



Abstract
Purpose: Growing evidence associates low oral health literacy (OHL) with poor oral health outcomes. While nearly half of United States adults have periodontal disease (PD), there are conflicting results on association between OHL and PD. The purpose of this pilot study was to explore the association between functional OHL and periodontal health as defined by the American Academy of Periodontology (AAP) classification system.
Methods: A cross-sectional study was conducted with a convenience sample of dental patients presenting for care at a Midwestern Federally Qualified Health Center. Functional OHL was measured using the Oral Health Literacy Adults Questionnaire (OHL-AQ), and periodontal health was measured clinically and categorized by stage and grade using the recently revised AAP classification system. Additional demographic factors and health history information related to periodontal health were collected. Descriptive analysis reported the median and range for ordered variables, and frequency and percentages for categorical variables. Wilcoxon rank sum test, Kruskal-Wallis test, and Spearman correlation coefficients were used to find association between functional OHL and periodontal health.
Results: Among fifty-four participants, statistically significant associations were found between OHL-AQ scores and AAP staging and grading categories. Periodontal disease stage increased with age, and periodontal disease grades progressed among participants with diabetes. No associations were found between periodontal health and sex, race, ethnicity, education, insurance, or country of origin.
Conclusion: Functional oral health literacy had a significant inverse relationship with both AAP periodontal disease staging and grading. A larger study is needed to confirm the findings of this pilot study.
- oral health literacy
- functional oral health literacy
- periodontal health
- periodontal disease grading
- oral health outcomes
Introduction
Oral health literacy (OHL) is defined as, “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate oral health decisions.”1 Patients with low oral health literacy are more likely to have poorer oral health outcomes related to missed dental appointments, demonstrate greater levels of dental anxiety, and have poorer oral health including dental caries and temporomandibular joint problems.2–10 In addition, oral health literacy is linked to the social determinants of health theory, asserting that when social factors including economic stability, education, health, served health care, neighborhood, built environment, social and community context are compromised, people are more likely to have lower levels of OHL and poorer health outcomes.11 Building on these concepts, the American Dental Association (ADA) proposed a conceptual model designed to address low oral health literacy that includes educational systems, health systems, and cultural/social factors.12 Both the social determinants of health theory and the ADA model suggest that if low oral health literacy levels are not addressed or improved, poor health outcomes will persist.11,12
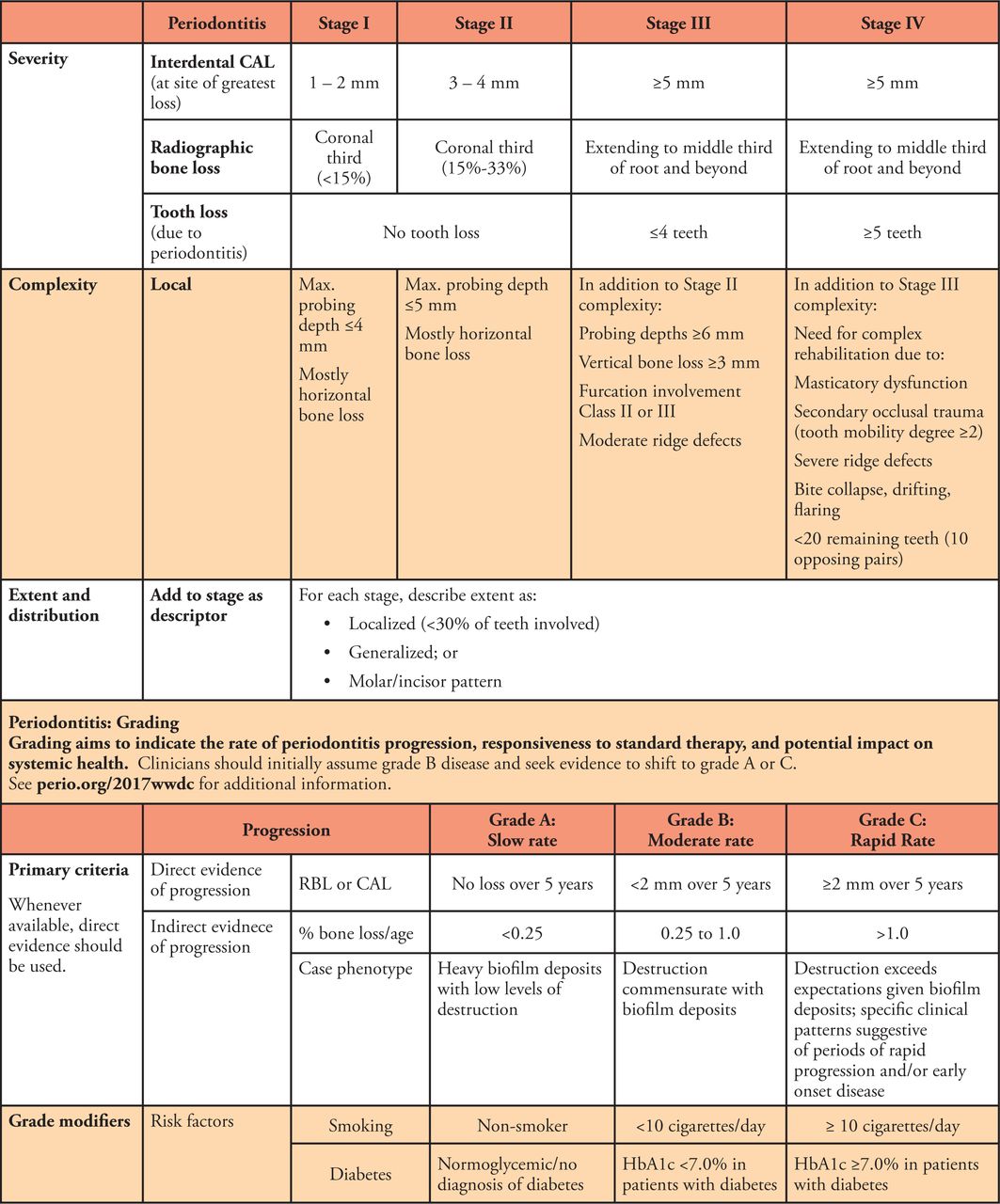
Periodontal disease (PD) affects the soft and hard tissues of the oral cavity, and can lead to tooth loss if not treated and controlled.13 Nearly half of adults residing in the United States (US) have been diagnosed with periodontal disease.13 As evidence-based dentistry has evolved, strong associations have been identified between the progression of PD and diseases such as diabetes, and behaviors such as smoking. Due to these and other considerations, the American Association of Periodontology (AAP) revised periodontal staging categories to include grading criteria in 2017.14 This revised system describes stages of diseased periodontium, and the progression of PD as influenced by co-morbidities and behaviors through grading (Figure 1).

AAP Periodontal Disease Staging and Grading14
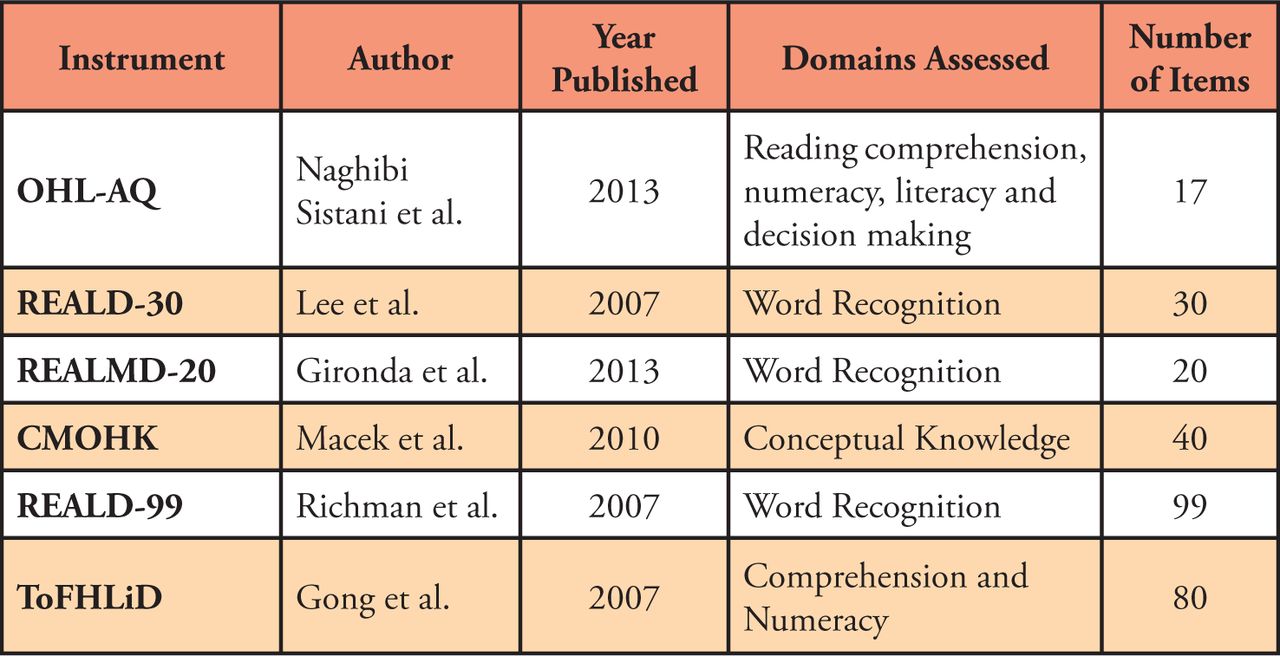
While several studies have demonstrated an association between OHL and PD, a systematic review conducted by Firmino et al. concluded that these findings were unsubstantiated because of the considerable heterogeneity in measuring both PD and OHL.15 Examples of PD measures include plaque and gingival indices, bone loss, and screening tools such as the Community Periodontal Index (CPI).15 As summarized in Figure 2, multiple OHI instruments are available but fall short in their ability to capture the full scope of oral health literacy.16 For example, several validated instruments measure word recognition only (REALD-99, REALD-30, REALM-D, and REALMD-20), while others are limited to measuring conceptual knowledge (CMOHK) or a combination of reading comprehension and numeracy (ToFLiD).17 As OHL instruments continue to evolve, recent instruments capture several practical aspects described as “functional oral health literacy.”16

Examples of OHL instruments, domains assessed and number of items17
One instrument designed to test functional OHL is the Oral Health Literacy Adults Questionnaire (OHL-AQ).16 Functional oral health literacy is the ability to successfully navigate the health care environment and includes tasks such as reading prescription labels, making and keeping appointments, and completing and understanding health forms.16,18 Functional OHL is measured by assessing word recognition, reading comprehension and numeracy, conceptual knowledge, and evaluating listening and decision-making skills.16,18
Noting the changes in available OHL instruments to include measures of functional OHL, and the availability of a more comprehensive system to measure both periodontal health and disease, the purpose of this study was to use the OHL-AQ and the AAP classification system to measure the association between periodontal health and OHL. While several studies report an association between OHL and periodontal disease, to the authors’ knowledge, there are no studies that use a functional OHL instrument and the definitive American Academy of Periodontology (AAP) classification system. Examining this association may assist clinicians and oral health care systems in implementing systems to better accommodate patients with low OHL with the goal of improved periodontal health.
Methods
This study used a cross-sectional design and was conducted in a Midwestern federally qualified health center (FQHC). The FQHC dental clinic serves a diverse patient-base from 61 counties throughout the state and offers medical, dental, and behavioral health services. This study was approved by the University of Minnesota Institutional Review Board (ID 0009459).
Sample
A convenience sample of fifty-four new patients and patients of record presenting for a regularly scheduled dental hygiene appointment were recruited by the dental hygienist when presenting for their appointment. Each of the fifty-four patients that were recruited over a one-month time period qualified and consented to study participation. Inclusion criteria were adult patients aged 18 years and older presenting for dental hygiene care and the cognitive ability to consent for study participation. Patients were required to have a minimum of 3 teeth, with at least two adjacent teeth, and at least one additional non-adjacent tooth to conduct a diagnostic periodontal assessment. Exclusion criteria were patients unable to participate in the survey due to mental or physical limitations, patients that required a medical interpreter, or those experiencing dental pain requiring immediate treatment. Patients meeting inclusion criteria and agreeing to participate signed an electronic informed consent and Health Insurance Portability and Accountability Act (HIPAA) document. A power analysis determined a minimum sample size of n=45 participants to detect a moderate effect size assuming 80% power and an alpha level of 0.05.
Data Collection
Functional oral health literacy was measured using a validated survey and periodontal health was assessed clinically. The primary investigator (PI) was a dental hygienist employed by the FQHC. The PI collected all data and had been trained on the AAP classification system through various calibration sessions with other dental hygienists at the FQHC and through continuing education courses. Patients were given an electronic tablet to record their survey answers and were given the option of the investigator inputting their answers if they preferred or were not comfortable using the tablet. Following survey completion, the periodontal assessment was completed and entered into the patient’s electronic health record, as part of the clinic’s standard dental hygiene care protocol. The PI then entered the participant’s periodontal health status according to the AAP periodontal disease staging and grading system. The dental hygiene appointment continued, and all scheduled care was completed. Participants were thanked for study involvement; no remuneration was provided.
Instruments
The instrument consisted of demographics (7 items), health history (3 items) and OHL-AQ (17 items). The Oral Health Literacy Adults Questionnaire is a validated survey that measures functional oral health literacy and was originally developed in Iran.16,19 Seventeen items assess word recognition, reading comprehension and numeracy, conceptual knowledge, listening and decision-making skills.16,19 Two questions were verbally administered to assess listening and comprehension skills. Values for correct answers were scored as “1” and incorrect answers were scored as “0”. Scores for all items were totaled with a potential sum ranging from 0 to 17 with higher scores indicating increased functional OHL.16,19
Demographic variables collected via the survey included gender, race, ethnicity, education, and type of dental insurance, if any. As part of the AAP periodontal disease staging and grading system, smoking and diabetes status were collected, as they are known risk factors for periodontal disease.14
The periodontal assessment involved collection of pocket depths, clinical attachment loss (CAL), recession, bleeding upon probing, mobility, furcation involvement, radiographic bone loss, gingival tissue evaluation, and periodontal risk assessment. Periodontal health status was classified using the recently updated American Academy of Periodontology (AAP) classification system as detailed in Figure 1.14
Patient findings were categorized as: healthy (no periodontal disease involvement), gingivitis (reversible gingival inflammation), or periodontal disease (irreversible periodontal disease involvement). If periodontal disease was found, calculation of the participants’ staging, and grading of their disease was completed. Staging measures the severity and extent of the disease and was categorized as stage I, stage II, stage III or stage IV, as defined by the AAP classification system.14 Grading measures the rate of disease progression, responsiveness to treatment and impact on overall health as is divided into three categories: grade A (slow rate), grade B (moderate rate) and grade C (rapid rate).14 As shown in Figure 1, modifying factors include smoking and diabetes status were also collected for AAP periodontal disease staging and grading.14
Statistical Analysis
Descriptive statistics were calculated for each variable, reporting counts and percentages for categorical items, and medians and ranges for quantitative variables. Bivariate associations between primary outcomes (identify) and covariates were tested by the non-parametric Wilcoxon rank sum test (2 categories) or the Kruskal-Wallis test (more than 2 categories). Spearman correlation coefficients measured the association between two ordinal scale variables. Functional OHL was analyzed with each individual demographic factor to determine individual associations. P-values less than 0.05 were considered statistically significant. Data analysis was conducted using a statistical software program (SAS version 9.4; SAS Institute, Cary, NC, USA).
Results
A total of 54 patients consented to participate and completed the survey (n=54). The majority of the participants were female, non-Hispanic White and US-born. The median age was 51.5 years (range 19-86) and most reported being a high school graduate or less and indicated having public dental insurance. Each demographic variable was compared to the OHL-AQ scores. Only the educational level yielding statistical significance (p=0.03). Age was negatively correlated to OHL-AQ (r=−0.15) but was not statistically significant (p=0.29). Demographic variables and OHL-AQ scores are shown in Table I.
Demographic factors compared to OHL-AQ scores (n=54)
Table II presents participant total OHL-AQ scores with categorization into three levels (low, moderate, high) using two different methods. The “traditional” categories are those derived from Sistani et al. who categorized participants with total scores as low OHL (score of 0-9), moderate OHL (score of 10-11) and high OHL (score of 12-17).16 As this instrument was developed in Iran, differences in the Iranian and US population samples may exist. Therefore, “proposed” categories specific to this study were calculated based on the study median OHL score with subsequent placement of approximately equal groups into the three OHL categories as follows: low OHL (score of 0-11), moderate OHL (score of 12 or 13) and high OHL (score of 14-17). Both OHL categorization schema (traditional and proposed) used in the analysis to answer the study’s research question comparing the OHL-AQ to AAP staging and grading results, yielded statistically significant correlations (<.05). As the OHL-AQ scores decreased, the periodontal stage and grade increased, indicating poorer periodontal health (Table III). The Spearman correlation between age in years and periodontal health stage was 0.27 (p=0.05) and grade was 0.24 (p=0.08).
OHL-AQ scores and categorization into proposed and traditional OHL categories (n=54)
Spearman correlations between proposed and traditional OHL-AQ categories and AAP categories
Discussion
A wide range of OHL and health literacy instruments have been used to measure OHL in populations around the world.4,5,10,22,23 Previously used instruments range from a short six-item, Newest Vital Sign screening survey for reading and numeracy literacy to the extensive REALD-99 consisting of 99 items covering word recognition.24,25 In addition, previous reports in the literature on OHL and periodontal health specifically have used a variety of indicators including bleeding, plaque levels, number of teeth and other Center for Disease Control Guidelines for periodontal health.4,5,10,22 While this study examined functional OHL, which includes the ability to navigate the health care environment in addition to reading instructions and labels, and the association with an individual’s periodontal disease stage and grade in the AAP classification system, the findings support previous research in the area of OHL and health outcomes.
Perhaps this study’s most significant finding was that only OHL-AQ and periodontal health measures reached statistical significance. All single demographic factors and measures of periodontal health were not statistically associated. This is important because the Institute of Medicine (IOM) reported in “Health Literacy: A Prescription to End Confusion,” that limited literacy skills are a stronger predictor of one’s health status than age, income, employment status, education level and racial or ethnic group.26 Conversely, previous studies found statically significant associations between periodontal disease and demographic factors. Holtzman et al. noted severe periodontal disease was associated with older age, male gender, race/ethnicity, lower educational attainment and not having dental insurance.5 Wehmeyer et al. found that race was associated with periodontal health but education and insurance status were not statistically significantly associated with periodontal health.10 Singh et al. found that periodontal health was associated with gender and income but oral health literacy was a stronger predictor of periodontal health.23 While study design and sample size differences may be related to study outcome variations, the results of this study are compelling as they align with the IOM report.26
Statistical results found that both schema for categorizing OHL-AQ results yielded statistically significant results suggesting that the instrument is somewhat independent of cultural context. The OHL-AQ was developed and validated in Iran.16 The instrument was translated into English and found to be valid and reliable.19 Researchers translated the instrument into Hindi and Mandarin with both versions also found to be valid and reliable.20,21 These studies in addition to this study’s results suggest that the four constructs tested in the OHL-AQ categories are appropriate for use in the subsequent studies across a wide range of cultures and languages.
This pilot study had several limitations. Selection bias may be present due to the convenience sample method used to recruit participants. Participants were recruited from the PI’s schedule, making them more likely to be a patient reporting to a recall appointment where they would have received oral hygiene instruction previously, which could have skewed OHL-AQ scores. The OHL-AQ scores could have also been skewed, as these patients were in a system where they already had access to oral health care. There is limited generalizability due to the small sample size, single clinic where data were collected, and nature of convenience sampling. A strength of this study that studies in the past have not included are use of a functional oral health literacy instrument and use of the newest AAP periodontal classification system that represent current clinical practice.
Conclusion
Results from this study identified an association between functional OHL and periodontal health status as indicated by the AAP staging and grading system. Individuals with low to moderate functional OHL had higher levels of periodontal disease indicators. Oral health care professionals should take functional OHL into consideration when providing patient care. Future research should explore the impact of functional OHL on periodontal health in larger patient populations.
Footnotes
Alyssa M. Olson, MS, DH was the 2021 winner of the graduate ADHA/Sigma Phi Alpha Journalism Award sponsored by:

This manuscript supports the NDHRA priority area: Client level: Oral health care (new therapies and prevention modalities).

- Received September 3, 2021.
- Accepted May 16, 2022.
- Copyright © 2022 The American Dental Hygienists’ Association





{kind=link}
{kind=link}