



Introduction
According to the CDC, between 12.1% and 41.9% of the American population ages 5 years and older (depending on age and income level) has untreated dental caries. In addition, the percentages of those who have restorations vary from 44.5% to 92.6%. Children at or below the federal poverty level (and most likely Medicaid eligible) have the highest untreated dental caries rates for children, at 25.4%. Yet nationally, only 46.9% of children receiving Medicaid, on average, were able to access any dental care in 2013. Limited Medicaid budgets often lead to Medicaid fees that are below the cost of providing surgical treatment to repair the damage caused by caries. However, it is possible to provide effective preventive treatment by dental hygienists or other health professionals at lower costs before the disease progresses to an irreversible state which necessitates surgical repair.
The construct of classifying health services into three levels of prevention to differentiate them from curative treatment was developed by Leavell and Clark in 1965.3 More recently, Jekel defined the levels of prevention as listed in Table 1.4
Our knowledge about dental disease and how to prevent it has increased significantly, which opens opportunities to provide beneficial care to many people who otherwise would not receive it and who would ultimately suffer the consequences of untreated disease. The DentaQuest Institute has been partnering with Boston Children's Hospital (BCH) since 2008 on an Early Childhood Caries Collaborative that makes extensive use of primary, secondary and tertiary prevention. The ECC Collaborative's protocol includes performing a risk and behavior assessment to determine which risky behaviors parents are doing and whether they are using protective factors.5 When it comes to the determinants of health, we know that behavior may contribute 40%, while health care services may only contribute 10%.6 Changing behavior can have a profound affect, and the clinical staff in the collaborative was trained in motivational interviewing, behavior modification and simple goal setting. Parents are taught the causes of tooth decay. Most are not aware that the apple juice they put in a Sippy Cup has a pH of 3.5% or that milk in a bottle at bedtime damages their child's teeth. Goal setting asks parents to pick just one risky behavior they can work on during the next month, such as putting water in the Sippy Cup or the bedtime bottle. Or they may choose to add a protective factor, like brushing the child's teeth with a smear of fluoridated toothpaste. BCH found that it was able to reduce the risk status of children from high risk to moderate risk after three of these visits.
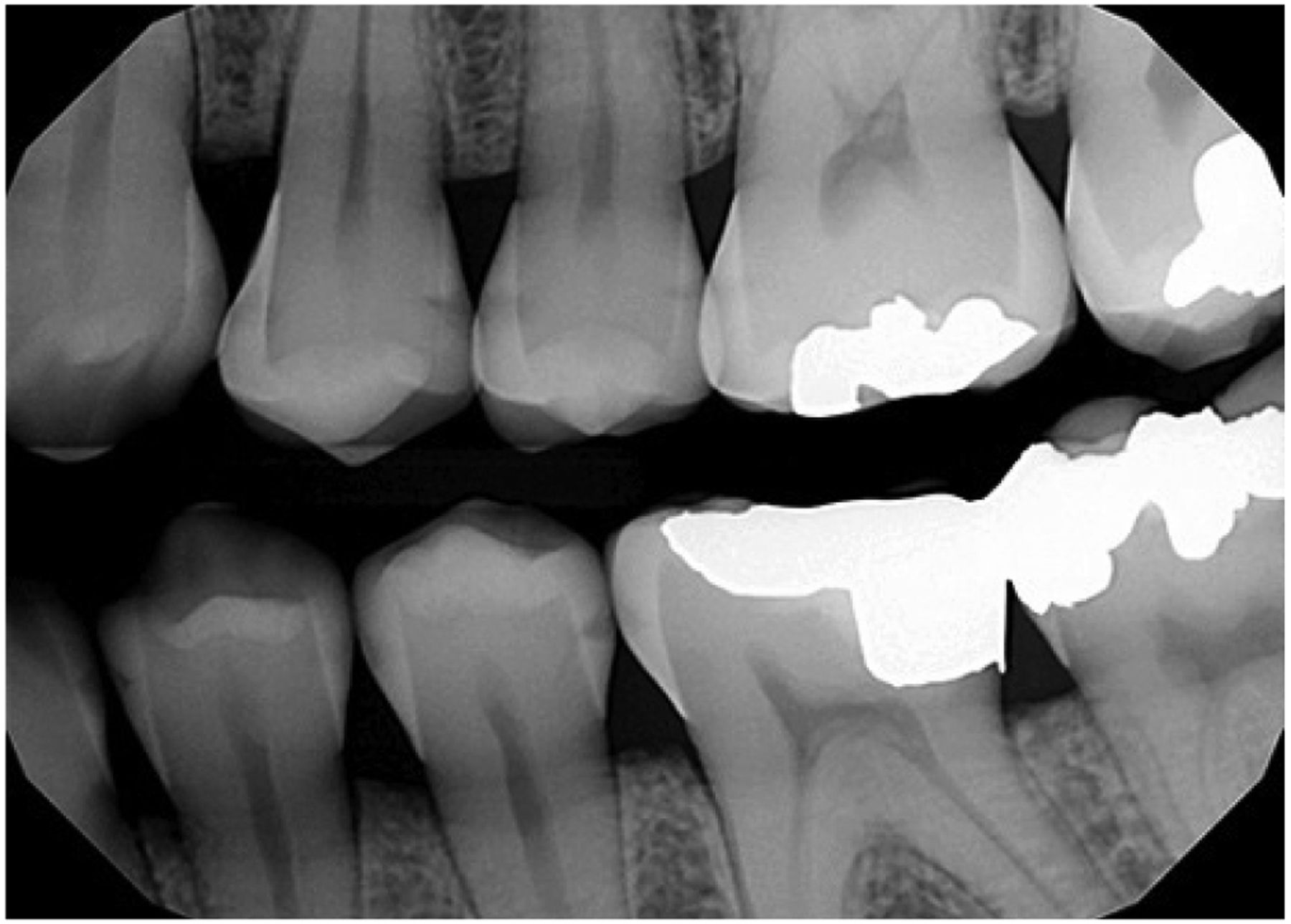
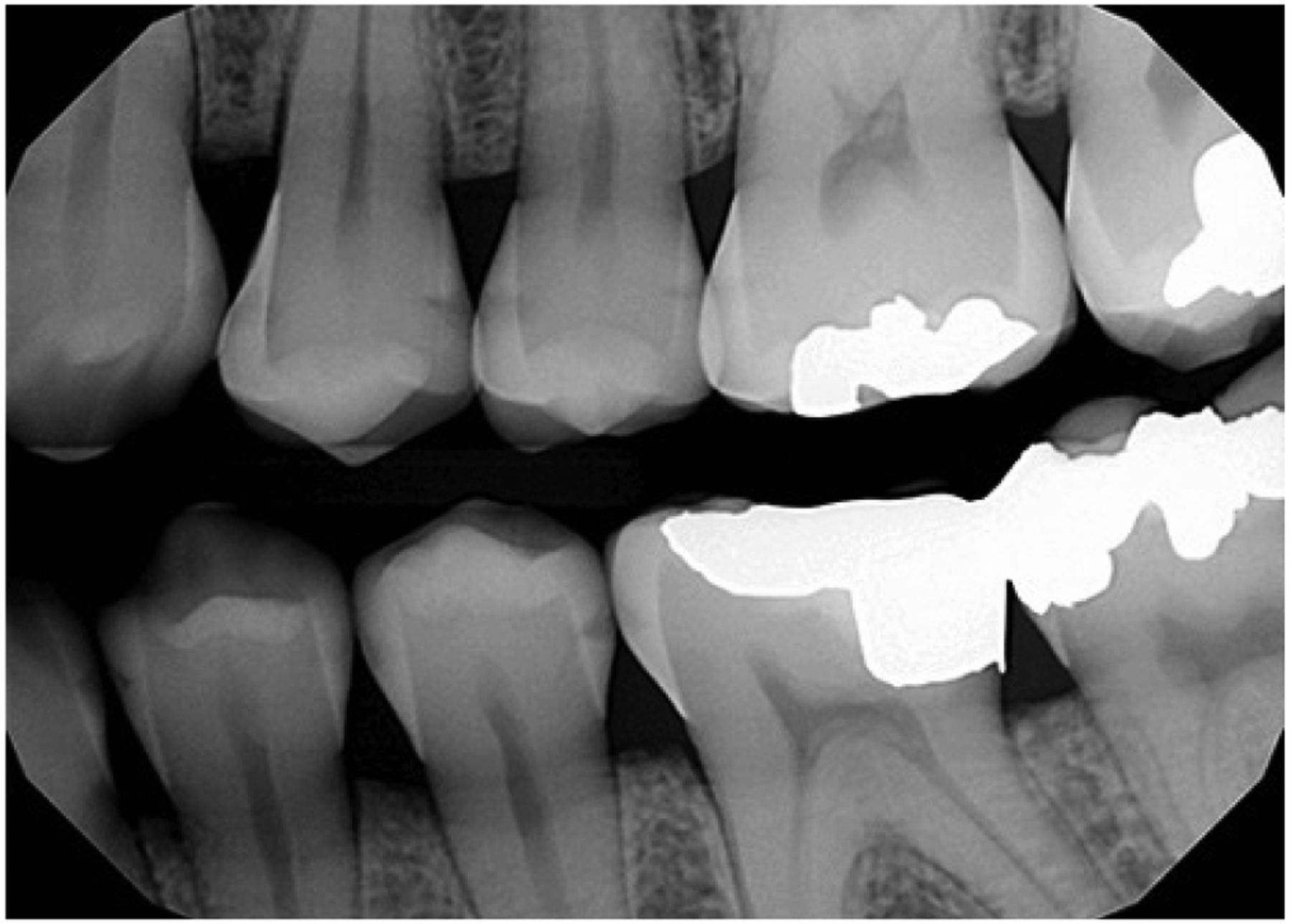
Radiograph of Interproximal Caries
Secondary prevention is employed after the patient has developed a carious lesion but before it has cavitated. Figure 1 shows several interproximal carious lesions. The upper bicuspids appear to have demineralization that extends into the dentin and probably have cavitated. They will most likely require surgical repair. However, the lower bicuspids show examples of demineralization that do not appear to be into dentin. A patient with only early stage demineralization could be managed medically rather than surgically by applying topical fluoride and prescribing 1.1% sodium fluoride or calcium phosphate/fluoride enhanced toothpaste to remineralize early stage lesions. The resulting remineralization would be better quality care than a restoration, because the fluoride would incorporate into the tooth structure and the pH would have to drop significantly before that area would demineralize. On the other hand, placing a restoration would increase the probability that the area would need retreatment at some point in the future. At BCH the result of behavior modification and goal setting along with frequent application of fluoride varnish and home fluoride toothpaste was a reduction in new cavitation of 65%.5 Both of these procedures can be performed by non-dentist health professionals, achieve better health outcomes and cost less than placing restorations.
Levels of Prevention4
In addition to these primary and secondary preventive treatments, BCH used tertiary prevention on cavitated lesions. Many very young children are treated at BCH because their disease is so extensive that they cannot be managed in a clinical setting and they are referred for operating room (OR) treatment under general anesthesia. Because of the high demand at BCH, the waiting time for the OR (prior to adoption of the ECC protocol) was between six and nine months – plenty of time for caries to advance into the pulp or cause the child considerable pain.
The ECC protocol includes removing caries with hand instruments without local anesthesia, applying fluoride varnish and placing an interim therapeutic restoration (ITR) of glass ionomer. This stabilizes the infection and reduces pain, and many of these children were subsequently able to be managed in a clinical setting. This tertiary prevention reduced the need to treat the children in the operating room by 48% at BCH. This is a better experience of care since the use of general anesthesia in young children has inherent risks. Plus, the protocol reduced reported pain by 38%, again a better experience of care. The new ECC protocol was able to reduce the average cost of care for their population of children by 37% in the first year.7
The primary focus of the Patient Protection and Affordable Care Act (PPACA) is to bring down the escalating costs of health care that are threatening the American economy and to improve the quality of care. The goal of the Triple Aim is to simultaneously improve the health outcomes for a population, improve the patient's experience of care, and to lower the per capita cost of care.8 BCH with its ECC protocol was able to achieve the Triple Aim. But one of the challenges to spreading this protocol is the fact that Medicaid and commercial insurers do not cover many of these procedures. They do not pay for disease management or motivational interviewing even though they both can achieve dramatic results. Usually they will pay for only two fluoride treatments in a twelve month period, and the ECC protocol may call for three or more. Many do not cover interim therapeutic restorations. These benefit programs are hesitant to cover additional services because of the potential to provide them to children who are not at high risk and thus would drive up cost without providing additional health benefit.
However, a new opportunity may be developing. The PPACA encourages the formation of Patient-Centered Medical Homes (PCMH) and other Accountable Care Organizations with the belief that they can control costs and improve quality.9 A PCMH is:
“A primary care practice that gives patients the individualized care and support they need to stay healthy…the patient, the primary care physician and a medical team work together to develop and implement a plan of care for the patient that details the patient's optimal medication use, diet, exercise, behavioral health treatments, etc. to get and keep the patient healthy.”10
These types of Patient-Centered Health homes can include dental professionals and could potentially cover other populations besides Medicare recipients. They can share in savings they create. Had BCH been part of a Patient-Centered [Health] Home that qualified to share savings, they could have received substantial payment for achieving their outcomes. Before adopting the ECC protocols, the average cost to the hospital of providing care was $2,023 per child, and after adopting the protocol, it dropped to $1,271, for a savings of $752 per child.7 For their population of 395 children, they lowered their costs by almost $300,000. Had they received just 20% of that expense, they would have more than covered their costs of disease management and extra fluoride, earned additional revenue while also saving the Medicaid program money.
It is possible to expand the use of primary, secondary and tertiary prevention to achieve improved health outcomes, better patient experience of care and lower cost of care, which could allow existing benefit dollars to cover more patients and increase access.
- Copyright © 2015 The American Dental Hygienists’ Association





{kind=link}