



Abstract
Purpose: The purpose of this study was to evaluate the effects of using mobile text messages and a novel floss holder as compared to finger flossing or the novel floss holder alone, on the psychological, behavioral, and clinical parameters of patients with gingivitis.
Methods: A total 165 adults were assessed for eligibility and 144 met the criteria for randomization into three groups: Finger Floss (FF, n=43), Novel Floss Holder (NFH, n= 40), and Novel Floss Holder plus Text Messages (NFH+TM, n= 61) following a dental hygiene consultation appointment. Gingival bleeding points were measured on probing (BOMP) at baseline and four months later by a calibrated dental hygienist, blinded to the experimental groups. Participants also self-reported their oral hygiene behaviors, and indicated psychological determinants of behavior change prior to the dental hygiene consultation and at four months. Descriptive statistics and repeated measures analysis of variance (ANOVA) were used to compare groups over time.
Results: Two subjects dropped out of the study making the total number of participants 142. At the four month follow-up, the NFH group and the NFH+TM groups demonstrated significantly higher levels of self-reported flossing, action self-efficacy, intention, action planning, and action control. The NFH+TM group showed lower levels of bleeding and higher levels of oral hygiene and recovery self-efficacy than the other groups, in addition to higher levels of maintenance self-efficacy as compared to the FF group.
Conclusions: The use of a novel floss holder, NFH, was shown to improve the behavioral and psychological determinants of periodontal health four months after introduction of the device. However the clinical measures of BOMP only improved significantly when used in conjunction with text messages (NFH+TM). The use of a consciousness awareness technique,TMs, in combination with a novel device, may help patients to reach therapeutic objectives and contribute to the management of periodontal pathologies such as gingivitis.
Introduction
Mechanical control of biofilm is the primary therapeutic strategy for preventing gingival diseases.1,2 Toothbrushing plays an important role to that end and is the most commonly used means of controlling plaque2 but toothbrushing alone is not sufficient for efficiently reaching into interdental surfaces.3 Recent literature reviews have identified interdental brushes (IDB) as the most effective interdental cleaning devices.3,4 However, some limitations have been noted for IDB, as several shapes and sizes are required and most of the interdental spaces in the anterior teeth are too narrow for their use.3 Additionally, other researchers have drawn attention to the scarcity of well-designed studies demonstrating the relative clinical value of flossing, arguing that it may be premature to discontinue the use of floss.5 A more recent systematic review mentions that both floss and interdental brushes may contribute to reducing gingivitis.4 Many researchers are advocating for oral health care professionals to change their mindset from flossing to interdental cleaning. Selection of the best interdental cleaning device should be made according the dimensions of the embrasure space combined with patients' skill levels and motivation, not based exclusively on the comparative results of efficacy.3-5
Individuals often fail to exert control over their own behavior despite being motivated to do so,6 and this self-control can be even more challenging when routine behaviors are involved, such as those related to oral hygiene. Some models of health behavior change, such as the Health Action Process Approach (HAPA),7 take volitional or self-regulatory aspects of behavior into consideration. According to the HAPA, a change in health behavior is the result of a motivational phase where individuals form an intention to act. However, it also involves volition, the cognitive process by which an individual decides on and commits to a particular course of action, as well as a post-intentional phase where the individual plans how to put their intentions into practice and maintain their behavioral changes.6-9 When compared to other social cognitive models, the HAPA has been shown to be a good predictor of oral hygiene behaviors.8,9 The HAPA is illustrated in Figure 1.

The Health Action Process Approach (HAPA)7
It is also known that individuals thrive on novelty and challenge, seeking new experiences and stimulating activities.10,11 Under most theories of motivation, both curiosity and a personal sense of control influence readiness and motivation to initiate behavior and expend effort.12 This is particularly important when approaching new situations, such as using a novel floss holder or receiving text messages about oral health issues. Floss holders have a long history of use, with studies showing benefits for patients lacking the dexterity to use finger flossing, and in helping patients establish a long-term flossing habit as compared to finger flossing.13,14 New or novel floss holders (NFH) may be a way to increase curiosity, control, and flossing frequency, thereby fostering oral hygiene efficacy.
One method of disrupting undesired habits, such as failing to control plaque biofilm in interdental spaces, is by bringing habitual behavior and its context to conscious awareness.9 Consciousness-raising for health behavior may be facilitated by mobile digital technologies, which provide the opportunity to display habit-disrupting cues.15 Mobile text messages (TM) may offer an opportunity to disrupt an undesirable habitual behavior by keeping a goal salient or by bringing the goal back to working memory at an appropriate point in time. Moreover, according to a recent systematic review and meta-analysis,16 the use of mobile health interventions has been shown to positively influence communication between patients and providers, facilitating patient-centered healthcare. In the same vein, TMs have also been shown to foster social support mechanisms.17
It is not known whether the use of a consciousness awareness technique such as a TM in combination with a novel device such as the NFH, could lead to a new behavior and ultimately improved oral health. The purpose of this randomized controlled trial was to investigate whether the effect of using a NFH would improve compliance and help to develop positive health behaviors to promote gingival health and to investigate the effect of TMs on increasing the sustainability and clinical efficacy of those behaviors between dental hygiene care appointments.
Methods
Sample selection
Interested participants were recruited among the local urban community, through newspaper ads and advertisements in local shops in Caldas da Rainha, Portugal. A total of 165 patients were initially assessed, however 21 patients failed to meet the inclusion criteria (age 18 years or older, having 20 teeth with a minimum of five teeth per quadrant, periodontal pockets >3mm and Bleeding on Marginal Probing >0.5, non-smoker, not pregnant, not in orthodontic treatment and not having removable partial dentures). A dental hygiene consultation appointment including professional mechanical plaque removal (scaling and polishing) and oral hygiene instruction was delivered to participants by an experienced dental hygienist in two private dental clinics; the clinical trial was conducted over a span of four months with two assessment points. Data confidentiality and anonymity were assured and the ethics committees of the University of Lisbon and the Escola Superior de Saúde de Portalegre approved the clinical trial (Ethics Committee Doc. No. 6/14). The study was registered at the ClinicalTrials.gov database (NCT03120559).
Procedures
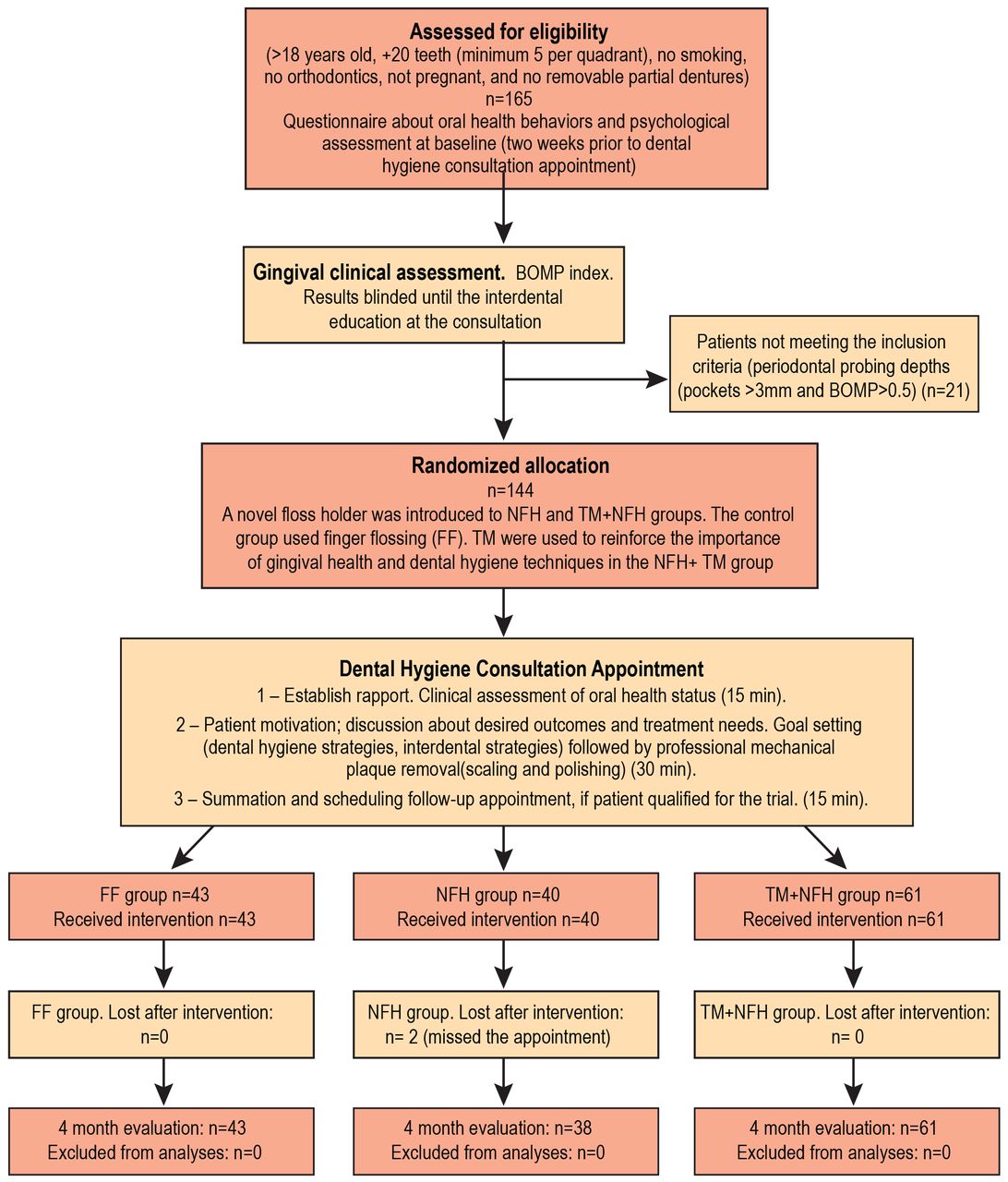
Participants meeting the inclusion criteria, with the exception of the periodontal status, completed an online informed consent and a questionnaire with items addressing psychological determinants and oral health behaviors. Two weeks later, the gingival condition, Bleeding on Marginal Probing, (BOMP)18 was evaluated by the experienced dental hygienist. After the bleeding index values were collected, each qualified participant was allocated, via computer-generated random sequencing, into one of three groups: Finger Floss (FF), Novel Floss Holder (NFH), or Novel Floss Holder plus Text Messages (NFH+TM). Next, a dental hygiene consultation appointment was provided by the experienced dental hygienist who was blinded to the participant groups. The 60 minute dental hygiene appointments (professional scaling, polishing, and individualized oral hygiene instructions) were free of charge. Each session included behavior change techniques,20 that were the same regardless of the participant's clinical trial group. Individualized oral hygiene instructions were delivered thorugh verbal and practical demonstration (tell, show, and do) with the help of a hand mirror. The same BOMP assessments were performed and recorded four months later and the participants were asked to complete the post-questionnaire addressing psychological determinants and oral health behaviors. Items regarding TMs were added to the post-questionaire. A flow chart of the study is illustrated in Figure 2.
A novel floss holder (GumChucks®; Oral Wise Inc.; Calabasas, CA, USA) was provived to the participants in the NFH and NFH+TM groups during the dental hygiene consultation appointment. The NFH resembles miniature nunchucks, featuring disposable tips connected by a piece of dental floss. The two-handle system is designed to increase dexterity and control, facilitating the recommended “C” shape with the floss. The FF group was provided a waxed, flavor free floss (GUM, ButlerWeave®; Sunstar Europe; Etoy, CH).
Subjects assigned to the NFH+TM group were informed about how the messaging system would operate and asked to provide their mobile phone number in order to receive the TMs, at the rate of one per week, over the next four months. Messages consisted of approximately 140 characters. Content related to oral hygiene and gingival inflammation and was designed to include characteristics described as important for improving efficacy and compliance, such as assertiveness, comprehensibility, originality, individualization and humor.19 The TMs were pretested to an independent sample of 40 adults in order to evaluate their perceptions of the messages. A sample TM stated: “It is impossible to sneeze with your eyes open, BUT it is possible to take care of the gums between your teeth, even if it has been some time without doing so. You'll see! If you can, your gums will be healthy again. (Dental hygienist's name)”
Assessments
Gingival condition was assessed using the BOMP index, as described by Van der Weijden et al.18 In this index, bleeding is scored during 30 seconds of probing using a 3-point scale, from 0 to 2 (0 = no bleeding, 1 = pinprick bleeding and 2 = excessive bleeding). Moderate gingivitis was defined as having at least 40% of the test sites showing bleeding on probing at the initial screening.18 A healthy BOMP score was considered to be equal to or less than 0.5, or fewer than 25% of sites bleeding on marginal probing.21 Four months after the initial appointment, the same procedure and measures were used. One-fifth of the patients were re-evaluated for BOMP by a second dental health professional blinded to the assigned groups, to determine inter-rater agreement at baseline and four months. High agreement was found between the two dental health professionals who evaluated the BOMP (κ=.718; 95% CI, .50; .94, p< .001).
Participants were asked two questions regarding brushing and flossing habits using a 5-point scale, 1) not using, 2) barely, 3) once a day, 4) twice a day, 5) more than twice a day, in order to evaluate their oral hygiene habits. Scores for brushing and flossing were calculated and a composite (mean) score for oral hygiene was also computed. Satisfaction with the NFH was assessed by: “How do you rate the use of the NFH? Response options included: “They are easy to use and I like them, I like them, but they are difficult to use, I don't like them, and They are a waste of time”.
Measures were adapted for oral health behaviors from previous studies using the HAPA model22 using a seven-point Likert-type scale ranging from 1)“totally disagree,” to 7) “totally agree.” Evaluation of the TM, according to the overall interest (comprehensibility, interest, and relevance) and usefulness, was measured by adapting a 10-item scale22 with responses using a five-point Likert scale. A four-point scale ranging from 1) “Less than one message per week” to 4)“More than three messages per week” was also used to determine the frequency at which participants were willing to receive more messages. In order to inquire regarding how participants reacted to receiving the TM, a five-point scale was used, ranging from 1) “Ignored it” to 5) “Read it immediately.”
To ensure that the effects on gingival health were not dependent on the dental hygiene consultation appointment, a four-item checklist (introduction and diagnosis, explanations, hygiene goals, and clinical procedures) was used. In order to verify whether the consultation script was similar for all the patients, the fidelity of the intervention was checked by two other oral health professionals for more than one-fifth of the randomly selected consultion appointments. In 80% of the checked appointments, 100% fidelity was obtained; the fidelity was above 90% for the remaining 20%.

Flowchart of randomized control trial
Data analysis
A dropout analysis and a randomization check was performed through multivariate analysis of variance (MANOVA) for the psychological determinants, behavior, and clinical gingival outcome; ANOVA and Chi-square tests were used to compare continuous and categorical variables, respectively. Distribution normality (Shapiro-Wilk) and variance homogeneity (Levene's test) were verified for all outcome variables. To compare the three groups at the four-month follow-up, mixed between/within-subject repeated measures ANOVA with each intervention group (FF, NFH, NFH+TM) times the assessment time (baseline vs. four months) were computed. Whenever differences of interest were found at baseline in outcome variables, the same analysis was repeated introducing baseline scores as a covariate.
Results
Dropout analysis and randomization check
No significant differences between the longitudinal sample (n=142) and those who dropped out (n=2) were found in any baseline sociodemographic variables. However, a difference was identified in intention, which was lower among those who dropped out (M=4.00, SD=4.24) as compared to those who remained in the study (M=6.00, SD=.86), p=.003. No differences across the three groups were found at baseline in relation to sociodemographics, frequency of flossing, tooth brushing, or BOMP, nor on most of the psychological determinants (p>.10). Exceptions were found for intention, maintenance self-efficacy, and coping planning. At baseline, intention was significantly higher in the FF group than in the NFH+TM group; maintenance self-efficacy was significantly higher in the FF and NFH groups than the NFH+TM group; and coping planning was higher in the NFH+TM than the NFH group (all at p<.05).
Descriptive statistics
Descriptive demographic data for the sample are presented in Table I. Participants' daily frequency of flossing was low at baseline (M=1,7, SD= .79); the majority either never or barely used dental floss. Reference to other interdental devices for dental plaque control was low, with only 2.8% of individuals using interdental brushes. However, the majority of the sample brushed their teeth twice a day. The initial level of BOMP for the entire sample was relatively high, with an average of 60% bleeding points. The majority of the NFH+TM sample considered the messages useful for the new behavior and rated the TM very positively overall in regards to comprehensibility, interest, and relevance. Regarding the use of the NFH, 69% liked it after four months of usage, although around a third of participants reported some difficulties in using it. Oral hygiene behaviors at baseline and 4-months are shown in Table II.
Sample demographics (n = 142)
Intervention effects on clinical and behavioral outcomes
Values for interaction between group and time, and for the main effects of group and time at baseline and at the four-month follow-up, are presented in Table III. Significant interactions between the intervention group and time were obtained for BOMP (F [1,139]=262.95, p<.001), flossing (F[1,139]=134.74, p<.001), and oral hygiene (F [1,139]=103.07, p<.001). While no differences between the groups were found for any of these three outcomes at baseline, the NFH+TM group presented a significantly lower BOMP values (i.e., 0.6; SD=.32) and a significantly higher level of oral hygiene than the other two groups at the four-month follow-up.
Oral hygiene behaviors at baseline and 4-months (n =142) NFH
The average BOMP score in the NFH+TM group decreased from 1.2 (SD=.35) at baseline, to 0.6 (SD=.32) at 4 months, which corresponds to the decrease in bleeding sites at baseline from 60% to 30%, at 4 months. While the number of bleeding sites in the NFH+TM group was lower than the FF and NFH groups, bleeding sites in the NFH group were not significantly lower than the FF group.
The NFH+TM group reported higher frequency of flossing at the four-month follow-up (67% of the individuals started using floss daily) as compared to the NFH group (50% started to use it daily), demonstrating a higher flossing frequency than the FF group (37% started to use it daily).
Intervention effects on psychological determinants of oral hygiene
Interaction effects between intervention group and assessment time were obtained for nearly all the assessed psychological determinants. The two exceptions were for outcome expectancies, which were not affected by either time or the intervention, and for coping planning, which was significantly affected by time alone. All groups demonstrated an increase in the planning of coping responses from baseline to four months, despite this increase only being significant in the NFH group (Mdiff 4month – baseline = 0.56, SE =0.24, p = .02). While no significant differences existed between the groups at baseline in relation to action self-efficacy, action planning, or action control, the levels for these determinants at the four-month follow-up were significantly higher in both the NFH and NFH+TM groups as compared to the FF group.
Despite the FF group demonstrating a slight, but significantly higher, level of intention at baseline, the level of intention among participants in this group was significantly lower than those in the other two groups at the four-month follow-up. Participants in the NFH+TM group demonstrated a significantly higher level of intention than the NFH group. At the four-month follow-up, participants in the NFH+TM group showed significantly higher levels of maintenance self-efficacy as compared to FF, as well as demonstrating significantly higher levels of recovery self-efficacy than both FF and NFH groups. In summary, for the psychological determinants, the NFH+TM and the NFH groups showed a positive and significant change in action self-efficacy, action planning, and action control as compared to the FF group. Intention and recovery self-efficacy increased in the NFH+TM as compared to the FF and NFH groups. Maintenance self-efficacy was higher in the NFH+TM group as compared to the FF group.
Item examples for behavioral, clinical, and psychological determinants (Cronbach's alpha, means* and standard deviations)
Discussion
This study was designed to evaluate the effects of using a NFH combined with TMs between appointments, with the goal of improving gingival health. Changes in adherence to interdental hygiene cleaning behaviors, clinical outcomes, and underlying psychological determinants among patients with gingivitis were assessed. Participants who received TMs in addition to the NFH demonstrated higher frequencies of flossing four months following their initial appointment. Participants in the NFH+TM group, on average, attained the recommended daily frequency of dental floss use and consequently had lower levels of gingival bleeding than participants who used FF or the NFH exclusively.
The average BOMP score in the NFH+TM group decreased significantly from a baseline of 60% to 30% at the four-month follow-up and approached less than 25% of bleeding on probing sites, which has been considered to correspond to gingival health established by Barendregt et al.21 However, it should also be acknowledged that the values for percentage of bleeding sites has been updated by Chapple et al, who definined periodontal stability as corresponding to fewer than 10% of bleeding on probing sites.23 The use of floss by way of a NFH was more frequent at four months than in the FF group, although this difference in behavior was not translated into a significant difference in BOMP scores.4 It was hypothesized that the NFH without TMs would also present a significantly lower BOMP scores than the FF group, however the results did not demonstrate any differences and supports findings from other studies where the efficacy of floss holders was no more effective than finger flossing.13,14
The use of TMs as reminders or “cues to action,” increasing proximity with the patient and frequency of flossing, was considered as a means of contributing toward effective use. In this regard, significant results were obtained for frequency of use. The combined use of TMs with the NFH contributed to a higher frequency of use in the NFH+TM group. These results were higher than those found previously in systematic reviews demonstrating that dental floss has a weaker effect on plaque or bleeding indices when used alone,3 due to patients' difficulty in accepting and using it correctly, as well as low levels of motivation and of dexterity.2,3,4 Reported levels of satisfaction with the use of floss holders found in earlier studies, were also lower than the level of satisfaction with the NFH identified in this study.13,14 This higher level of satisfaction could have contributed to the increased motivation at follow-up, inferred by increases in action self-efficacy and intention, thus supporting the hypothesis that the NFH would increase motivation to use dental floss, due to its novelty and ease of use.
Levels of recovery self-efficacy were higher in the NFH+TM group, but the other self-regulation variables were shown to be as high as in the NFH group. One explanation for this may be that, as the messages functioned as reminders for oral hygiene behaviors, they reinforced the subjects' beliefs that it is possible to return to and reach the objective, even following a lapse in the behavior (i.e., recovery self-efficacy). However, the NFH+TM group showed improved results at the behavioral level, without any significant differences in self-regulation variables (except in recovery self-efficacy), and may indicate that part of the TM effect on behavior operated via non-deliberated, automatic processes and was not mediated by deliberate self-regulatory cognitive processes.24
Results from this study showed an increase in motivation resulting from the use of a novel device to facilitate flossing, however only when accompanied by the use of TMs does the use of the NFH ultimately help reduce levels of gingival bleeding. Similarly to results previously described in the literature,25 findings from this study showed that the use of floss improved with increasing levels of intention. However, intention alone did not attain the desired outcome, and other self-regulatory processes or cues to action must also be deployed. The TMs seem to have worked as a cue to action in the NFH+TM group, contributing to an effect on flossing that could not be fully explained through an increase in self-regulation. It was not the changes in planning, but rather changes in self-efficacy that helped to explain the behavioral (flossing frequency) and clinical modifications (improved gingival health) obtained.
Study participants had positive reactions to the TMs. Considering the formality that traditionally characterizes the relationship between the oral health professional and the patient,20 the use of friendly and collaborative TMs may have contributed to forming closer relationships, facilitating patient-centered healthcare.16 The TMs may also have contributed to behavior changes as they consisted of persuasive messages from a credible source and were also a source of social support, fostering patients' self-efficacy and belief in being able to handle the challenge.16,20
Several limitations should be considered in the interpretation of the study findings. Although all participants used floss less often than the daily frequency recommended, participants were generally motivated towards oral hygiene behaviors, as inferred by high levels of intention at baseline. This is not surprising, considering that all participants had gingivitis and had been invited to have it treated at no cost. Therefore the results can only be generalized to similarly motivated individuals with low levels of floss usage. In order to better understand the motivational contribution of a NFH, a group combining the use of FF with TMs will be important to include in future studies. Future studies should also consider the comparison of floss holder devices vs another type of interdental cleaning aid such as interdental brushes, water flossers, and wood sticks. In spite of its limitations, this study had several strengths. The study included the objective BOMP clinical measures as well as self-reported measures. Second, the dental hygiene consultation appointment was designed to include important behavior change techniques for all groups, representing an important addition to the routine care included in these appointments. Third, was the inclusion of a follow-up at four months, a shorter interval than normally used.4,20 Future studies should look at the maintenance of these behaviors and gingival health status over longer periods of time.
Findings from this study have additional implications for practice, especially considering that TMs are inexpensive, easy to compose and apply. Text-messaging may be easily introduced into the routines of oral health professionals and integrated within a broader stepped, patient care approach.16 The option of articulating different interventions (NFH+TM) is also innovative, seeking to create a multiaction strategy to optimize the oral health behaviors addressed in the dental hygiene appointment. Simply telling patients to brush and floss as part of their dental hygiene care appointment is just not working for many people.26 However, flossing can be effective, if people become motivated to do it correctly and regularly.4,5 Moving beyond motivation, demonstrating positive results in the self-regulation processes underlying behavioral change, is a useful finding. Even when interventions are effective in fostering motivation for change, translating intention into self-regulation for behavior change, is more difficult to achieve.22, 27
Conclusion
The use of a novel floss holder, NFH, was shown to improve behavioral and psychological determinants of periodontal health four months after introduction of the device. However, clinical parameters measured by reduction in bleeding points on probing, only improved significantly when the NFH was used in conjunction with text messages delivered via a mobile device. Mobile text messages can support patients' motivation and serve as an alternative pathway to create cues to action, forming alternative routines and strategies. The use of a consciousness awareness technique, in combination with a novel device, such as a NFH, may help patients to reach therapeutic objectives and contribute to the management of periodontal pathologies such as gingivitis.
Footnotes
Mário-Rui Araújo, M. Psych, BSDH is a doctoral student at School of Psychology, University of Lisbon, CICPSI, Lisbon and an adjunct professor at Escola Superior de Saúde de Portalegre, Portalegre, Portugal.
Maria-João Alvarez, PhD is an associate professor at University of Lisbon, Department of Psychology, CICPSI, Lisbon, Portugal.
Cristina A Godinho, PhD is a researcher at Universidade Católica Portuguesa, Católica Research Centre for Psychological - Family and Social Wellbeing, Lisbon, Portugal.
This manuscript supports the NDHRA priority area, Client level: Oral health care (new therapies and prevention modalities).
Disclosure
The authors received material support from Oral Wise, Inc.; Calabasas, CA, USA, for the novel floss holder (GumChucks™) used in this study. This product is not marketed in Portugal. The authors did not receive any financial support for this study.
- Received June 10, 2019.
- Accepted March 17, 2020.
- Copyright © 2020 The American Dental Hygienists’ Association





{kind=link}
{kind=link}