



Abstract
Purpose: Numerous oral health promotion programs are directed at reducing the prevalence of early childhood caries. Smartphone applications (app) may be beneficial in oral health promotion. The purpose of this study was to evaluate the effect of a smartphone app, based on the Theory of Planned Behavior (TPB), on the oral health behaviors of the parents of preschoolers.
Methods: A two-phase, sequential, embedded mixed methods design explored how the app influenced the attitudes, beliefs, perceived behavioral control, and intentions of parents of preschoolers. Phase 1 was a quasi-experimental, one-group pretest-posttest design. Parents of preschool aged children (n=26) participated in the 4-week intervention. Phase 2 consisted of qualitative interviews with a purposive sample of parents from Phase 1 (n=11).
Results: Parents' behavioral intentions or oral health behaviors with their preschoolers did not significantly change from pre- to post-intervention (p>.05). Social norms (SN) and perceived behavioral control (PBC) predicted behavioral intentions pre-intervention and behavioral change post-intervention. Thematic analysis revealed that parents' belief in the importance of establishing oral health habits and brushing reminders and videos delivered via a mobile application supported efforts to form oral health habits.
Conclusion: The use of TPB constructs in the development of oral health promotions aimed at parents of preschoolers was partially supported. Intention and behavior were not affected post-intervention, but SN and PBC emerged as significant predictors of intentions and behavior. A dental smartphone app may aid parents to make good oral health habits part of their preschooler's daily routine.
Introduction
Dental caries is the most common chronic childhood disease in the United States (U.S.), with an estimated 14% of children suffering from untreated caries.1 Race, ethnicity, and socioeconomic status (SES) have been shown to play a significant role in the prevalence of dental caries in the U.S.1 The American Academy of Pediatric Dentistry also reports that the majority of children with early childhood caries (ECC), are low SES and qualify for financial assistance through Medicaid.2 Although oral health professionals have attempted to reduce ECC prevalence, treatment alone is not sufficient, and additional preventative action is needed.3 Health promotion aimed at increasing parents' or guardians' oral health knowledge is an integral component of oral health programs aimed at reducing caries including ECC,4-6 and has been shown to be successful when implemented through computer-based programs.5
An estimated 3.4 billion smartphone users worldwide, have downloaded mobile health applications in 2018.7 Interventions delivered through technology offer frequent, prolonged exposure which has been shown to be essential for an effective intervention.8,9 Current research suggests mobile technologies, such as smartphone applications (app), are a cost-effective approach to provide health information to large populations.10-13 Applications have the potential to improve the oral health behavior of parents and guardians of preschool-aged children. Interventions, based on the Theory of Planned Behavior (TPB), directed at mothers, have been shown to have a positive influence on children.14-16
The TPB was applied to a smartphone app, ToothSense,8 which was developed as a means to educate parents and guardians on the importance of good oral health behaviors for children.8 The app was designed using the Behavior Intervention Technology (BIT) model which accounted for the clinical aims and intervention strategies and their incorporation into the overall features of the app.17 The BIT model accounts for the “why, how, what and when” type questions that are documented in the design features integrated into the intervention strategies.18 The smartphone app included parental or guardian support in the form of documents and videos on oral hygiene instructions, timer videos, a journal to track tooth brushing times, tooth brushing reminders, and a social feed to share tooth brushing and flossing experiences with family and friends.8
There is a lack of research demonstrating how a smartphone app incorporating the TPB designed to influence parents and guardians, can impact children's oral health. The goal of this pilot study was to explore the influence of a smartphone app on parents' attitudes, subjective norms (SN), intentions, and perceived behavior control (PBC) of the oral health behaviors of their preschool-aged children.
Methods
This study was approved by the MCPHS University Institutional Review Board with the assigned protocol ID IRB082017L. Informed consent was received from the participants prior to beginning each study phase. A two-phase, sequential embedded mixed methods research design was used to test a smartphone app prototype (ToothSense) in an applied setting. The first phase of the research used quasi-experimental, one-group pretest-posttest design.18 In the second phase, qualitative data was collected via interviews to support and build on quantitative results.19 Phase one participants were recruited at two Head Start programs, two public preschools and local medical and dental offices throughout Rio Grande County, located in rural southwestern Colorado. Nearly 18% of the population in Rio Grande County lives in poverty20 and the dental safety-net is at capacity due to a large number of Medicaid-eligible individuals and a lack of dentists accepting it.21,22 In addition, Rio Grande County's municipal water supplies are not fluoridated.23 Inclusion criteria for phase 1 were parents of at least one preschooler who used an iPhone. The minimum number of phase 1 participants was determined by the medium effect power of 80% and calculated to be 26 participants.
Once participants provided consent (n=33), they received an email with instructions to download the smartphone app and create push notifications for brushing reminders, which also served as a reminder to use the app daily. After confirming the app was installed and working correctly, participants received an email to take the pre-intervention questionnaire using a web-based survey tool.
A 124-item validated questionnaire designed by Van den Branden et al.24 to measure oral health behaviors in children and TPB determinants was used, with permission, prior to and following use of the app. Four TPB-components identified and explained 44% of the total variance of dietary habits.24
The questionnaire consisted of 71 belief-based items related to three primary scales: dietary habits (24 items), oral hygiene (22 items), and dental attendance (25 items). The belief-based items included questions regarding attitude, intention, SN, self-reported behavior and PBC. There were additional questions to gather background information on dental care (14 items), children's oral hygiene habits (7 items), nutrition (17 items), parents' oral health (8 items), and demographics (4 items).
Upon completion of the pre-intervention questionnaire, participants were instructed to use the app twice a day for four consecutive weeks. The app was designed with push notifications to support usage.17,18 After four weeks, participants received instructions on completing the post-intervention questionnaire. Participants who completed the post-intervention questionnaire were sent an incentive and information about phase two.
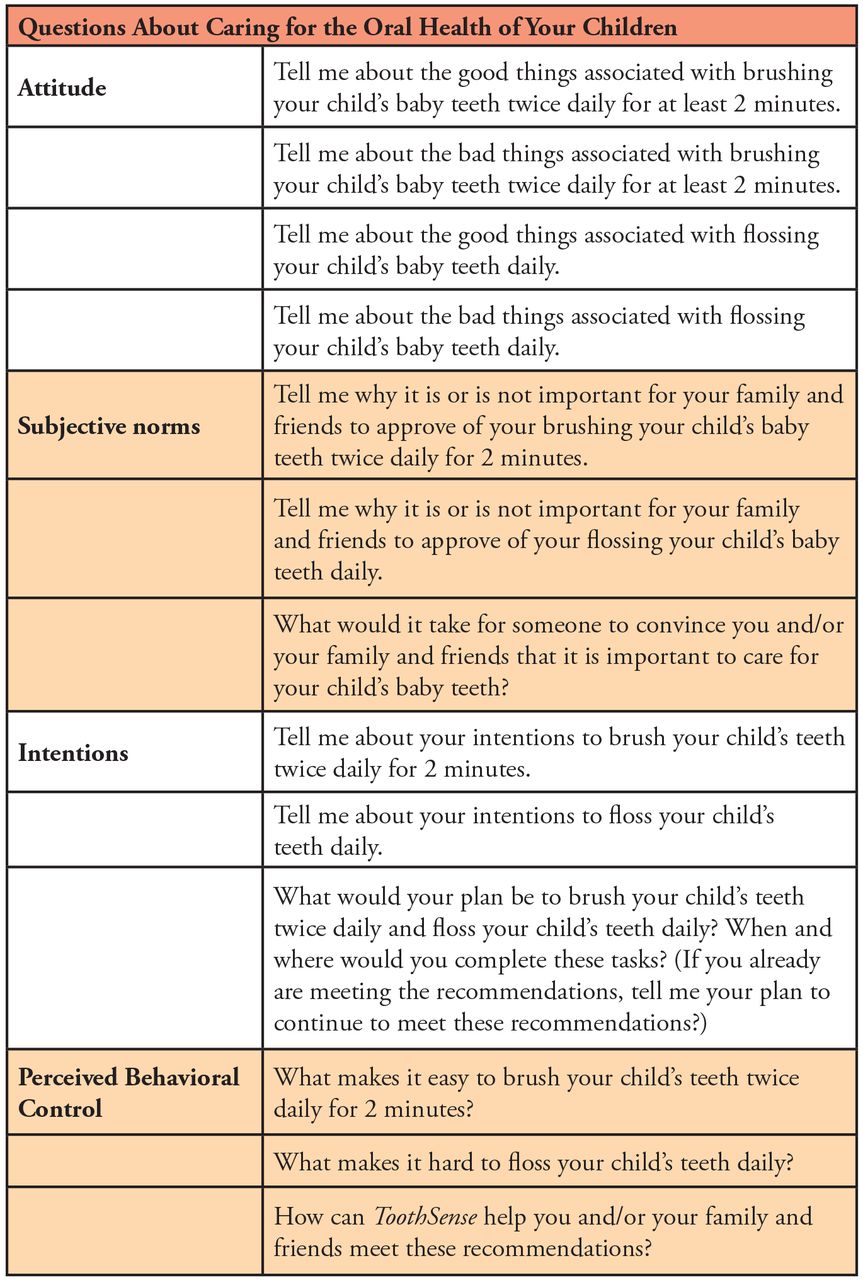
Phase 2 consisted of semi-structured interviews using 13 open-ended questions based on previous research by Zoellner et al.25 The questions asked how parents cared for their children's oral health based on the TPB determinants including attitude, SN, intentions, and PBC following the use of the smartphone app (Figure 1). Responses were gathered using virtual interviews recorded and conducted using a video conferencing platform (Zoom Video Communications, San Jose, CA). Interviews were transcribed and coded to identify themes. Once no new themes emerged, it was determined saturation was reached.26 Participants who completed the interview received an additional incentive.
Demographic information and variables of interest were reported using summary statistics. The independent variable time had two levels, pre- and post-use of the smartphone app. Differences in behavioral intention and reported behavior between the pre- and post-intervention were examined using repeated measures within a group t-test. Regression analysis was also used to explore whether any variables of interest predicted behavioral intention or reported behavior.
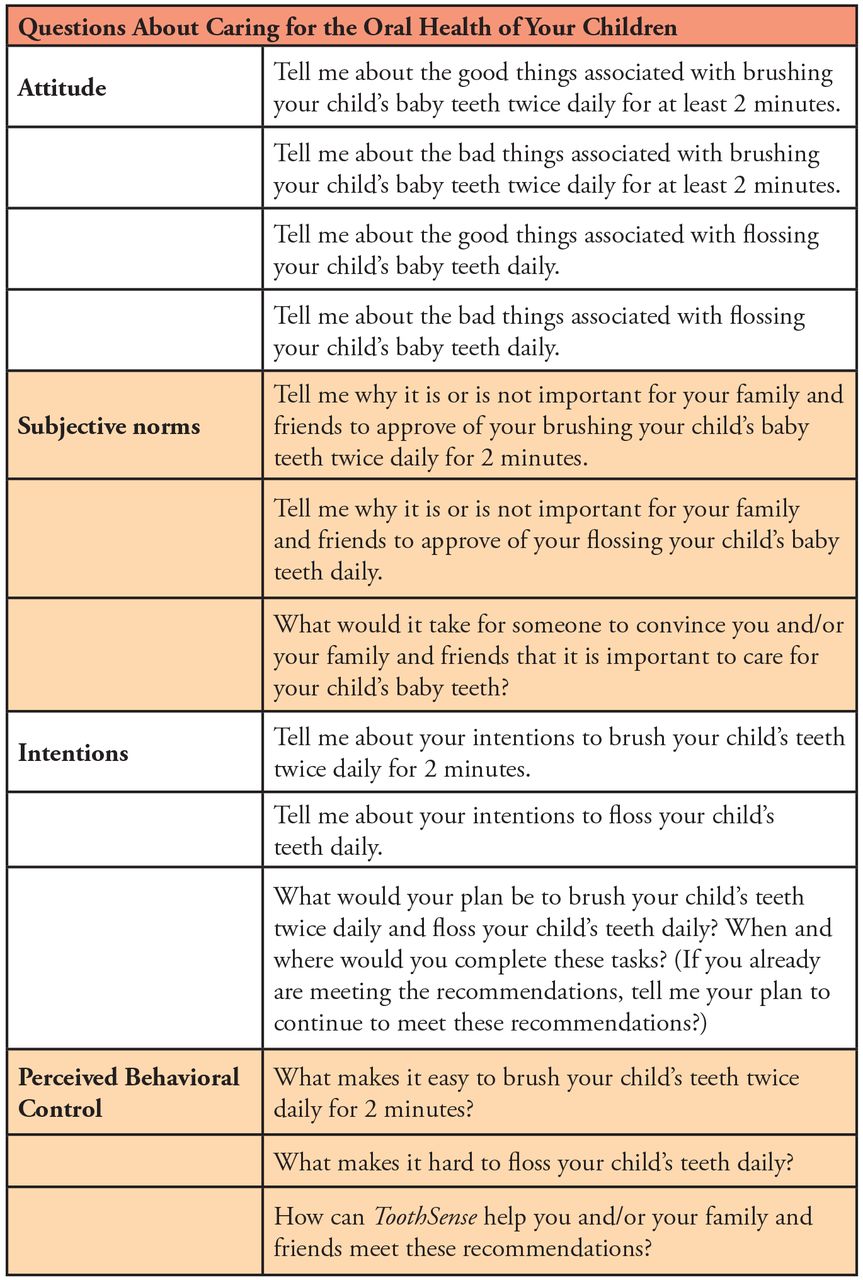
Qualitative interview questions
The recorded interviews were transcribed verbatim by the investigator. Participants were sent a copy of their transcribed interview to verify accuracy. Using an inductive process, the principal investigator and the creator of the app independently reviewed the transcripts for common words and phrases to identify initial key themes. Notes were compared to resolve any inconsistences. The themes were organized into lists according to the TPB constructs used to create the app to answer the research question.27
Results
Invitations to complete the pre-intervention questionnaire were emailed to 41 parents of preschool children (n=41). Of those, 33 participants completed the pre-intervention questionnaire (n=33). The mean age of the children was 3.48 years (SD 0.93). At the end of four weeks, 26 participants completed the post-intervention questionnaire (n=26). For the majority of the participants, this was their first child, and the child resided with both parents (Table I). Of the parents who completed both the pre- and post-intervention questionnaires (n=26), 54% reported that their child had been to the dentist within the past six months, and 42.4% reported their children had their teeth brushed at least once a day (Table II). Over half of the parents reported that their child eats sugary snacks between meals more than once a week but not every day; 39.4% reported that their child consumed sugary drinks between meals more than once a week but not every day (Table II).
The TPB survey was assessed and each of the scales (attitude, SN, PBC, short- and long-term consequences) showed acceptable reliability levels across the three domains of dietary habits, oral health behaviors, and dental attendance (α=.71-.83) with belief in short term consequences for the dental attendance domain being the lowest (.71). To test the hypothesis that participant attitudes, SN, PBC, intentions or behaviors would change after using the smartphone app, paired-sample t-tests were conducted for each of the variables across dietary habits, oral health, and dental attendance. To compare the scores for the TPB, each subscale was computed by summing the items for each subscale based on the Van den Branden et al. findings.24 Single items were entered for pre- and post-intervention (e.g., intention to limit sugary snacks) for all behavior and intentions outcomes. No changes were found in dietary habits, oral health practices, and dental attendance when tested across the TPB constructs of attitude, PBC, and SN. Parents' behavioral intentions or reported oral health behaviors used with their preschoolers did not change with the use of the app. Table III shows the mean of each subscale score for pre and post intervention measurements.
Participant demographics (pre-intervention n=33, post-intervention n=26)
Linear regression was used to determine the predictive relationship of each TPB subscale on the domain matching intention and behavior (e.g., parent intention to limit sugar snacks for their children regressed onto dietary attitudes, SN, and PBC). Characteristics measured by the TPB survey predicting intention or behavior were examined. Three separate models were performed using dietary attitudes, SN, and PCB to predict the intention to limit sugary snack frequency for children (pre-intervention), the number of sugary drinks the child consumes between meals (post-intervention), and the number of sugary snacks the child consumes between meals (post-intervention). The dietary attitude model was a significant predictor of dietary intention (R2=.38, p=.004) with dietary PBC emerging as the only significant predictor in the model (β=.57, p=.002). The model was also a significant predictor of sugary snack frequency (R2=.41; p=.007) with dietary SN predicting behavior (β=-.64, p=.006) but not attitude or PBC (p>.05). Lastly, the model was not shown to be a significant predictor of the frequency of sugary drink consumption (p=.22).
Two separate models were performed with oral attitudes, SN, and PBC predicting intention to ensure the child brushes their teeth daily (pre-intervention) and the frequency that the child brushes their teeth (post-intervention). This model was shown to be a significant predictor of intention (R2=.40; p=.002) with SN (β=.46, p=.009) and PBC (β=.50, p=.02) however, not attitudes (p=.22). The model was not a significant predictor of behavior post-intervention (p=.90).
Lastly, two separate models were conducted with dental attendance SN, PBC, short-term consequence beliefs, and long-term consequence beliefs predicting intention to take the child twice a year for a check-up (pre-intervention) and the last time the child had been to the dentist (post-intervention). Neither model was shown to be significant (p>.05). However, PBC was a significant predictor of intention (β=.46; p=.02).
Oral health behaviors of parents and children (n=26*)
Pre- and post-intervention mean scale score (n=26)
A new change variable was created to investigate which subscale sets predicted change in intention or behavior from pre- to post-intervention. Change was calculated by dichotomizing whether a participant changed a response from pre- to post-intervention (1) or not (0). Table IV shows the frequency of parents who either changed or did not change from pre to post intervention. The new variable (their response) was used in a logistic regression model to determine the predictive relationship of each subscale set (dietary, oral, and dental attendance) on the odds someone would change self-reported behavior or intention between pre- and post-intervention. Each model had subscales for the set predicting intention and behavior change for the matching items (e.g., dietary subscales to dietary behavior and intention). The oral subscales were significant predictors of the likelihood of changing intention to have the child brush daily (either direction) between pre- and post-intervention (χ2(3, 26)=10.34, p=.02, R2=.50) with a one unit increase in the SN scale predicting 1.2 times higher odds of changing (p=.04). Dental attendance subscales predicting change from pre- to post-intervention in intention to take the child for a check-up twice a year was not a significant model (p>.05) however a one unit increase in the PBC scale predicted 2.43 times increase in the likelihood of changing between pre- and post-intervention (p=.02). All other models were not significant (p>.05). All models regressing outcome variables on demographic variables were not found to be significant (p>.05).
Qualitative data from the second phase of the study resulted in five emergent themes organized across the TPB constructs for attitude, SN, intentions, and PBC.
Attitude
When asked about the good or bad aspects associated with caring for their children's teeth, the majority reported positive associations corresponding to having strong teeth and developing good habits in addition to the prevention of caries and gingivitis.
“It'll help with cavities and bad breath; and teach them to brush their teeth when they're older.”
The child's cooperation and fear of improper technique were the most mentioned negative attitudes.
“They're not interested in doing it. It just is it takes a lot of work to make them do it, and sometimes maybe I'm worried that they are not doing it correctly or long enough.”
Frequency of parents whose scores changed from pre- to post-intervention (n=26)
Several parents reported an improvement in attitude with the assistance of the “goal setting” to set their own personalized brushing reminders and the “brush along” and educational videos.
“The app made us start brushing his teeth twice a day because normally we just did it at night. I would say he did better with it. It was more like three to four days a week instead of none. He liked watching some of the videos, and that kept him brushing longer.”
Subjective Norms
When asked if it was important for family and friends to approve of caring for baby teeth, a majority felt family and peer approval was important, especially from other parents and caregivers such as grandparents. Family and friend influences were also important in promoting oral health among their children.
“So, when they're spending the night with grandma or granddad then they are following through and brushing teeth while we're away and that's comforting.”
The participants motivation to comply with professional oral health recommendations stemmed from the prevention of caries and gingivitis.
“I think my wife and I both had issues in our late teens with cavities and root canals and our parents were not adamant about brushing.”
Several participants felt restorative dental care cost was a motivation to comply with oral health recommendations.
“I put so much money into my own mouth that I think it's very important. I don't want to spend lots of money because they won't brush their teeth.”
Intentions
When asked about intentions to meet oral health recommendations, a majority of participants had positive intentions to meet the recommendations for their child. Oral health promotion measures, such as keeping oral health practices part of a daily routine, helping their children maintain healthy teeth and good oral habits, and finding motivators for the child, such as a new toothbrush, were identified as the most common plans for parents to continue to meet oral health recommendations.
“I'd like to be more like intentional for the morning one [brushing].”
Some parents felt the “brush along” videos improved their intentions to brush their child's teeth for two minutes and one parent felt that the brushing reminder would aid in their intention to brush their child's teeth in the morning.
“I think about the app, you know in the back of my mind I'm like oh I want to put that on. I feel like the reminders in the morning, and at night, seemed like they helped keep us on track. You should be brushing his teeth at this time, and we can get him in bed by this time. It helped to keep the routine…”
Perceived Behavioral Control
In response to what made it easy to brush twice per day for 2 minutes and floss once per day, most felt promoting oral health through a daily routine made meeting the recommendations easier. Some parents felt using motivators for their child made it easier.
“You know once it's a habit, it's not an issue. If we start to forget the kids remind us.”
A vast majority revealed a lack of cooperation from the child was a hindrance when attempting to meet these recommendations.
“Yeah just if she's battling me. Toddlers are just on the go all the time. Sometimes she just refuses to sit still.”
Some parents felt the “brush along,” and the “educational” videos improved their PBC in brushing their child's teeth for two minutes two times a day.
“I think having that video reinforcing you know we need to brush the same time that the video's going has helped make sure that we're brushing for an adequate amount of time every day.”
Smartphone oral hygiene applications
In response to how the smartphone app could help with oral health recommendations, 90% of parents interviewed for phase 2 reported that the app aided in supporting oral health recommendations for their child. Most parents reported the “goal setting” (45%) and the “brush along” videos (72%) were beneficial. Twenty-seven percent reported the “educational” videos and 18% reported the “tracking the happy teeth” in the “mouth journal” helped support their care for their children's oral health. Two parents mentioned the kid-orientated design of the app was another helpful feature.
“The reminders and timer are helpful; the app and little videos are fun. I'm not sure what else it would need. I think it meets all the things needed and it reminds you to do it and helps you make it fun.”
Discussion
The low mean change score in this study suggests the changes in behavioral intention and reported behavior were random and not associated with this particular smartphone app. However, previous research has demonstrated the efficacy of health information technology in delivering health interventions and health promotion to a large population through the use of apps.10,13 Findings from this study are similar to those of Bueller et al., whose research did not show significant changes in behavior intentions when utilizing a smartphone health app.12 The smartphone app, Toothsense, piloted in this study has the potential to be used as a tool to aid parents in meeting the oral health needs of their preschool-aged children. The data from this study demonstrated the TPB constructs significantly predicted the oral health behaviors and intentions of oral hygiene, dietary habits, and dental attendance. Social norms, including approval from the child's pediatrician and the family dentist, were shown to be a significant predictor of oral hygiene intentions and dietary behaviors. Although PBC and SN demonstrated the strongest correlations in this study, attitude and intentions have been demonstrated to have the strongest associations in other studies.15,16 This difference could be attributed to the high attitude scores of this study population as shown in the pre-intervention questionnaire.
A portion of the study population was recruited from Head Start programs which offer oral health support to parents.28 In addition, a majority of the parent participants had education past the high school level. Both factors may have influenced the high attitude scores on the pre-intervention questionnaire. Castilho et al. identified a link between childrens' oral health and parents' knowledge, attitude, SES, level of education and maternal age.4 While studying a population already educated on the importance of oral health did not demonstrate improvement in attitude and intention, increasing parental knowledge has been shown to be an important component in changing behaviors and attitudes.4,6,29
Although Phase 1 data did not demonstrate that use of the smartphone app changed behavioral intentions and behaviors in the study population, qualitative data gathered from Phase 2 suggested a perceived value for the use of the app. A majority of participants from Phase 2 felt that the app aided them in meeting the oral health recommendations for their children and supports an association between PBC and behavior as described by McDermott et al.15
There were limitations to this study. The sample population was not representative of the general population of Rio Grande County, Colorado.20 The smartphone app was only available in English and on an iPhone platform. This may have limited potential participants who were more representative of the general population. A larger sample size for phase 1 would have been beneficial to increase the study's statistical power. Also, parents may have given socially acceptable responses, creating bias. Future studies would require the smartphone app to be available on an android platform, in multiple languages, and utilize a larger sample population.
Conclusion
Although the results from this study did not support the use of a smartphone app to improve attitudes, SN, intentions, and PBC of the parents of preschoolers, it can be concluded that PBC is a significant predictor of dietary, oral hygiene, and dental attendance intentions and should be considered when developing oral health promotion. Social norms were shown to be significant predictors of dietary behaviors and oral hygiene intentions and the use of TPB can support oral health goals in developing oral health promotions aimed at parents of preschoolers. Although the qualitative data suggest that a smartphone app supports parents' efforts to make oral health recommendations part of their preschooler's daily routine, more quantitative data needs to be collected to establish the use of TPB in developing oral health interventions.
Acknowledgements
The authors would like to acknowledge S. Van den Branden, S. Van den Broucke, R. Leroy, D. Declerck, and K. Hoppenbrouwers for granting permission to use their survey. Sara Nolen is the creator and owner of the free smartphone application “Toothsense” available from the App Store (iOS).
Footnotes
Carly J. Santi Lozoya, RDH, MS is a graduate of the Forsyth School of Dental Hygiene; Lori Giblin-Scanlon, RDH, DHSc is an associate professor and the Associate Dean for Clinical Programs at the Forsyth School of Dental Hygiene; Linda D. Boyd, RDH, RD, EdD is a professor and the Associate Dean of Graduate Studies at the Forsyth School of Dental Hygiene; Sara Nolen, RDH, MS is a graduate of the Forsyth School of Dental Hygiene; all at MCPHS University, Boston, MA.; Jared Vineyard, PhD is a postdoctoral fellow in applied research, St. Luke's Health, Boise, ID.
This manuscript supports the NDHRA priority area Client level: Oral health care (health promotion: treatments, behaviors, products).
- Received October 8, 2018.
- Accepted March 29, 2019.
- Copyright © 2019 The American Dental Hygienists’ Association





{kind=link}