



Abstract
Purpose: Dental hygienists have the potential for filling critical roles in multidisciplinary victim identification teams. The purpose of this pilot study was to evaluate the accuracy of dental hygiene students utilizing dental charting, bitewings, and skull dentitions for the purpose of making identification matches.
Methods: Thirty senior dental hygiene students (n=30) independently viewed an asynchronous online multimedia-based presentation on the procedures used for collecting and recording forensic dental evidence. Following the presentation participants attempted to chart and match three bitewing radiograph sets to three human skull dentitions by correlating matches/exclusions. Immediately following the activity, each student completed a questionnaire rating the difficulty of the exercise, as well as their confidence, and willingness to volunteer as a forensics team member. Descriptive statistics were used to analyze the data.
Results: Of the total sample 36.7% (n=11) reported having prior experiences with dental radiography; while the majority (63.33%, n=19) reported no prior experience. Participants' accuracy scores for dental charting ranged from 91.23% (SD=9.42) to 99.06% (SD=3.60), with no statistically significant difference based on prior experience (p>0.05). The average interrater reliability was 86% (p<0.0001), indicating a high level of agreement with charting skulls and radiographs. No statistically significant differences were found for charting time, perceived difficulty, or level of confidence when comparing experience among the participants (p>0.05).
Conclusions: Regardless of previous experience, dental hygiene students were able to match postmortem dentitions and radiographs with good interrater reliability and did not differ statistically for charting time, perceived difficulty, or confidence. Results suggest dental hygienists can work as effective victim identification team members when educational programs are implemented.
- dental hygienists
- dental hygiene students
- dental radiology
- radiographic interpretation
- forensic odontology
- forensic education
Introduction
Historically, the scientific process of collecting and comparing dental evidence for the purposes of identifying human remains has been utilized with great success.1,2 Comparing antemortem (AM) and postmortem (PM) unique concordant features of the human dentition and surrounding structures is a reliable biometric tool for establishing the legal identification of human remains.2-4 Human teeth maintain integrity during exposure to extreme temperatures and during the process of human decomposition.5,6 Dental charting and comparisons of AM and PM dental radiographic evidence are of central importance, especially in cases of physical damage rendering the body incapable of producing fingerprints or any other form of biometric identification.2,7,8
During previous occurrences of mass fatalities, comparison teams, including volunteer dental and non-dental members, have been utilized to assist in victim identification when the availability of forensic odontologists was limited.9-16 Concerns have been raised regarding the use of disaster victim identification (DVI) team members who are not forensic odontologists, due to lack of standardization in volunteers' formal education, experience, and cognitive bias.4,7,16-18 Wenzel et al. and Zohn et al. suggest that prior to DVI participation, volunteers should demonstrate competence in simulated scenarios.16,17 Several studies have tested the competence of participants with various education and experience to see if there are differences in how they perform with DVI tasks. Participants with formal dental-related education have been shown to outperform participants who have no dental-related education.4,7,17 Having prior dental-related education could be beneficial, especially during mass fatality incidents (MFI) when there is a shortage of forensic odontologists and comparison team members.4,7,17 Pinchi et al. conducted a study comparing the abilities of participants with no dental education (emergency room specialists, legal medicine specialists) to participants with dental education (dental students, dentists, dentists with forensic education, and forensic odontologists), and found participants with dental education had correct answer rates of 85% to 96% and significantly outperformed participants with no dental education with a correct answer rate of 67%.7 Pinchi et al. also found that the accuracy of dental students was similar to dentists who had forensic education; however, forensic odontologists outperformed all participants, especially in very difficult cases.7 The inter-operator variability for the forensic odontologists was also lower when compared to other groups in the study, pointing to reliable consistency in expert opinion among forensic odontologists.7
Dental hygienists can fill critical roles as members of multidisciplinary victim identification and records reconciliation teams.9-13,15 The literature has shown that dental hygienists have been beneficial members of AM, PM, and comparison teams, and have the ability to aid in the management of administrative and miscellaneous duties as they relate to DVI during MFIs.15 Additionally, a 2014 survey of dental hygienists in the United States (n=334) found that 85.6% were interested in DVI as a community service opportunity and of those showing interest, 91.6% indicated intentions for becoming involved.15 Dental hygienists have relevant educational coursework closely interrelated with the curriculum covered in forensic odontology, including anatomy, radiology, embryology, oral pathology, and biomaterials.4,19,20 However, little has been reported in the literature evaluating the effectiveness and reliability of the curriculum, assessments, or in-time trainings for dental hygienists with an interest in forensic-based practice.13,14,16 A review of the literature revealed that curriculum guidelines and best practices for assessment of skills and competencies related to DVI are not well established and lack standardization.2,7,8,17,18 In a study by Sholl et al., forensic odontologists, dental students, and dental hygiene students compared dental radiographs taken from dry skulls to test accuracy of matching influenced by rater experience.4 Dental hygiene students performed better than the dental students, 89.7% versus 85.2% accuracy, however, forensic odontologists performed best with 93.3% accuracy.4 While the authors suggested that dental hygiene students may have performed better than the dental students due to more recent coursework in anatomy and a more acute awareness of tooth morphology, they also concluded that a DVI team with allied dental professionals who have successfully completed discipline related coursework, could benefit DVI.4
Research by Sholl et al. also identified that forensic odontologists with DVI experience performed better than odontologists with only formal education, suggesting that competence for accurate matches may increase with experience.4 This observation was also noted by Pinchi et al. who stated that actual experience in forensic odontology was a better indicator of identification performance when compared to formal education in forensic odontology alone.7 A study of non-forensically trained dental students (n=152) by Sivaneri et al. found that 92.1% of the first, second, and third year students were able to correctly match PM radiographs of heat altered teeth to AM radiographs, and that there were no statistically significant differences in the students' abilities to make matches based on their standing in the program.19 These researchers hypothesized that knowledge and skills gained from formal coursework in dental anatomy and radiology could transfer to dental forensic skills, despite an absence of dental forensics in the curricula.19
When evaluating the amount of time for raters to make forensic matches, two studies found that dental students spent less time completing identification tasks as compared to experienced forensic odontologists, while non-dental professionals took considerably more time when completing identification tasks.7,16 Pinchi et al suggested that a lack of experience with dental radiographic interpretation could explain the increased time taken by non-dental specialists.7 It has also been hypothesized that the increased time required by experienced forensic odontologists may be the result of a more thorough examination conducted with caution, versus haste, in assignment of matches.7,18
It has been suggested that the forensic odontology curriculum for dental volunteers should include simulated disaster events with hands-on activities, and exercises allowing learners the opportunity to attempt identification matches.17 In a study by Wenzel et al., dental students, forensic odontologists, and a radiologist tested pattern recognition of anatomical morphology in unrestored teeth using film AM radiographs and digital PM images from dry skulls.16 In this study, the number of incorrect scores between the experts and the students was found to be low and not statistically significant (p<0.02). Dental students were found to spend less time deciding on matches, but needed more PM images to decide on matches as compared to the experts.16 Wenzel et al. found that the ability of the participants to make matches increased with periapical images as compared to bitewings,16 which conflicts with the findings of Sholl et al.4 However, in a retrospective study of a closed roster airplane crash by Bux et al., while the absence of AM radiographs did not impede identification efforts, the importance of AM radiographs for open disasters with many victims was also cited.21 According to the American Board of Forensic Odontology (ABFO) 2017 Diplomates Reference Manual, PM radiographs are required for most victim identifications and should be relied on as a primary tool, especially when AM radiographs are not available.22 Currently, there is no standard protocol for comparing radiographs when deciding on matches.3,7,18
The lack of standardization among DVI volunteers can make it difficult to determine whether volunteers are competent.17 Dental volunteers involved in DVI activities must be competent in their ability to critically evaluate dental evidence and accurately make conclusions regarding identification matches in a manner consistent with acceptable medico-legal standards.3,18,19 The purpose of this pilot study was to evaluate the accuracy of dental hygiene students in the utilization of dental charting bitewings and skull dentitions for the purpose of making identification matches.
Methods
A convenience sample of senior dental hygiene students (n=30) from Old Dominion University (ODU) were invited by email and verbal announcement to participate in this ODU Institutional Review Board exempt (#1322640-3) study. All participants had successfully completed the same formal coursework of head and neck anatomy, histology, embryology, periodontology, dental radiology, and dental materials; and completed the informed consent letter. Participants then logged into the learning management system (Blackboard, Inc©; Providence Equity Partners, Washington, D.C.) to view a researcher-designed, online multimedia PowerPoint presentation explaining the concepts and procedures for collecting and recording forensic dental evidence and comparisons of the evidence for the purpose of making identification matches. Students viewed the asynchronous presentation independently at their convenience through the learning management system. Time lapses between viewing the presentation and participating in the research project were not tracked. Participants then were asked to chart and match three bitewing radiograph sets to three human skull dentitions by correlating matches/exclusions. At the completion of the charting and matching activity, the participants completed a researcher designed questionnaire rating the difficulty of the exercise, as well as their confidence, and willingness to volunteer as a forensics team member.
Identification procedure
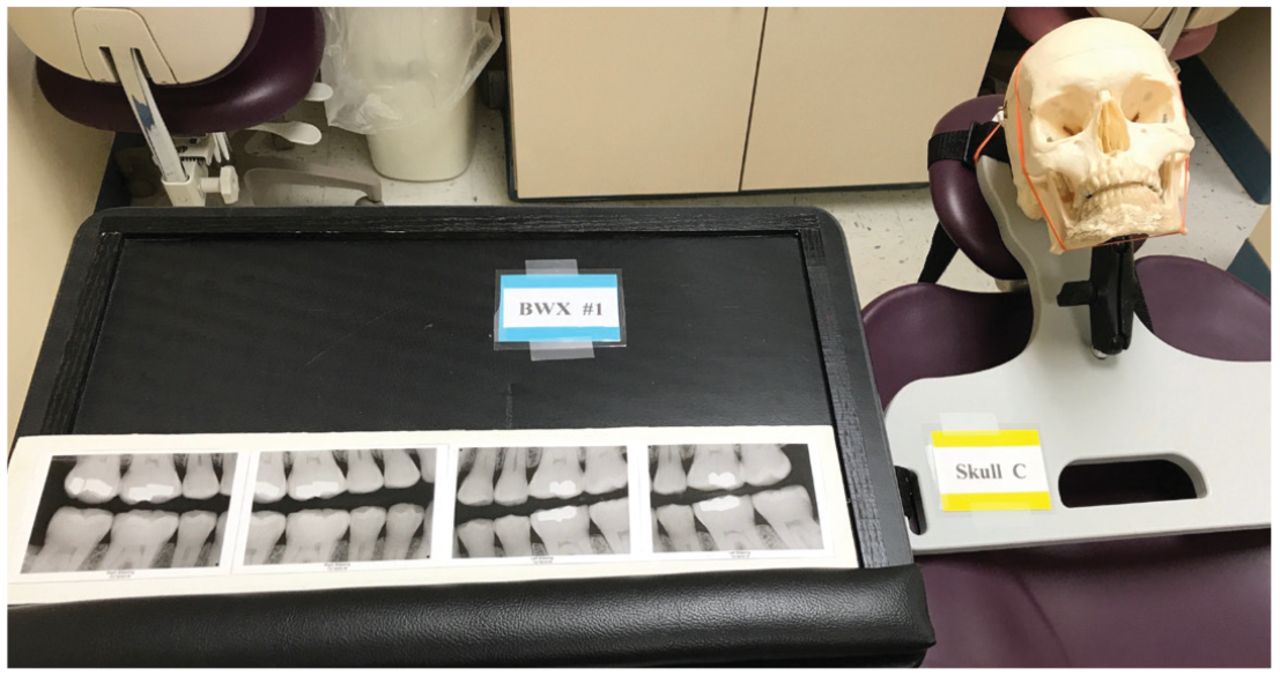
The principal investigator (PI) exposed a set of four horizontal bitewing digital radiographic images on three dry human skulls; the skulls were then mounted to reclined dental chairs. The radiographic image sets were enlarged, printed, and placed on podium stands next to the mounted skulls (Figure 1). The bitewings were randomly labeled 1, 2, 3 and the corresponding skulls were randomly labeled A, B, C. The participants were informed that the bitewings had been mismatched from the skulls. Each participant was provided with six paper dental charting forms (one for each set of radiographs and one for each of the three skulls). The forms were in the same order as the randomized bitewings and skulls, and each participant proceeded in the same order in the room where the study took place.

Bitewing radiographic set randomly mismatched with a skull
Each participant identified the imaged teeth for the three sets of PM dental radiographs and identified the dentition of the three skulls in the following order: skull C, bitewing set #1, skull A, bitewing set #2, skull B, bitewing set #3. Participants were asked to identify each tooth in the image as: present, missing, or as having a dental restoration. They were then asked to do the same for each tooth in the three human skulls. Finally, the participants were asked to match each bitewing radiographic set with its corresponding skull based on the dental evidence recorded on the six dental charting forms. Participants were not asked to qualify their answers for matches based on categories and terminology for identification as required by the ABFO (e.g. positive identification, possible identification, insufficient evidence, exclusion).
Each participant was timed while completing the dental charting and deciding on identification matches however this was unknown to the participant. Entry to the study operatory was limited to one participant at a time and participants were allowed to revisit the bitewing sets and skulls to check their answers during the session. At the conclusion of the identification exercise, participants completed a researcher-designed, paper questionnaire consisting of twelve items regarding the difficulty of the tasks, their level of confidence, and their feelings about volunteering as a forensics comparison team member in the future. Participants indicated whether they had previous work experience with exposing and interpreting dental radiographs. A follow-up question for positive responders inquired whether they felt that their formal dental hygiene coursework helped to improve their skills with exposing and interpreting radiographs, recognizing dental restorations, and recognizing anatomical differences in teeth and bone. Prior experience, or the lack thereof, was utilized to conduct the interrater reliability comparison, and to investigate whether prior experience influenced accuracy, charting time, perceived difficulty, and confidence while making identification matches.
The study's methodology was supported by the experi-mental design by Sholl et al., which included forensic odontologists, dental students, and dental hygiene students who attempted to make matches with AM and PM bitewings and periapicals from dry skulls and also suggested that the type of radiograph did not affect the accuracy when used as a matching tool.4 The research design also took into consideration the amount of time participants would devote to the identification exercise between classes and other obligations. Therefore, the exercise limited the number of radiographs and skulls to three each, to avoid overwhelming the participants with an activity that would be too time consuming. The amount of time required for subjects to complete research activities has been considered in other studies along with a consideration of not causing mental fatigue for participants.
Statistical analysis
The participants' demographic information, their accuracy grades for dental charting, as well as their levels of perceived difficulty and confidence were summarized and compared between level of experience using the Chi-square test or the Fisher's Exact test for categorical variables, and the Student's t test for continuous variables. Level of experience was a binary variable, representing whether a participant had experience with exposing and interpreting dental radiographs prior to entering dental hygiene school. Categorical data were presented as frequencies and proportions, whereas continuous data were presented as means and standard deviations. The %MAGREE macro for multiple raters with multi-categorical ratings, was used to compute the Kappa statistics to test charting agreement among all participants.23 All statistical analyses were performed using SAS 9.4 (SAS Institute, Inc., Cary, NC), and statistical significance was determined using an alpha level of 0.05.
Results
A convenience sample of senior dental hygiene students agreed to participate and completed the simulated dental charting and identification matching activity and post-questionnaire. All participants were female (n=30) and a little more than one-third (36.67%, n=11), reported having at least one year of work experience with exposing and interpreting dental radiographs prior to entering the dental hygiene program. Participant demographic data is shown in Table I.
Sample demographic characteristics (n=30)
The participants' mean accuracy scores for the dental charting of bitewing radiographs ranged from 91.23% (SD 9.42) to 95.49% (SD 7.20), and ranged from 93.94% (SD 7.70) to 99.06% for charting the skull dentitions. No statistically significant difference was found between experienced and non-experienced participants in terms of accuracy for dental charting the bitewing radiographs or skull dentitions (all p>0.05). Additionally, all participants successfully matched the radiographic sets and corresponding skulls with 100% accuracy. The participants' dental charting accuracy is shown in Table II.
Mean accuracy for dental charting of skulls and bitewing radiographs
Kappa statistics for assessing dental charting reliability agreement between participants ranged from 0.81 to 0.89 for the three sets of radiographs, and from 0.76 to 0.96 for the skull dentitions; all were statistically significant (p<0.0001), indicating stronger agreement than can be expected by chance (Table III). Overall, there was an 86% agreement between all participants in charting present, missing, and restored teeth for both bitewing radiographs and skull dentitions. Participants used a minimum of 12 minutes and a maximum of 46 minutes to complete the activity and post-questionnaire, with an average time of 19.23 minutes (SD = 6.61). Although not statistically significant (p = 0.351), the trend of the data showed the average charting time was higher among non-experienced as compared to experienced participants [20.11 min (SD = 7.77) vs. 17.73 min (SD = 3.74)].
Kappa statistics for interrater reliability for dental charting of skulls and bitewing radiographs
Students were asked to rate the level of difficulty they experienced while: 1) dental charting the radiographs, 2) dental charting the skull dentitions, and 3) matching the radiographs to the corresponding skulls. No statistically significant difference was found in levels of perceived difficulty between the experienced and non-experienced participants (p>0.05 for all). However, over half of the participants reported experiencing a slight level of difficulty while dental charting the bitewing radiographs (n=16, 53.33%), and while dental charting the dentitions of the skulls (n=18, 60%). However, a majority (80%, n=24) reported slight or no difficulty in matching the radiographic image sets with the corresponding skulls. Participants were also asked about their perceived confidence regarding their accuracy with matching the radiographs to the corresponding skulls. Although not statistically significant (p = 0.8498), perceived confidence levels were slightly higher among participants with prior experience as compared to those without prior experience (81.82% vs. 78.95%, respectively). When asked about their willingness to volunteer as a member of a forensic comparison team in collaboration with forensic odontologists, the majority (93.33%, n=28,) indicated that they would consider it. The participants' perceived levels of difficulty, and confidence, along with their reported interest in dental forensics is shown in Table IV. When participants with previous experience in radiography were asked whether or not their formal dental hygiene coursework helped to improve skills, perceived improvement was indicated in the following areas: exposing radiographs (100%, n=11), interpreting radiographs (90.91%, n=10), recognizing dental restorations (100%, n=11), and anatomical differences in teeth and bone (90.91%, n=10).
Discussion
This pilot study assessed senior dental hygiene students' ability to apply knowledge gained during their entry level dental hygiene curriculum, to match PM dental radiographs with human skull dentitions within a researcher-designed dental forensic scenario. All participants were able to match radiographic sets with the corresponding skulls with 100% accuracy and scored 91% or better when charting the dental evidence. Findings from this study are comparable to a previous study in which dental hygiene students were found to have an almost 90% accuracy rate.4 The high level of accuracy demonstrated by these participants can be used to support efforts aimed at incorporating dental hygienists into multidisciplinary teams with forensic odontologists during MFIs. Furthermore, these results support the need for including forensics as part of dental and dental hygiene education as identified by Sivaneri et al.
Descriptive statistics of levels of perceived difficulty and confidence
The majority of participants (93.3%) indicated that they would consider volunteering as part of a MFI forensic comparison team, which concurs with a previous study by Bradshaw et al., where almost 92% of U.S. dental hygienists indicated willingness to serve in this capacity.15 This pilot study helps fill gaps in the literature by assessing the skills obtained from a bachelor's degree dental hygiene program curriculum which could be successfully applied to identification match scenarios, and demonstrates the effectiveness of including this source of willing volunteers into future forensic comparison teams.
Inclusion of hands-on activities of matching skull anatomy with radiographs can be incorporated into the radiology course curriculum in dental hygiene programs. These activities would allow students the opportunity to build the conceptualization skills to better understand how unique anatomical features produce unique images. This pattern recognition skill has been identified by several researchers as one that could be learned through simulated activities similar to the design of this pilot study.16,17 Pinchi et al. supports the inclusion of comparative activities for dental radiology coursework in forensic training, stating that it increases the performance of volunteers with dental education over non-dental volunteers.7
No statistically significant differences were found in the charting or identification match skills between participants with and without prior radiography experience in this pilot study. It is possible that the two semesters of radiology and three semesters of clinical curriculum completed by the participants included enough coursework so that the skills of non-experienced participants were comparable to experienced participants; yielding high accuracy for both. The vast majority of the participants in the pilot study reported slight to no difficulty when charting the radiographs, charting the skulls, and deciding on the matches. Considering these results, it is not surprising that the majority of the participants reported being very confident (80%) or moderately confident in their performance (20%).
This pilot study had limitations. The convenience sample was small and limited to one dental hygiene baccalaureate-degree granting institution. The pilot study was researcher-designed and not in complete alignment with other dental forensic study designs. Repeating previously published dental forensic studies is difficult for several reasons. There is a lack of standardization among the designs of dental forensic studies regarding the materials, methods, and participants. Second, dental features of the radiographs and skulls will be unique to each study. Third, the inclusion of dental hygienists in dental forensic research studies has been lacking.
The current study was limited to PM bitewing sets and did not include AM radiographs. This could be a limitation when considering that AM radiographs and a full mouth series of radiographs would also provide additional detail useful in forensic dentistry. Wenzel et al. also found that the ability of the participants to make matches increased with periapical images as compared to bitewings.16 Some studies have been designed without AM radiographs, as they are not always available for forensic cases as cited in the ABFO Diplomates Reference Manual22 and by Bux et al.21 This supports the rationale for designing research studies requiring participants to rely on PM radiographs as the primary identification tool, which was a feature of this pilot study.
Another limitation was participants did not include qualifications of their answers to the identification matches to indicate degrees of probability. Not using qualification categories of “positive identification, possible identification, insufficient evidence, and exclusion,” may have impacted the generalizability of the results. According to Pinchi et al, confidence reported by forensic odontologists relates to the rater's assignment of the likelihood of the positive match as it relates to a “probable” degree, rather than actual match accuracy.7 Therefore, the cognitive bias of the participants cannot be compared to findings of forensic odontologists from other studies.
Dental hygienists have shown evidence of being interested and committed to supporting forensic dentistry in their communities when the availability of forensic odontologists is limited.15 Still, more evidence of the effective utilization of dental hygienists as a supportive adjunct for DVI is needed. Future studies should include large sample sizes of dental hygienists from areas throughout the United States, a variety of simulated forensic scenarios, and include students and graduates from a variety of dental hygiene education programs.
Conclusions
Results from this pilot study demonstrate that dental hygiene students were able to match postmortem skull dentitions and radiographs with good interrater reliability and that they did not differ statistically for charting time, perceived difficulty, or confidence regardless of previous experience in dental radiography. A high level of agreement and accuracy among raters for dental charting and matching indicates dental hygienists are knowledgeable and well suited to work in a forensic-based capacity. Education in records comparison can help prepare dental hygienists for activities related to dental forensic victim identification. More research is needed to utilize the skills of dental hygienists related to dental forensics. Published reports of pedagogy used to teach forensic dentistry could aid future research in developing study designs to test educational best practices.
Footnotes
Brenda T. Bradshaw, RDH, MSDH, is an assistant professor; Ann M. Bruhn, RDH, MSDH, is associate professor and Dental Hygiene Program Chair; Tara L. Newcomb, MSDH, is an associate professor and Director of Clinical Affairs; all at the Gene W. Hirschfeld School of Dental Hygiene, Old Dominion University, Norfolk, VA.
Hadiza Galadima, PhD, is an assistant professor and biostatistician at the School of Community and Environmental Health, Old Dominion University, Norfolk, VA.
This manuscript supports the NDHRA priority area: Professional development: Education (Educational models).
- Received September 23, 2019.
- Accepted January 12, 2020.
- Copyright © 2020 The American Dental Hygienists’ Association





{kind=link}