



Abstract
Purpose: The purpose of this study was to assess the oral health needs of community-dwelling older adults participating in congregate meal centers and to determine whether differences exist in the oral health needs of older adult populations residing in urban versus rural communities in the state of Texas.
Methods: Study participants were recruited at 6 congregate meal centers located in identified rural and urban communities in the greater metropolitan area of Austin, Texas. (N=78) Participants completed a validated, modified questionnaire containing 20 items on the following topics: self-reported oral health, tooth loss, dental insurance, frequency of dental visits, time since last dental visit, access to dental care, dry mouth, and oral cancer screening. Each participant received an oral health screening based on the Association of State and Territorial Dental Directors Basic Screening Survey for Older Adults. The examiners received hands-on training prior to the study to ensure the validity of their findings and to test for inter-examiner reliability.
The chi-square test of independence was performed to analyze the participants' responses on the Basic Screening Survey to identify any relationships between the variables.
Results: There were no significant differences in oral health conditions of older adults residing in urban versus rural communities. Over 50% of the participants (64.9% urban; 56.1% rural) reported incomes below $15,000 and lacked dental insurance to cover all or a portion of their oral health care needs. Eighty-seven percent of the participants reported tooth loss due to dental caries, 35% required periodontal care, and 37% reported occasional and 43% reported frequent oral pain over the last 12 months.
Conclusions: Oral health promotion and disease prevention is an emergent need for older adult populations residing in urban and rural communities of the state of Texas. Analysis revealed that the majority of the older adult populations in both settings to have financial and socioeconomic barriers to access preventative and restorative dental care services.
Introduction:
The older adult population in Texas is projected to triple by the year 2050, making 65 years and older, the state's population average.1,2 This rise in the aging population will also include an increased demand for medical and dental care.3,4 Although Medicaid, Medicare, and the Affordable Care Act have been established to cover the costs of medical care, there is limited insurance coverage for older adults requiring dental care.5-7 This lack of coverage requires community-dwelling older adults to find their own dental insurance for dental expenses or to pay out-of-pocket.5,6 Most community-dwelling older adults are retired and live on fixed incomes that do not accommodate for the rising costs of oral health care in the United States (US).8,9 Currently, the oral health needs of this population along with the appropriate strategic plan for meeting these needs has not been determined in the state of Texas. While the Texas Department of Health and Human Services has a program in place ensuring that all children and adolescents receive oral health services, similar oral health care programs for older adults do not exist.10,11 The lack of an oral health care program for older adults may be impacting the management of systemic conditions in this population.12 Home health and respite services typically do not include oral health services even though research has determined an association between oral health and the aging process.13
The Surgeon General's National Call to Action states that “…no rural inhabitant, no homebound adult, no inner city dweller should experience poor oral health because of barriers to care…14 The Administration on Aging released a report revealing the population over the age of 60 years increased by 34% from 2005-2015, and estimated approximately 1 in 7 residents will be considered older adults.8 At the same time, the US Census Bureau projects that the average age of the adult population is now 60 years and over and will continue to increase.15 In Texas, this population is projected to increase to 12 million older adults, tripling the population of older adults by the year 2050.16 The anticipated growth of the aging population will also increase the demand for medical and dental care services.8
Oral health promotion and disease prevention has been shown to have a positive impact on the aging process in older adults.13 Preventive oral health services in the older adult population can slow the aging process and inhibit systemic inflammation by reducing inflammatory cell markers.17 Oral health promotion also plays a key role in the quality of life for older adults.18 Individuals with good oral health lead a more active lifestyle and have a more positive outlook regarding the aging process.13,18 When dental coverage is limited, individuals are less likely to receive preventive care and must seek out emergency room care when dental problems become acute and start to affect other body systems.19,20
Geographic and socioeconomic challenges have been identified as two of the main barriers to access to oral health care in older adult populations. Federally qualified community health centers (FQHC) are more likely to be available and utilized in urban areas as compared to rural areas often because of differences in driving distances.13,21 Despite the availability of community health centers, socioeconomic disparities can also hinder the ability to obtain services for this population.21 Dental services for older adults dependent on home health care are limited because they are not included as part of the home health and respite care services in the state of Texas.22
The purpose of this study was to assess the oral health needs of community-dwelling older adults participating in congregate meal centers and to determine whether differences exist in the oral health needs of older adult populations residing in urban versus rural communities in the greater metropolitan area of Austin, Texas.
Methods:
This cross-sectional observational study was part of a statewide study conducted in Texas to determine the oral health needs of community-dwelling older adults attending congregate meal centers while also participating in Medicaid, Medicare, and other state assisted programs for low income adults.
Setting and Sample
This study was administered in six congregate meal centers in the Austin-metropolitan areas and received the approval of the Meals on Wheels and More organization director and the center events coordinator. Congregate meal centers provide nutritious meals on a daily basis in a variety of group settings such as senior centers and are supported through the Title III Congregate Nutrition Program.23 Three of the metropolitan Austin congregate meal centers were designated as rural locations, serving populations less than 10,000, while the remaining centers were considered urban with populations exceeding 10,000 as determined by the 2010 US census.24
Inclusion criteria were adults aged 65 years and older who participated in the congregate meal center activities. Participants were recruited during an oral health education presentation and were provided with a recruitment letter in English and Spanish. Study participants reviewed and signed informed consent forms prior to receiving the questionnaire and oral screening.
Survey and Screening Process
The Association of State and Territorial Dental Directors (ASTDD) Basic Screening Survey (BSS) for Older Adults Toolkit was used for the study.25 The toolkit included examiner training materials (PowerPoint presentation and video), screening form, and participant questionnaire.
The training video and manual was used for hands-on examiner training to ensure the findings were valid and could be replicated between the examiners. Two examiners, a dentist and a dental hygienist, acted as examiners for the study. To maintain ongoing calibration, every tenth participant was screened by the two examiners independently to maintain calibration and validate the findings.
The BSS questionnaire utilized questions from the NHANES (National Health and Nutrition Examination Survey), BRFSS (Behavioral Risk Factor Surveillance System), and NHIS (National Health Interview Survey) surveys. The topics in the BSS questionnaire included: self-reported oral health, tooth loss, dental insurance, frequency of dental visits, time since last dental visit, access to dental care, dry mouth, and oral cancer screening (20 items).25 The ASTDD recommended addition of demographic questions (5 items).25 Validation information was not provided in the ASTDD BSS for Older Adults Manual. The participant questionnaire was made available in English and Spanish.
After completing the questionnaire, each participant had an oral health screening performed by calibrated examiners utilizing the ASTDD Basic Screening Survey for Older Adults form. The examiners performed the following assessments: functional posterior occlusal contacts, substantial oral debris, number of upper and lower teeth, untreated decay, root decay, number of teeth with root decay, root fragments, tooth mobility, need for periodontal care, severe dry mouth, suspicious soft tissue lesions, and treatment urgency.25
Statistical Analysis
Descriptive statistics were used to describe the differences between the demographic characteristics and the oral health conditions of the participants in the study. All statistical analyses were performed in STATA® statistics/data analysis software version 14.0. A chi-squared test of independence was utilized to analyze the questionnaire data and the oral health assessment data for relationships between the following variables; including: oral health conditions, economic, and demographic conditions of the participants.
Results:
Population Demographics
A total of 78 volunteers (n=37 urban, n=41 rural) participated in the study. No significant differences were found in demographic characteristics between the urban and rural populations. (Table I) The majority of the survey participants were women and reported family incomes of $10,000 - $14,999, making them ineligible for Medicaid.25 However it is worth noting that these individuals were also unable to afford the out-of-pocket costs of dental services through the Medicare Advantage program.8 The majority of participants in both the urban and rural communities reported a lack of dental insurance coverage to pay for either all or a portion of their dental care costs (64.9% urban, 56.1% rural).
General and Oral Health Conditions
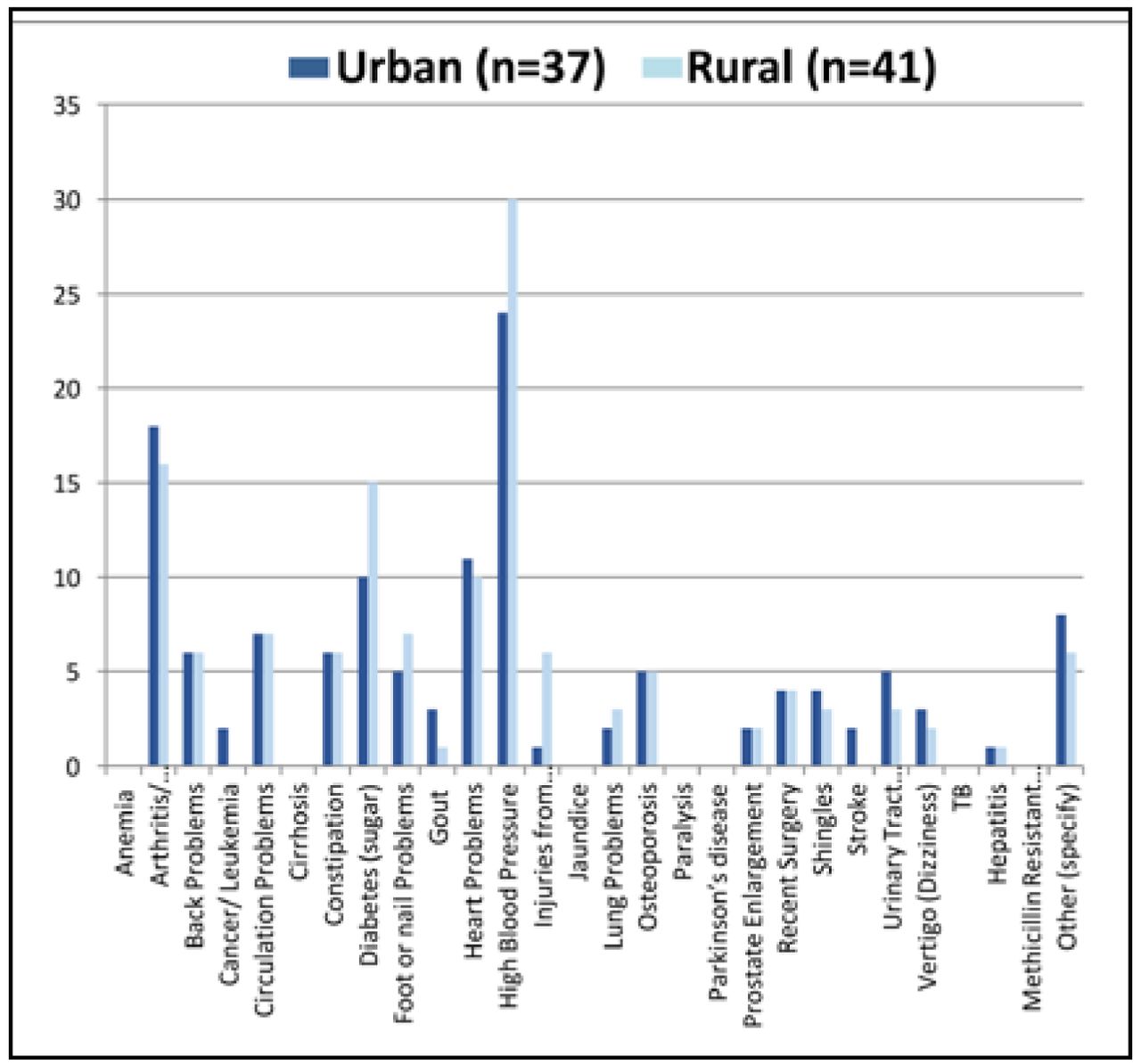
Common general health conditions reported by the participants from both rural and urban communities were hypertension, arthritis, and type 2 diabetes.(Figure 1) Respondents reporting common chronic health conditions, also reported having ongoing oral disease such as untreated dental caries, periodontal disease and lacked dental insurance to assist in the payment of routine dental care. (Table II)
Demographics of Urban and Rural Communities in Austin, TX.

Medical Conditions Self-reported by Older Adults Residing in Urban vs. Rural Communities
No significance differences were revealed between the oral health conditions reported in the urban versus the rural communities. (Table II) The majority of the participants (86.6%), regardless of the community setting, reported tooth loss due to dental caries and/or periodontal disease. (Table II) Over one third of the participants reported having painful aching in the mouth over the past year, either occasionally (37%) or very often (43%). A total of 53.3% of the urban and rural participants reported frequently avoiding certain foods because of tooth, mouth and denture pain. (Table II)
The oral screening revealed that 48.6% of the urban and 56.1% of the rural communities had untreated dental caries present at the time of the study. Seventy-nine percent of participants had missing teeth and 11-24% of the remaining teeth demonstrated chronic oral infection requiring periodontal therapy. Less than one-third of the participants reported having dental insurance, 28% urban and 32% rural. (Table II) Forty-nine percent urban and 56% rural participants reported over that it had been more than 2 years since their last dental visit. The primary reason reported for a dental visit was oral pain by 34% of the urban and 38% of the rural participants. (Table III) Over 50% of both the urban and rural communities reported having had oral pain during the past 12 months but were unable to seek dental care due to cost of treatment.(Table III)
Discussion:
Systemic conditions such as hypertension, rheumatoid arthritis and diabetes have been associated with chronic conditions related to poor oral health.27 In the present study, the majority of respondents reported being diagnosed with chronic systemic diseases that included hypertension, arthritis, and diabetes. These findings indicate that both rural and urban participants have chronic systemic conditions; research also suggests an association these conditions and oral disease, putting this population at even greater risk.27 Taking these findings one step further, oral health is also related to healthy aging so it is critical to educate this population on the importance of maintaining good oral health.13
The finding that over half (53%) of participants reported often avoiding certain foods because of tooth, mouth and denture pain may lead to compromises in nutrition status. Research has shown that tooth loss and the ability to chew food may lead to decreased consumption of nutrient-rich fruits and vegetables which may further result in malnutrition for sustaining energy and immunity to systemic infections.28,29
Although there were no significant differences in the oral health needs between the urban and rural communities, there were similarities based upon the need for improvements of access to oral health care and education for this specific population. Over half of the participants in both types of communities revealed an urgency for immediate oral health care but also lacked access to oral health care services due to the rising costs of dental care and a limited understanding of the important relationship between oral and systemic health.5,6,13 Texas Medicaid coverage limits dental services to dental extractions and emergency care.12 Eligible Medicare Advantage members were unable to pay the co-payments of the rising costs of dental services due to their fixed incomes.58 As the older adult population increases, the demand for oral health services will also increase the need for medical care.1,9 With the older adult population's limited access to oral health services in Texas, an increased number of exacerbated systemic illnesses and emergency room visits may result, leading to higher demands for emergency room and other hospital services as well as workforce expansions of oral health professionals.19,30,31 A plausible solution to these increased demands on the health care system could include the implementation of a mid-level oral health provider, capable of assisting in the triage and care in medical centers and other community settings.30
Oral Health Conditions of Urban and Rural Communities in Austin, TX.
Oral Health Services in Urban and Rural Communities in Austin, TX
Limitations of this study include the potential for the inaccurate recall of the study participants influencing the responses to the self-reported survey questions related to demographics, oral health history, and general health. Future studies should focus on examining the multiple issues related to access to oral health care for community-dwelling older adults throughout the state of Texas as well as other states.
Conclusions:
Oral health promotion and disease prevention is an emergent need for older adult populations residing both urban and rural communities in the state of Texas. More research is needed in these populations to assess the impact of the lack of access to routine dental services on oral as well as systemic health. As the older adult population continues to increase, oral health care will play a crucial role in the overall management of systemic diseases accompanying this age demographic. Demand for oral health care services will increase as more older adults choose to live independently within their communities. With limited coverage of Medicaid and Medicare for preventive and restorative dental services, the expansion of services provided by oral health care professionals may assist in supporting overall health and wellness.
Footnotes
Julie L. Martin, RDH, MS, MPH is a graduate of Forsyth School of Dental Hygiene, MCPHS University; Boston, MA; Linda D. Boyd, RDH, RD, EdD, is the dean, Forsyth School of Dental Hygiene, MCPHS University; Boston, MA; Helena Tapias-Perdigón, DDS, MS; a Clinical Assistant Professor at Texas A&M University College of Dentistry, Dallas, TX; Lisa LaSpina, RDH, MS, is an assistant professor, Forsyth School of Dental Hygiene, MCPHS University; Boston, MA.
This manuscript supports the NDHRA priority area Population level: Health services (epidemiology).
- Received June 22, 2016.
- Accepted April 5, 2017.
- Copyright © 2017 The American Dental Hygienists’ Association





{kind=link}