



Abstract
Purpose: Dental hygiene graduates often experience significant psychological stress while transitioning from the educational setting to clinical practice environments. The purpose of this study was to characterize the duration of dental hygiene activities and tasks and explore efficiency within appointments, by students in educational programs.
Methods: Right-handed female dental hygiene students were recruited from two dental hygiene education programs. Each participant was video recorded while providing patient care during 3 sessions, once per term, over 3 consecutive terms. Activities, tasks, and student postures and positions were coded across the patient visit. Descriptive analyses were conducted to characterize overall durations and distributions across each category. Time spent on non-dental hygiene related activities was compared to other durations, as well as across the education/training time points and by patient type.
Results: Fifty-three videos were analyzed from nineteen participants. The average patient visit length was 155.06 ± 35.63 minutes; approximately half the visit was dedicated to instrumentation activities. Nearly 20% of the visit was categorized as activities or tasks unrelated to education or patient care. Although most participants completed the patient visit more quickly by the third time point, the percentage of non-dental hygiene activities did not decrease, and there were no associations between patient category type and the duration of the patient visit.
Conclusion: Patient visits were roughly three times the length of the typical dental hygiene care appointment, indicating a disconnect between training and practice. In addition to spending more time on hand scaling tasks, participants spent a lot of time on equipment setup and interacting with or waiting for faculty members. These findings have implications for improving efficiency in educational settings, particularly to facilitate a successful transition to clinical practice.
Introduction
Dental hygienists are licensed health care professionals who provide important preventative oral health services and treatments for a variety of oral diseases.1,2 There are over 330 Commission on Dental Accreditation (CODA) accredited dental hygiene education programs in the United States, with approximately 6,700 dental hygiene students graduating annually.1,3 The American Dental Education Association (ADEA) requires that dental hygiene education programs teach every clinical skill routinely performed by a registered dental hygienist to competency.4 In addition to general education, basic sciences, and dental science courses, accredited dental hygiene programs require an average of 659 clocked hours of supervised instruction in pre-clinical and clinical practice both within the institution and at extended clinical facilities in the community or in public health settings.2
While current dental hygiene curricula provide a strong focus on the development of basic skills for risk assessment, scaling, polishing, patient education and therapeutic techniques,5 many graduates experience difficulties transitioning from educational settings to clinical practice environments.6-8 This transitional period has been found to be a significant source of psychological stress.9,10 Although numerous research articles have evaluated the clinical component in dental hygiene educational programs through the aspects of ergonomic exposure,11-14 instruments used,15-18 and curriculum design,4 little research exists to examine the overall duration, task breakdown and the time efficiency of clinical procedures conducted by dental hygiene students in educational programs that may contribute to psychological stress and poor transition to clinical practice. Therefore, it is important to investigate the distribution of clinical time in an educational setting, relative to the clinical environment, to help bridge the gap between education and practice.
Foundational understanding of time on task will assist in supporting efforts to identify the disconnect between training hours and clinical practice; closing this gap can thereby reduce physical and psychological stress experienced by dental hygiene students. Measuring and describing positioning, behaviors, and the time span associated with various tasks can provide insight into specific areas of focus for other risk exposure assessment and interventions. Video recording and systematic video coding can serve to provide insight to guide the development of teaching techniques and curriculum design to address the disconnects between education experiences and clinical practice. The purpose of this study was to assess and describe the overall duration, task breakdown, and time efficiency of dental hygiene visits/appointments, performed by students in educational programs.
Methods
An observational study design was utilized to characterize the activities and tasks conducted by dental hygiene students during patient visits across the final three consecutive terms within each student's academic program. Twenty right-handed female dental hygiene students were recruited from bachelor's degree programs at two universities, representing approximately one-third of the available student population. All participants were in the second semester of their junior year at the initiation of the study. The study was approved by the institutional review boards at both universities, all participants provided informed consent prior to data collection, and signed a photo/video release form prior to the initiation of individual recording sessions.
Data collection procedures
Video recordings of participants were obtained during patient visits within the academic clinic on dates and times scheduled by supervisors from each respective dental hygiene program. Each participant was scheduled to be recorded at three different time points approximately three months apart during the final three terms of their academic program. During the video recording sessions, three GoPro cameras (GoPro, Inc.; San Mateo, CA) were arranged in orthogonal positions to capture overhead, front, and lateral views of the participant (Figure 1). Cameras were set up in positions that would not physically obstruct students' performance during the dental hygiene appointment, clearly allowing for identification of the dental hygiene activity or task regardless of student positioning relative to an individual camera. Recording commenced when the student completed all pre-appointment screenings and the patient was cleared for treatment. The recording concluded when the patient left the chair and the student confirmed that the visit was completed.
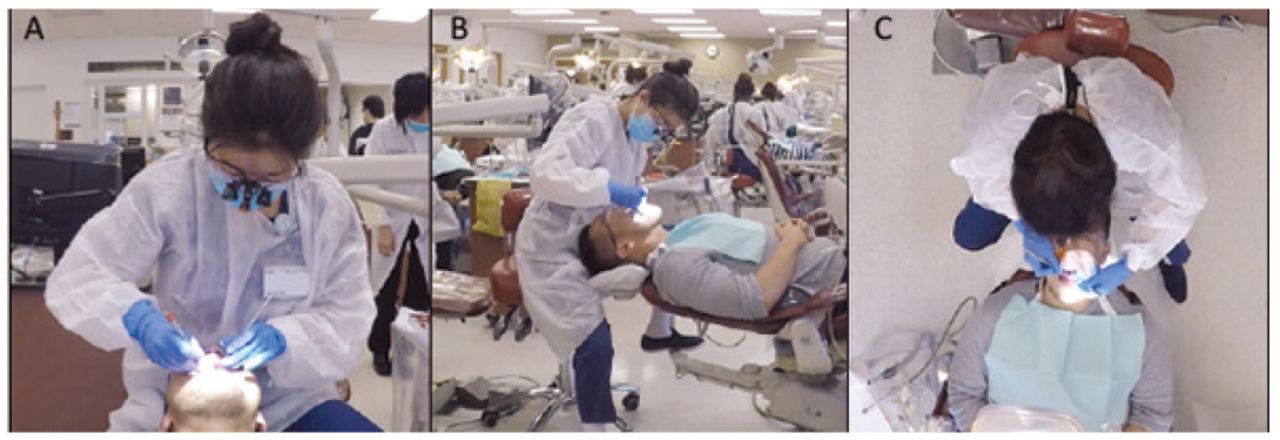
Synchronized video images used to capture and code dental hygiene tasks and activities. Orthogonal camera views from the front (A), lateral (B), and overhead (C) positions.
Patient case type for each recorded visit was obtained for descriptive and comparative analyses. Both institutions used a five-level categorization system for case type (i.e., Type I – Type V); however, Type V was utilized differently between the two programs. Institution one classified Type V as periodontitis that had progressed beyond the severity of a Type IV, whereas Type V at institution two indicated a patient who had initially received treatment classified as Type II, III or IV and was currently in refractory periodontitis. Despite the different use of Type V, both programs recoded patients to higher or lower categories upon patient reevaluation. Following multiple conversations among the research team that included program directors, dental hygiene faculty, and statisticians, a crosslink for classifying patients in a similar manner from both institutions was developed. Patients at institution one who were a Type V were reclassified to Type IV, and patients at institution two were reclassified from Type V to Type I to create one system for both programs. This resulted in a four-level typology roughly indicating increasingly higher difficulty: Type I – gingival disease/gingivitis/refractory periodontitis, Type II – early/slight periodontitis, Type III – moderate periodontitis, and Type IV – advanced/severe periodontitis.
Video coding
Observer XT (Noldus, Inc.; Wageningen, Netherlands, Version 14.1) software was used to code dental hygiene activities and tasks, as well as other contextual components across the duration of each video. A standardized coding manual was developed and validated by an interdisciplinary research team that included experts in dental hygiene and occupational analysis. This manual provided definitions for all variables to be coded, as well as a specific protocol for completing the observational analysis. Three coders were trained in the protocol and calibrated through an iterative process of coding three consecutive videos until between-coder reliability (i.e., inter-rater agreement) was greater than 80% across individual codes.
The coding protocol was conducted in two viewing sessions per video. During the first session, coders first identified which activity was occurring from among five primary dental hygiene student activities including: assessment, patient education, instrumentation, faculty consultation, and other. The other activity code encompassed activities that occurred at any given time during the video that were not clearly part of the other four primary activities. In addition to activities, the coder identified when the student hygienist was sitting or standing and in which clock position the student approached the patient. During a second viewing session, nine different tasks were coded during any video segments when instrumentation activity was identified including: hand scaling, ultrasonic scaling, instrument sharpening, pain management, irrigation, polishing, flossing, applying preventative material, and miscellaneous. As with the other activity, the miscellaneous task code was used when none of the other task codes were clearly applicable during instrumentation time. Brief text was entered into a comment box to describe what was occurring in the video whenever other and miscellaneous were selected.
Data analysis
To be included in final analysis, the recorded patient session had to meet two criteria: 1) the same student conducted the entire patient visit and 2) ultrasonic scaling and/or hand scaling occurred during the appointment. All behavioral data were exported from the coding software and descriptive statistical analysis was performed using Microsoft Excel 2016, Version 3.0 (Microsoft, Inc.; Redmond, WA,). Descriptive statistical measures included mean, maximum, and minimum duration of patient visits, and mean duration, standard deviation and percent time spent in each activity, task, and positioning code. Case series analysis was conducted for participants from whom videos were obtained at all three time points to examine efficiency during patient visits. The duration of hand or ultrasonic scaling tasks, miscellaneous tasks, and other activities were examined across participants by time point and patient category through visual representations of the data. Comments made by the raters to describe miscellaneous and other codes were extracted and examined to further characterize these time codes in the case series analysis.
Results
A final sample size of 19 participants was included for the data analysis (n=19); one of the original participants dropped out of the dental hygiene program during data collection of this study. A total of 53 video recordings, including up to three videos from each participant, met the criteria for inclusion for analysis. The majority of participants were White (55%) followed by Asian (35%), Hispanic or Latino (30%) and other (10%); and had an average age of 23.75 (SD, 3.38) years. The mean duration of all video recordings was 155.06±35.63 minutes, with a maximum duration of 227.46 minutes and a minimum duration of 78.07 minutes. Table I provides the average durations and distribution of time across all observational codes. On average, participants spent over an hour, roughly half of the patient visit, on instrumentation activities. Within instrumentation, participants spent approximately half an hour completing hand or ultrasonic scaling tasks. About 20% of each patient visit was spent on other activities or miscellaneous tasks, the latter accounting for a larger proportion of time than ultrasonic scaling. In terms of positioning, participants spent half of the patient visit away from patient, that is, not directly at the patient's side, and about one third of the visit at the 8, 9, or 10 o'clock positions relative to the patient. Over the course of the entire patient visit, participants shifted clock positions an average of 173 times and switched between sitting and standing an average of 28 times during the patient visit.
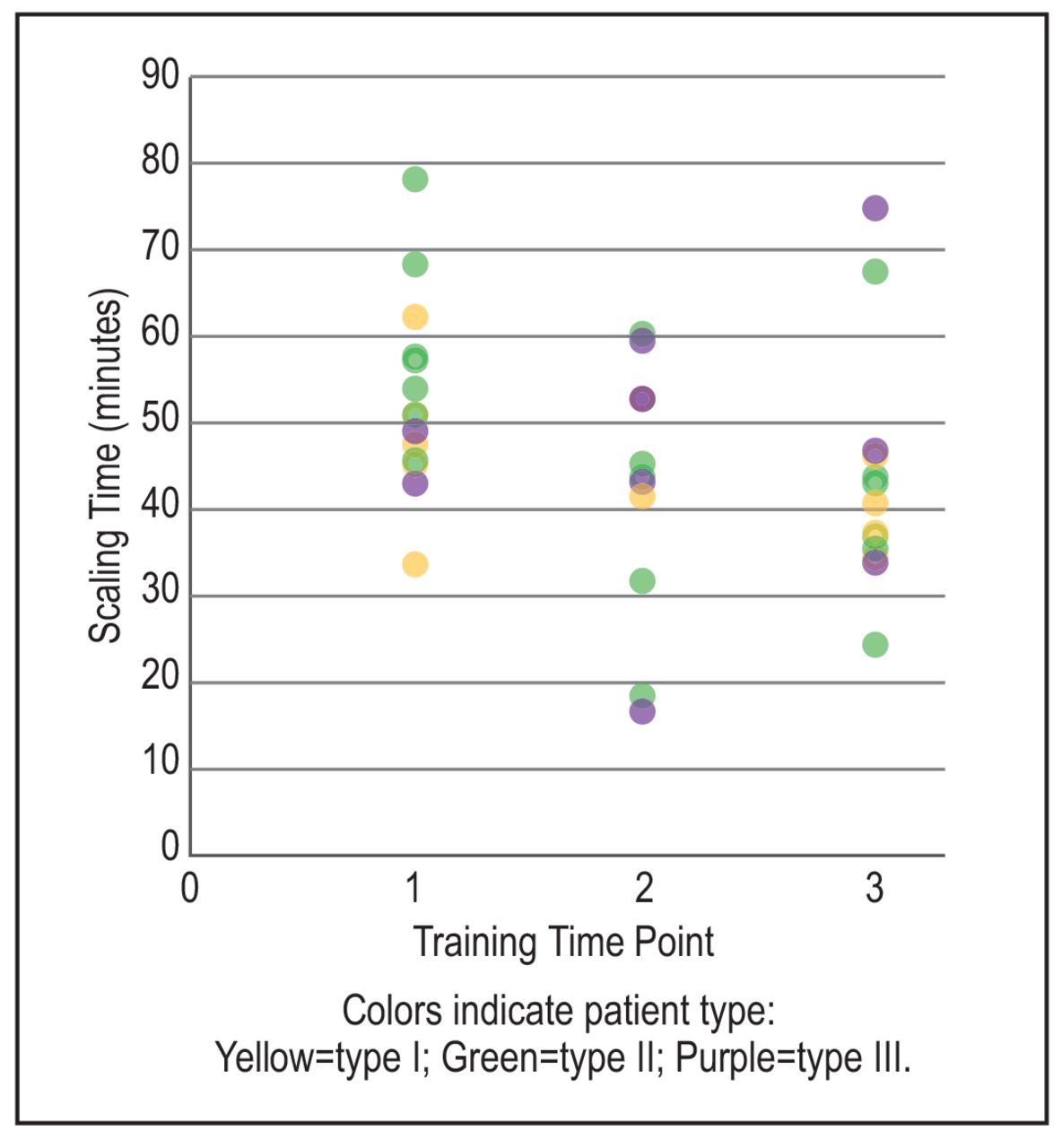
A case series analysis was conducted using data from 14 participants who had all three video recording sessions, resulting in a total of 42 videos. The frequency of patient types I, II, and III within the recorded sessions were 13, 19, and 9, respectively. The patient type in one session was unable to be determined due to lack of documentation, and no Type IV patients were seen by these 14 participants during recorded sessions. The distribution of patient types across each of the three time points by the total amount of hand or ultrasonic scaling time is presented in Figure 2. Across the three sessions, students were observed to spend more time on scaling during the first session as compared to the later sessions, with decreasing average scaling times from 55.07±11.30 minutes, to 44.05±13.89 minutes, and finally to 43.62±13.34 minutes per session. There was no difference in the distribution of patient types within or across each of the three time points, and there was no apparent relationship between the patient type and amount of scaling time.
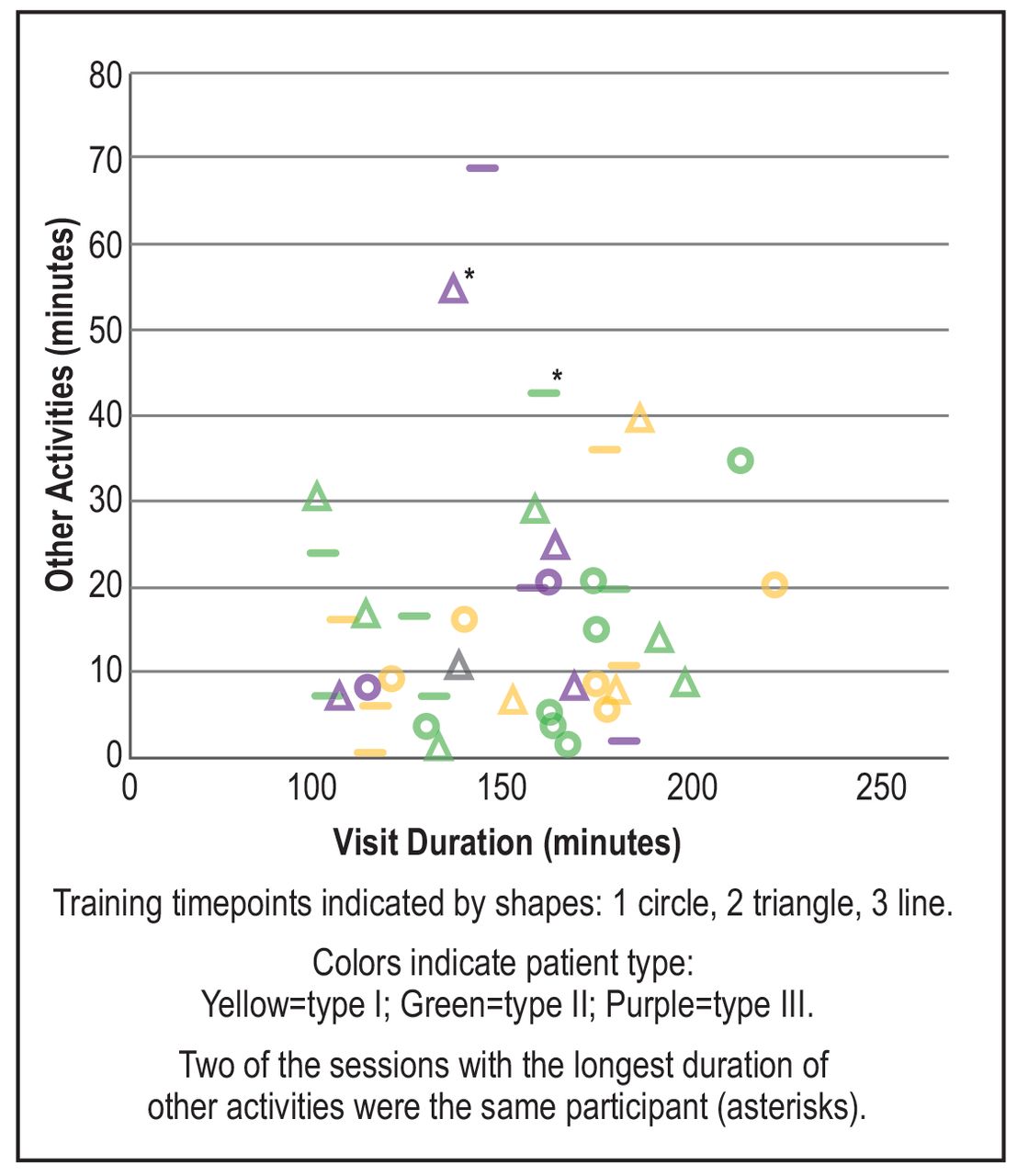
The proportion of other activities to total patient visit time across the three sessions and by patient type are presented in Figure 3. As with scaling time, there was no observable relationship between the total visit time and patient type; however, two of the longest durations of other activity, presented on the vertical axis of Figure 3, were patients of Type III as indicated in purple. Total visit lengths, shown on the horizontal axis, tended to be longer at the first session (circles) as compared to the second (triangles) and third sessions (lines); noted by a higher frequency of circles toward the right end of the chart. By the third session, no patient visit lasted longer than 200 minutes. In contrast, the duration of other activities was not related to the session; instead, most students spent between 5 minutes and 30 minutes doing other activities regardless of the session or patient type. Four videos were observed to have greater than 40 minutes of other activities. Descriptive comments indicated that talking to the patient or faculty member about things unrelated to education or consultation; preparing the workstation or equipment; and being away or out of the camera frame constituted the majority of other activities in these sessions. Two of the four videos with the longest other time were of the same participant who spent the majority of this time talking to the patient or out of view of the camera (denoted by asterisks in Figure 3).
Average duration and overall distribution of time for tasks in a patient visit*
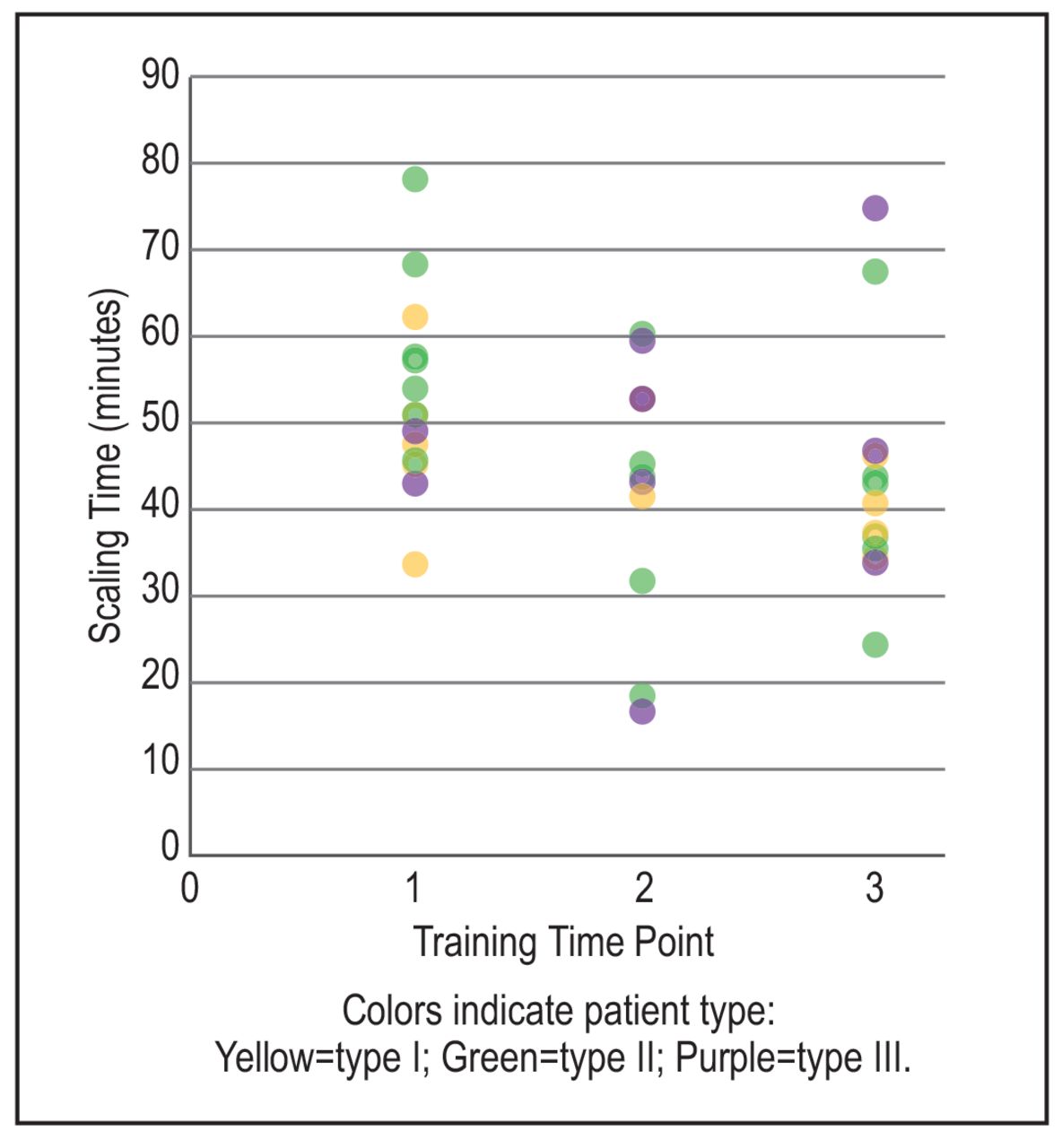
Total scaling time as a function of the time points of data collection across the training period.
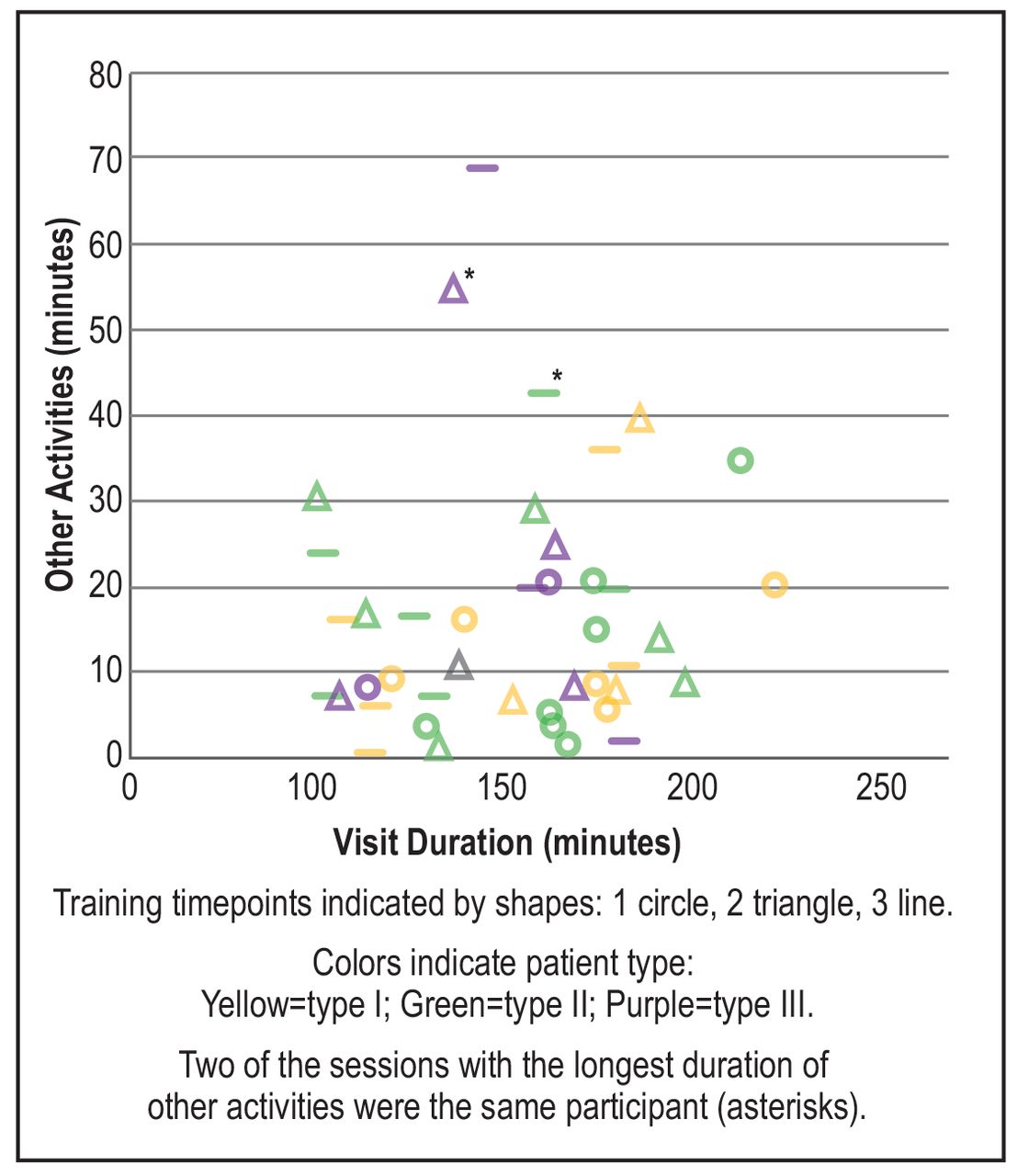
Duration of other activity by the total duration of the patient visit for each recording session.

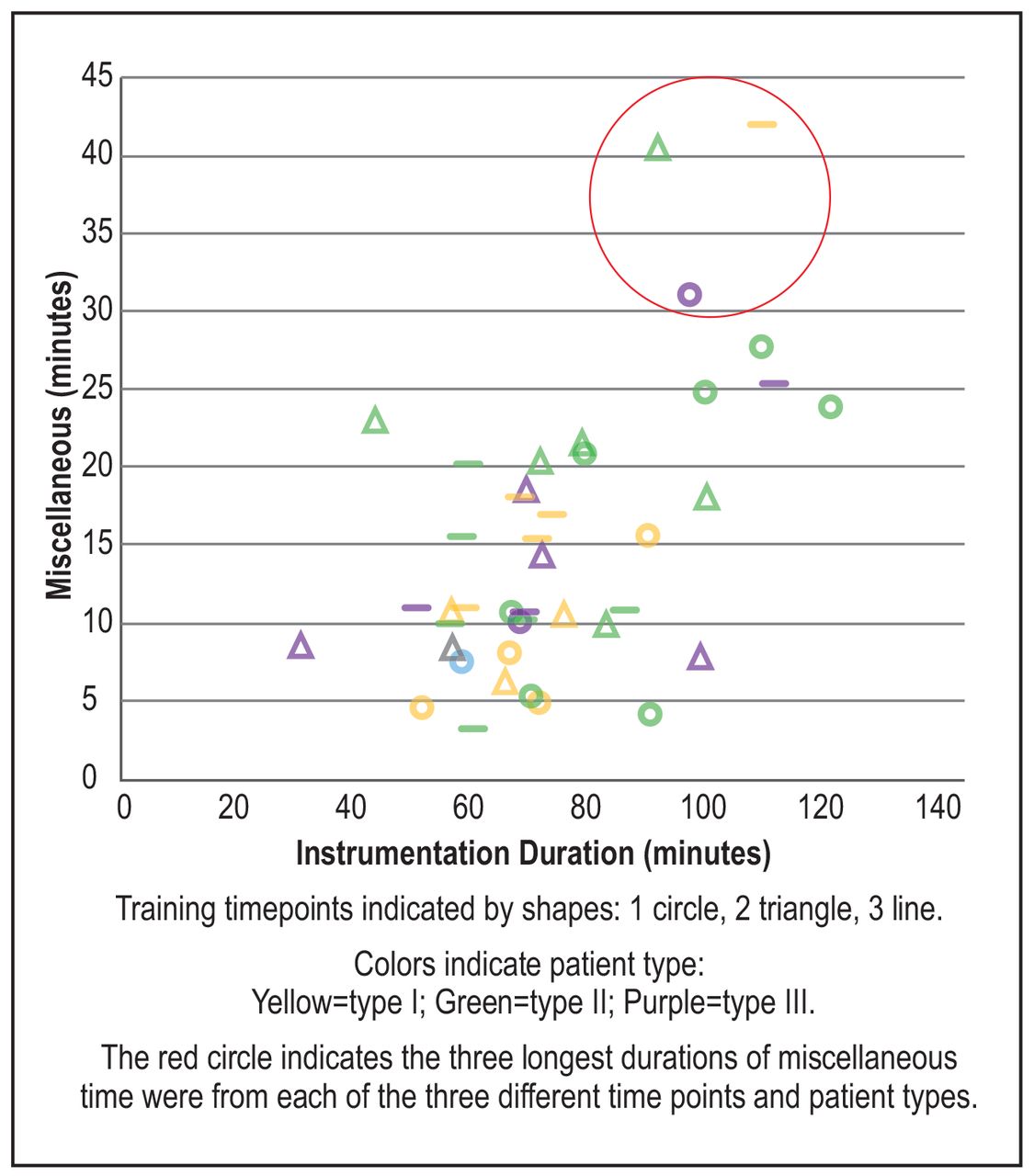
Duration of miscellaneous tasks (vertical) as a function of duration instrumentation time (horizontal) per patient visit.
A similar examination of time spent doing miscellaneous tasks during instrumentation is shown in Figure 4. In accordance with the decreasing trend across sessions for total visit length, instrumentation time plotted on the horizontal axis was longest in the first session (circles) with six participants spending more than 80 minutes as compared to only three and two participants exceeding this time in the later sessions (triangles and lines). While no clear relationship was noted between other activities and total visit length, a strong positive relationship was noted between the durations of miscellaneous tasks and instrumentation time (Pearson's r = 0.56, p <0.01); that is, the longer the instrumentation duration, the more miscellaneous time. Across all data, the majority of sessions had less than 20 minutes of miscellaneous time. The three longest durations of miscellaneous time were from each of the three different time points (i.e., all different shapes) and from each of the three different patient types (i.e., all different colors), indicating that there was not a clear association with the duration of miscellaneous time to training time point or patient type. Despite the lack of clear association, a general decreasing trend in the frequency of sessions, with more than 20 minutes of miscellaneous time, was observed as students progressed in their program (i.e., 5 at time 1, 4 at time 2, and 3 at time 3). Subjective comments from the raters indicated that looking through/arranging instruments, adjusting equipment, preparing for an injection, and talking to a faculty member without clear consultation as part of direct patient care were the most common descriptions of the miscellaneous time.
Discussion
The objectives of this study were to describe the breakdown of various activities, tasks, and behaviors of dental hygiene students while in entry level education programs and to examine the efficiency within and across time and by patient types. Although visit lengths decreased across time, the average duration of a patient visit within the student clinic was greater than 2.5 hours; more than triple the duration typically allotted to a patient appointment in a clinical practice setting.2 Moreover, although the student dental hygienists spent more than an hour on instrumentation activities, hand or ultrasonic scaling accounted for only half of that time. Together, other activities and miscellaneous tasks accounted for more than half an hour or 21% of the total patient visit. While there were no clear or meaningful associations identified among various durations of the overall visit and individual activities or tasks to patient type, downward trends were noted across the training time points for all durations. Of most interest is the strong positive association noted between the duration of miscellaneous time during instrumentation and the total instrumentation time. These data provide insight into areas of opportunity for improving clinical education techniques or curriculum design to identify and minimize causes of inefficiency in dental hygiene education.
Current evidence suggests that the typical treatment time of routine dental hygiene care and periodontal maintenance (PM) appointments in clinical settings ranges from 45 to 60 minutes.1-6 Although prevailing evidence suggests a maximum appointment time of 60 minutes, one recent study found that a PM appointment may require up to one hour and sixteen minutes to ensure provision of sufficient care.19 Unfortunately, during clinical dental hygiene education, students required and were given substantially more time to complete a patient appointment, even during the later and final stages of their education. According to the data in this study, even if faculty consultation time were removed from the total appointment duration, students still spent on average more than 2 hours on each patient visit. In fact, the average time spent on the instrumentation activities alone exceeded the typical clinical appointment duration resulting in a disconnect between education and clinical practice. It is important to work to reduce this discrepancy as much as possible, considering that this disconnect has been found to be a significant source of anxiety among dental hygiene students.9,10
Regarding the distribution of dental hygiene activities and tasks in clinical practice, Yee et al found that registered hygienists spent the most time performing scaling (57%) and other tasks related to cleaning (10%), accounting for approximately two-thirds of the patient visit.20 When the time spent in faculty consultation was subtracted, the time proportions identified by Yee et al.20 were similar to the participants in this study. However, participants this study had a substantially higher percentage of other/miscellaneous time (20%) as compared to the registered hygienists in clinical practice who spent only 6% of their time performing other tasks.20 In fact, within clinical practice only around 3 minutes per visit would be ‘wasted’ time, which is quite low compared to the average of more than 30 minutes in this study of dental hygiene students. Moreover, it is further concerning that a decrease in the amount of other activity time across the training period was not identified, with some students maintaining more than 20 minutes of other/miscellaneous time, even in the later stages of their education. There is a need to better understand what students are doing during these other and miscellaneous times, as these may be key areas for improving efficiency and reducing total patient visit length such that it would better prepare students to transition into clinical practice.
Two primary implications for dental hygiene education were identified based on the findings of this study. First, time requirements for each patient visit could be established as one of the standardized criteria for dental hygiene educators to evaluate student performance during clinical rotations. These time requirements could start similar to what was observed at the beginning of this study and become stricter (i.e., shorter) as the student progresses and increases proficiency. In addition to decreased time allotted for each patient visit, students may also benefit from training on time management skills. This can ensure that students continue to improve proficiency of practice skills while also meeting the time constraints of a busy clinical schedule.
Second, video recording patient sessions may be useful tools and resources within dental hygiene educational settings. Video recording has been used in dental hygiene and dental education for multiple reasons, predominantly as a means of assessing student performance within specific aspects of patient care or dental techniques.21-24 Given the findings of this study, an additional consideration for the use of videos may be to evaluate the efficiency of individual student hygienists and to identify opportunities for improving the process of care that would reduce the length of the visit. In addition to individual student evaluation, video recording may be an effective way for educational programs to detect common inefficiencies across groups of students, that can be addressed through changes in curriculum and training materials, as well as providing a means for identifying organizational or administrative processes that create barriers for students to work more efficiently. Video recordings can be utilized to enhance faculty calibration, and address faculty and student frustrations with faculty inconsistency25-27 by establishing standardized criteria regarding efficiency during clinical rotations.
In addition to these two considerations in dental hygiene education, there are multiple questions to be explained in future research. First, since the use of video may be useful to enhance faculty calibration efforts, it would be beneficial for future research to reveal whether the ratio of clinical faculty instruction has an impact on average time spent per patient visit in educational settings. Second, to identify the sources of the high percentage of other and miscellaneous times indicated in this study, future research may examine factors such as environmental factors in the student clinics (e.g., transient workstations, checking-out equipment) and student motivation levels while participating in unpaid educational clinical settings. Finally, it would be valuable for future research to investigate the average time that newly graduated dental hygienists spend adjusting to a typical schedule in clinical settings, which may facilitate efforts in bridging the gap between education and practice.
This study had limitations. The participant sample was recruited from only two educational programs. Since teaching methods, curriculum, and clinical settings vary across institutions, the findings and implications of this study may not be representative of all dental hygiene educational programs. However, given that all educational programs adhere to similar standards, it is likely that these data may be common to many programs and the implications of student hygienist efficiency has relevance to all programs. While combined data across more than 50 patient visits was robust for providing descriptive findings and generalized trends, the overall sample of videos was not adequate to conduct more robust analyses of individual student differences across time or by patient type. Because the times for video recording with each participant were randomly selected, this observational study did not adequately capture all patient types nor ensure an equal distribution necessary to fully evaluate the impact of patient type or difficulty on activity and task patterns. Also, while it is possible that students altered their behavior due to the awareness of being observed (i.e., Hawthorne effect), video recording is a wildly used method that has a lower probability of a Hawthorne effect than direct human observation,28,29 and the length of time being recorded will likely have minimized any significant effect as students were more apt to forgot that they were even been observed.30 Finally, this study did not evaluate or consider the impact of individual student or patient physical health, mental well-being, or other factors, such as a student's academic standing that may have impacted or been impacted by the patterns of practice. It would be useful for future research to consider the reciprocal impact of student practice patterns on these variables.
Conclusion
Findings from this study indicate that the average duration of patient appointments conducted by dental hygiene students is more than three times the typical treatment time allotted in a clinical setting. Up to 20% of the visit time was spent on activities and tasks that were not related to direct patient care or education, as compared to 6% of the time in the clinical setting. While the duration of the patient visit decreased as students neared the end of their education and training, students continued to spend a high percentage of time on unrelated activities and tasks. Because the duration of the patient visit and extraneous time did not significantly decrease over time, there is concern that clinical education models may not be adequately preparing students for a successful transition to clinical practice. This could lead to high levels of stress and anxiety, as well as prompt the onset of early career burnout or other injuries. Dental hygiene educational programs might consider techniques for encouraging increased efficiency across a student's education. Specific recommendations include the establishment of stricter time constrains during students' clinical sessions and the use of video recording techniques to identify individual or programmatic barriers to efficiency.
Acknowledgements
The authors would like to extend special thanks to Nancy A. Baker, ScD, MPH, OTR/L; Nikki L. Colclazier, MS, RDH; and Joyce Y. Sumi, MS, RDH for their contributions to the development of the initial coding protocol and consultation during data analysis.
Footnotes
Yiyang Fang, MA is a research assistant in the Chan Division of Occupational Science and Occupational Therapy; Kryztopher D. Tung, PhD is a post-doctoral scholar in the Chan Division of Occupational Science and Occupational Therapy; Joan Beleno-Sanchez, RDH, MHS is a clinical instructor and research coordinator, Herman Ostrow School of Dentistry; Jane L. Forrest, RDH, EdD is a professor of clinical dentistry, Herman Ostrow School of Dentistry; Shawn C. Roll, PhD, OTR/L, RMSKS, FAOTA, FAIUM is an associate professor in the Chan Division of Occupational Science and Occupational Therapy; all at the University of Southern California, Los Angeles, CA.
This manuscript supports the NDHRA priority area of Professional development: Education (educational models).
Disclosure
This research was funded in part by the Undergraduate Research Associates Program at the University of Southern California and through a grant from the Centers for Disease Control, National Institute for Occupational Safety and Health (R01-OH010665). The content is solely the responsibility of the authors and does not necessarily represent the official views of the CDC/NIOSH.
- Received October 9, 2019.
- Accepted April 23, 2020.
- Copyright © 2020 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}
{kind=link}