



Abstract
Purpose: The purpose of this systematic review was to describe the oral health literacy (OHL) inventories that have been used among caregivers of preschool-aged children.
Methods: Four databases were searched (CINAHL, Cochrane Database of Systematic Reviews, Dentistry & Oral Sciences Source, PubMed), to identify peer-reviewed, full-text studies published in English on the oral health literacy among caregivers of preschool-aged children from 2010-2021. All studies were assessed for eligibility using PRISMA guidelines. Inclusion criteria were experimental, non-experimental, or mixed methods peer-reviewed studies, conducted in the United States. Eligible studies were independently evaluated using the Effective Public Health Practice Project’s Quality Assessment Tool.
Results: The initial search yielded 182 articles; 11 studies met the inclusion criteria after screening: observational (n=8), experimental (n=2), and quasi-experimental (n=1). Main outcome measures included: oral health literacy, oral health knowledge, oral health attitudes and behaviors, child oral health status (COHS), child oral health-related quality of life (C-OHRQoL), and child oral health-related expenditures. However, this review focused only on caregivers’ OHL and the associated measurements for this variable. Most studies utilized the Rapid Estimate of Adult Literacy in Dentistry (REALD-30); the remainder used the Basic Research Factors Questionnaire (BRFQ), the Oral Health Literacy Inventory for Parents (OH-LIP), or self-designed survey questions.
Conclusions: Few studies met the inclusion criteria. There was an uneven distribution of studies using different inventories for the measurement of oral health literacy limiting the generalizability of the findings to low-income and minority groups. Most caregiver OHL studies focused on dental word recognition, only a few measured knowledge and comprehension. More comprehensive inventories could be designed to evaluate caregivers’ knowledge and understanding of dental terms.
Introduction
The concept of personal health literacy describes the degree to which an individual can obtain and understand basic health information needed to make important and timely health decisions.1,2 Low health literacy has been linked with poorer health, health-related behaviors, and health outcomes.3-6 While the concept of personal health literacy continues to receive significant attention among the research community, a complimentary concept focusing specifically on oral health literacy also has become a prominent research topic. Oral health literacy (OHL) is defined as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate oral health decisions.”7 Individuals with low OHL are less likely to obtain necessary and timely preventive dental care, as a result, they tend to have poorer oral health outcomes.8-10 In addition, caregivers’ oral health literacy may have an important role in their young children’s oral health status, oral healthcare utilization, and outcomes.8-10
Early childhood caries continues to be a public health concern among preschool-aged children in the United States (US) and has been associated with low or inadequate caregiver oral health literacy.8,11,12 In particular, the prevalence of dental caries is greatest among children in low-income families compared to children from higher-income families.13 Early childhood caries is defined as the presence of 1 or more decayed, missing, or filled primary tooth surfaces among children under the age of six years.14 According to the National Health and Nutrition Examination Survey (NHANES 2011-2016), approximately 23% of children aged 2-5 years experienced decay in their primary dentition, a 4.6% decrease from a prevalence of 27.9% from NHANES 1999-2004.15
Research has shown that poor OHL of the caregiver is related to poor oral health status, untreated dental caries, and a greater lifetime of dental caries for the child.8,12 Caregivers who have a limited or inaccurate understanding of dental terms may not be able to model and promote proper oral hygiene techniques to their young children. When caregivers are provided proper information and education, they are positioned to promote recommended oral health behaviors. Awareness of caregivers’ level of health literacy provides both dental and non-dental professionals with the information needed to effectively tailor communication and educational materials for maximum comprehension. Increasing caregivers’ understanding and comprehension of oral health may be the first step to improving oral health behaviors that translate into better oral health status and use of preventive services for the child.
The purpose of this systematic review was to address the question, “What are the oral health literacy inventories that have been used to describe the oral health literacy of caregivers of preschool-aged children?
Methods
Search strategy
An initial literature search was conducted in April 2021 by the primary investigator (PI) using PubMed, CINAHL Plus with Full Text, Cochrane Database of Systematic Reviews, and the Dentistry & Oral Sciences Source. Various combinations of selected keywords were used in the initial search. Search terms included: oral health literacy OR “oral health literacy” AND caregiver OR mother OR parent AND preschool age children OR child OR toddler OR preschooler. Once the initial database search concluded, an individual search of article reference lists was performed to identify any additional qualifying studies. After the search was complete, two additional investigators screened the list of article returns based on the chosen research question for this review.
Eligibility criteria
Inclusion criteria for the systematic review were experimental, non-experimental, or mixed methods peer-reviewed studies, conducted in the United States from 2000-2021, and written in the English language. Specifically, studies that examined caregiver oral health literacy and child oral health status among preschool-aged children were included in the review. Studies were excluded if they were case reports, editorial reviews, personal communications, or narrative reviews.
Study selection
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) check list was used as a guide for the systematic review.16 Three researchers discussed the study eligibility criteria and then independently conducted the review process. Independent evaluations of all the article titles identified in the initial database search were completed, duplicates and non-US studies were removed, then the remaining studies were screened by both title and abstract. Finally, full-text articles were assessed for eligibility based on the inclusion criteria by all three reviewers. In the case of disagreement among the reviewers, eligibility criteria were further discussed until a consensus was achieved.
Risk of bias in individual studies
The quality of each eligible study was assessed by two reviewers who independently evaluated the quality using the Effective Public Health Practice Project’s Quality Assessment Tool for Quantitative Studies.17 This tool contains eight components that evaluate study design, selection bias, data collection methods, confounders, blinding, withdrawals and drop-outs, intervention integrity, and analyses. Each of the eight sections were completed via questions with multiple choice answers scored according to the tools specific criteria provided in the accompanying dictionary. Upon the completion of each section, an overall rating (strong, moderate, or weak) was given based on the answers for that section. The overall quality of the entire article was determined by the final calculation of the component ratings. Strong articles contained no weak component ratings, moderate articles contained one weak component rating, and weak articles contained two or more weak component ratings total. Discrepancies among article ratings, due to differences in interpretation, were discussed by both reviewers until a unified consensus was reached. The eligible articles were summarized according to the author(s) and year, study design, setting, sample size and age range, OHL instrument utilized, outcomes, and significant results.
Results
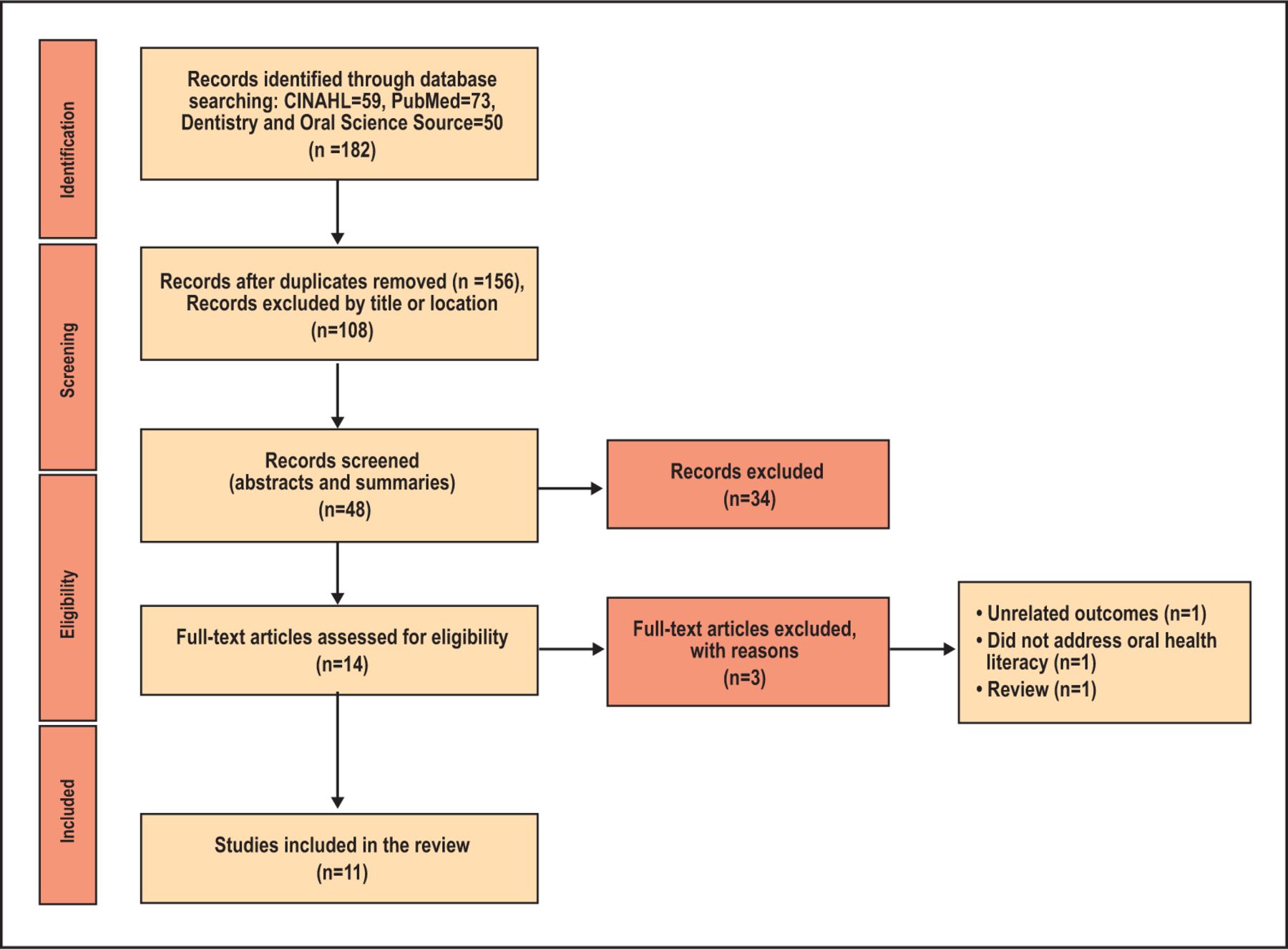
A total of 182 search results were obtained from the chosen databases. After duplicate articles were removed, 156 articles remained. An additional 108 articles were excluded based on title or studies conducted outside of the United States. The remaining 48 articles were considered for full-text screening by the three reviewers. A total of eleven articles met the inclusion criteria set for this review (Table I). Each article was assessed for risk bias using the Effective Public Health Project’s Quality Assessment Tool for Quantitative Studies and received a score of high (n=2), moderate (n=7), or weak (n=2). The complete study selection process for this review is summarized in Figure 1.
Summary and Characteristics of included Studies (n=11)

Screening of articles: Four-phase preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow-diagram.
Study characteristics
The eleven articles included in this systematic review were either experimental (n=2), quasi-experimental (n=1), or observational studies (n=8) and met the inclusion criteria determined by the primary and secondary reviewers. Participant populations included caregiver-child dyads from Head Start programs (n=4), The Carolina Oral Health Literacy Project (n=5), or community dental clinics (n=2). Caregiver-child dyads consisted of a primary caregiver (mother, father, grandparent, legal guardian, etc.) and a preschool-aged child. Most studies (n=8) defined preschool aged as <60 months with the remaining studies (n=3) including children up to 72 months of age. Sample sizes for the 11 studies ranged from 45 to 2,011 participants. The main outcomes examined included: caregivers’ oral health literacy, oral health knowledge, oral health attitudes and behaviors; and the child’s dental caries, oral health status, oral health related quality of life, and oral health related expenditures.
The primary outcome measure examined was oral health literacy inventories. Approximately half of the studies utilized the Rapid Estimate of Adult Literacy in Dentistry (REALD-30; n=6) to evaluate oral health literacy, the remaining studies utilized the Basic Research Factors Questionnaire (BRFQ; n=2), the Oral Health Literacy Inventory for Parents (OH-LIP; n=2), or self-designed survey questions (n=1). With the exception of the self-designed survey items, all inventories examined in this review have established validity and reliability, as reported in those studies.
Oral health literacy/knowledge
Six studies utilized the REALD-30 inventory to evaluate caregiver oral health literacy: Divaris et al.18-20 (n=3), Vann et al.21-22 (n=2), and Miller et al.12 (n=1). The five studies from Divaris et al.18-20 and Vann et al.21-22 examined data from the Carolina Oral Health Literacy project (COHL), a prospective study evaluating the relationship of OHL with health behaviors and outcomes among caregivers of preschool-aged children enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) in North Carolina. Miller et al. conducted a cross-sectional study, utilizing the REALD-30, of preschool-aged children presenting for an initial dental appointment at the UNC-Chapel Hill School of Dentistry.12 Scores for the REALD-30 inventory range from 0-30 with no set scale to determine specific levels of OHL. The five COHL-related studies designated a REALD-30 score of less than 13 as “low OHL”, while Miller et al. chose scores less than or equal to 22 as “limited literacy.”12 Among the six studies, the mean REALD-30 scores ranged from 15.6 to 20.7. However, most studies indicated a quarter to more than half of the caregivers had low OHL when utilizing the REALD-30.12,18,20,22
Albino et al. and Brega et al. examined the oral health literacy of American Indian parents or caregivers of preschool-aged children participating in Navajo Nation Head Start programs.23,24 Data for both studies consisted of secondary data from a previous clinical trial that tested an intervention applied in Navajo HS classrooms to reduce the incidence of Early Childhood Caries (ECC). The initial clinical trial utilized the Basic Research Factors Questionnaire (BRFQ) to assess caregiver OHL. Developed for use in clinical trials, this questionnaire assesses common predictors, mediators, and moderators of early childhood caries (ECC).25 The BRFQ contains three questions related to health literacy (score range: 1-5), nine related to oral health behaviors (score range: 0-100%), and 14 related to oral health knowledge (score range: 0-100%).23
Abino et al. examined the association among psychological and social variables reported by the caregivers and changes in their oral health knowledge and oral health behaviors related to the care of their child’s dentition.23 Only baseline data and one-year follow-up data were analyzed among the analytic cohort of 474 caregiver-child dyads. Caregivers’ mean baseline health literacy was (4.0 + 0.8), oral health knowledge (74.8 + 13.2), and oral health behavior (51.0 + 21.7). Mean increases from baseline to one-year follow-up were 3.8 percentage points for oral health knowledge and 3.9 percentage points for oral health behaviors following the intervention program. Results showed that oral health knowledge increased when parents perceived their child’s oral health to be a matter of chance or controlled by professionals, not themselves.
Brega et al. utilized the same data set but included the two-year follow-up to investigate the relationship between parental health literacy and their child’s oral health outcomes.24 The authors also developed a theoretical model to summarize the relationship between health literacy and oral health outcomes among the caregiver-child dyads (n=1,016). Parental health literacy was found to be associated with oral health knowledge, behavior, and attitudes. Mean health literacy (4.0 + 0.8), oral health knowledge (74.3 + 13.4), and adherence to recommended oral health behaviors (55.2 + 18.8) were similar to those found by Albino et al. when the entire sample was evaluated from baseline to 2-year follow-up.
Richman et al. and Chi et al. both utilized the Oral Health Literacy Inventory for Parents (OH-LIP) to evaluate oral health word recognition, vocabulary knowledge, and comprehension of caregivers of preschool-aged children.10,26 Richman et al. examined the oral health literacy of 45 parents/caregivers enrolled in two Head Start programs in Washington state, while Chi et al. used the same inventory with 113 parent/caregivers within a pediatric dental clinic, focusing specifically on the term “fluoride varnish.”10,26 Richman et al. concluded that word recognition alone may overestimate a caregiver’s OHL, with the majority of the sample scoring 78% or better on the word recognition section. Yet, half of the terms were scored as incorrect or partially incorrect for the majority of participants in the vocabulary knowledge section.10 Chi et al. showed similar results with the majority of caregivers having an incomplete or inaccurate understanding of the term “fluoride varnish.”26
Lastly, Dudovitz et al. utilized three items to assess parent knowledge of positive oral health behaviors: “When should you take your child for a first dental check-up?”, “Why are baby teeth important?”, and “What are some good ways to prevent tooth decay.”27 The objective of this study was to determine whether an oral health literacy intervention, among caregivers of preschool-aged children in HS programs in the US, would improve the OHL and behaviors of caregivers? The intervention was considered successful with a significant increase from baseline to follow-up in all three of the knowledge-related items. Knowledge of when to bring their child in for their first dental visit increased from 24.96% to 91.43% (p<0.001). Mean knowledge scores (range: 0-4) about the importance of baby teeth increased from 2.88 to 3.40, and mean knowledge scores of good ways to prevent tooth decay increased from 1.80 to 3.44 (p<0.001).
Discussion
Several valid and reliable instruments currently exist to measure adult oral health literacy, the most commonly used being the Rapid Estimate of Adult Literacy in Dentistry (REALD-30). Based on the Rapid Estimate of Adult Literacy in Medicine (REALM), this shortened, dental-specific instrument requires respondents to pronounce 30 oral health-related terms which are scored to determine an individual’s word recognition capabilities.28 Total scores for the inventory are open to individual interpretation, with most researchers choosing to designate <13 correct responses as “low” oral health literacy. While word recognition is an important indicator of literacy skills, knowledge and comprehension skills may be a better predictor of oral health literacy and may indicate how well individuals truly understand the health information they are receiving from dental and non-dental professionals. To capture a more complete assessment of oral health literacy, Richman et al. developed the Oral Health Literacy Inventory for Parents (OH-LIP).10 This three-part inventory assesses the word recognition, vocabulary knowledge, and comprehension of 36 pediatric dental-related terms through structured interviews. Part one requires respondents to read a list of dental-related terms similar to those in the REALM and REALD-30 inventories followed by part two which requires respondents to give a verbal definition of each term. Finally, part three requires participants to listen to 36 brief passages, each one containing one of the initial dental terms. Participants are asked to evaluate their understanding of the information, including their ability to act upon it appropriately.10 While previous systematic reviews have evaluated research on the oral health literacy of caregivers of preschool-aged children, most included studies utilized the REALD-30, which only evaluates word recognition. Additional inventories, such as the OH-LIP, are needed to evaluate the full comprehension of pediatric dental terms and dental-related information.
More than half of the research studies included in this systematic review evaluated OHL by using the REALD-30, an inventory that requires respondents to pronounce a series of oral health-related terms arranged with increased reading difficulty.28 While this inventory is considered a valid and reliable measure of OHL, it only evaluates word recognition making it difficult to determine knowledge and comprehension of the dental-related terms. Moreover, the REALD-30 was developed to evaluate the dental word recognition of adult respondents and is not specific to caregivers or parents with young children. The general adult population, including parents and caregivers of young children, may have seen or heard a term in the past that they can recognize and pronounce; however, they may not know the true meaning of the term and are potentially incapable of comprehending the meaning of the term in an oral health related context.
The more recent development and validation of inventories measuring OHL, including the BRFQ and the OH-LIP, have expanded upon word recognition to evaluate oral health knowledge and comprehension. Both inventories provide a more comprehensive assessment of OHL related to pediatric oral health among parents or caregivers of young, preschool-aged children who are at risk for early childhood caries. Following the 2011 article reporting on the development and validation of the OH-LIP by Richman et al., two studies have utilized the OH-LIP to examine caregivers’ word recognition, vocabulary knowledge, and comprehension of dental terms such as “fluoride varnish” or “decay” and “cavity.”10 Both studies by Chi et al.11 and Claiborne et al.26 found an inadequate understanding of dental related terms specific to fluoride varnish and dental caries, respectively, among caregivers of preschool-aged children. Continued research efforts are needed to develop additional inventories for diverse populations that measure a comprehensive understanding of pediatric oral health terms.
Focused consideration of a population’s OHL levels and current child oral health status allows for the development of dental specific education, messaging and interventions. Future studies are needed to determine the potential for increased positive oral health behaviors and use of preventive care in a timely manner through increased OHL. New interventions aimed at increasing OHL among pregnant women, new parents, and caregivers of young children could provide a means to reduce the burden of early childhood caries. Continued research efforts are needed to develop additional inventories for diverse populations that measure a comprehensive understanding of pediatric oral health terms.
Limitations of this systematic review include the low number of studies that met the inclusion criteria. In addition, there was an uneven distribution of studies among the different inventories used for the measurement of oral health literacy with the majority of included studies utilizing the REALD-30 to measure dental word recognition. Finally, given the study populations chosen for the majority of the studies, the generalizability of the findings is limited to low-income and minority groups. However despite these study limitations, to the best of the authors’ knowledge, this is the first systematic review to examine the most current trends in oral health literacy research, focusing on the inventories used for the evaluation of OHL among caregivers of preschool-aged children.
Conclusions
A limited number of inventories focus on the OHL of caregivers of preschool-aged children. Low oral health literacy may impede a caregiver’s ability to make timely oral health care related decisions on behalf of their child. Dental and non-dental providers need to be cognizant of caregivers’ level of OHL so that oral health communication and educational materials can be tailored to meet their specific literacy needs.
Footnotes
This manuscript supports the NDHRA priority area Population level (access to care) vulnerable populations.
- Received February 28, 2022.
- Accepted July 7, 2022.
- Copyright © 2022 The American Dental Hygienists’ Association





{kind=link}