science Center, Memphis.
-
This study supports the NDHRA priority area, Health Promotion/Disease Prevention: Identify, describe and explain mechanisms that promote access to oral health care, e.g. financial, physical, transportation.
- Copyright © 2013 The American Dental Hygienists’ Association





{kind=link}
{kind=link}