



Abstract
Purpose: To explore the oral health perceptions and practices of Vietnamese adolescents 13 to 17 years old in San Jose, Calif.
Methods: A purposeful sample of 10 Vietnamese parents with adolescent children were recruited at a Temple in San Jose, Calif. After gaining parental consent and adolescent assent, Vietnamese adolescents participated in an audio-taped, 20 to 30 minute, individual, semi-structured interview in English to explore their perceptions about oral health. Interview data were transcribed verbatim. All statements related to each question were identified, and similar statements were grouped into categories.
Results: Ten adolescents participated in the study. All reported tooth appearance as the most important reason for oral care, and that oral health, diet and general health were related. All were concerned about dental pain. Of the respondents, 9 believed that having good teeth would give them more confidence, and help them find jobs and romantic partners, while 2 did not follow recommended oral hygiene routines or recognize early signs of disease. Seven participants favored U.S. dentists over Vietnamese dentists. Frequently reported barriers to seeking dental care were fear of dental treatment (n=7) and inability to pay for dental care (n=6).
Conclusion: When educating Vietnamese adolescents, dental hygienists need to highlight availability of pain control, encourage better performance of personal oral hygiene and recommend dental clinics with sliding fee scales to low-income families. This approach to oral health education may enhance dental health and seeking of regular dental visits.
Introduction
The 1999 National Oral Health Survey of Vietnam reported 70% of children had decayed, missing or filled teeth.1 In addition, a 2010 survey of the Vietnamese adult population in Vietnam reported a moderate level of caries (decayed, missing and filled teeth score of 4.98) and a low level of oral hygiene.2
Over 1.5 million Vietnamese have immigrated to the U.S. since 2010, and nearly 40% (581,946) live in California. The U.S. city with the largest Vietnamese population, with over 125,000 people, is San Jose, Calif.3
Vietnamese migrant children in low income families tend to experience disproportionately high rates of dental caries. A 1979 study of 200 Vietnamese refugees of all ages in Germany reported that 43% of primary and 22% of permanent teeth were carious.4 In addition, a 1981 survey in Bergen, Norway reported that newly immigrant Vietnamese teenagers needed about 4 times the treatment for dental caries as Norwegian schoolchildren 12 to 18 years.4
A 1997 study in an urban Canadian population of Vietnamese preschool children reported that 64% of children 18 months of age had dental caries. Contributing behavioral factors were the constant presence of a bottle during the day and at naptime, and the belief that dental decay in primary teeth was not a problem.5,6
An Australian study of Vietnamese speaking parents' practices related to their children's oral health care and risk of disease reported 4 traditional patterns: tooth brushing with salt, delayed introduction of tooth brushing, not visiting dental clinics for preventive care and the use of lay remedies rather than dental care to cure oral pain. Language was identified as a major barrier to attending the child dental service, following notification of treatment need.7 In general, minorities in the U.S., including Vietnamese, suffer from more dental caries and periodontal diseases than Caucasians and non-Hispanics.8 Several California studies of younger children in other migrant situations have reported significant differences in dental caries in various ethnic low income minority groups compared to the rest of the population.6 Moreover, it has been reported that among Asians in general, 14 to 15 year olds have higher periodontal treatment needs than Whites.9
Although no clinical studies have been reported, it is reasonable to suspect that migrant adult Vietnamese in San Jose, Calif are susceptible to dental caries due to its high prevalence in Vietnam among adults. This suspected dental caries among Vietnamese adults in San Jose is a concern since a 2004 international study found that parents' perceptions, beliefs and oral health-related behaviors predicted whether their children had dental caries.10
No studies of the oral health perceptions of migrant Vietnamese adolescents in the U.S. have been reported. It is important, however, to explore this issue since adolescents are approaching a life stage where they will make health care decision. The purpose of this qualitative exploratory study was to develop an understanding of the oral health perceptions and practices of Vietnamese adolescents in San Jose, Calif. Our research questions were: What are the perceptions of Vietnamese adolescents about oral health? What are the oral health practices of Vietnamese adolescents to prevent dental diseases? What are the primary challenges facing them in getting oral care?
Methods and Materials
A qualitative approach based on phenomenography was used to gain an understanding of Vietnamese adolescents' perceptions surrounding oral health. Phenomenography is a way of looking at the world from the interviewee's point of view.11
Study design, Study Population and Pilot Testing
This qualitative, cross-sectional, exploratory study was approved by the University of California San Francisco Institutional Review Board. The study population was a purposeful sample of 10 Vietnamese adolescents, aged 13 to 17 years who attended a Buddhist Temple in San Jose, Calif. None of the study participants were siblings. After developing an interview protocol and guide and gaining parental consent and adolescent assent, the guide was pilot tested for content validity and acceptability of the questions by 6 volunteer Vietnamese adolescents. These adolescents were recruited from the same temple, but had no knowledge of those who were recruited to participate in the study. Based on their feedback, the interview guide was refined.
Exploring a phenomenon to gain insight is a characteristic of qualitative research. Qualitative research requires one to collect data to learn about the views of individuals to generate theories based on participant perspectives. It requires one to obtain detailed information about a few people to learn from the participants in the study and to develop forms, called protocols, for posing general questions so that the participants can provide answers to the questions. Often questions on these forms will change and emerge during data collection. Examples of these forms include an interview protocol or guide that was used in this study.12
Subject Recruitment, Parental Informed Consent, and Adolescent Assent
A Buddhist Temple in San Jose, Calif was selected as the study site because the researcher did not have a role within the Temple community that could affect the honesty of participant response; it offered English classes to Vietnamese adolescents, and had a large Vietnamese population attending the Temple. Parents and their adolescent children were approached concurrently by the bilingual researcher in the reception area of the Temple when the parents dropped off or picked up their adolescent children. The researcher verbally explained the study purpose, risks and benefits, and answered any questions about the study, in Vietnamese if necessary. The researcher, who was unknown to the parents and adolescents, passed out consent forms to interested parents and at the same time passed out assent forms to adolescents in English to establish their willingness to participate in the study. After gaining parental consent and adolescent assent, a date and time were scheduled for an in-person 20 to 30 minute interview in English at the Temple for the adolescent. All participants were interviewed on different days to avoid the potential exchange of information about the questions and answers and the interview process. This approach eliminated the possibility of contact among participants while waiting to be interviewed. Consent and assent forms were kept secure in a locked file cabinet.
Data Collection
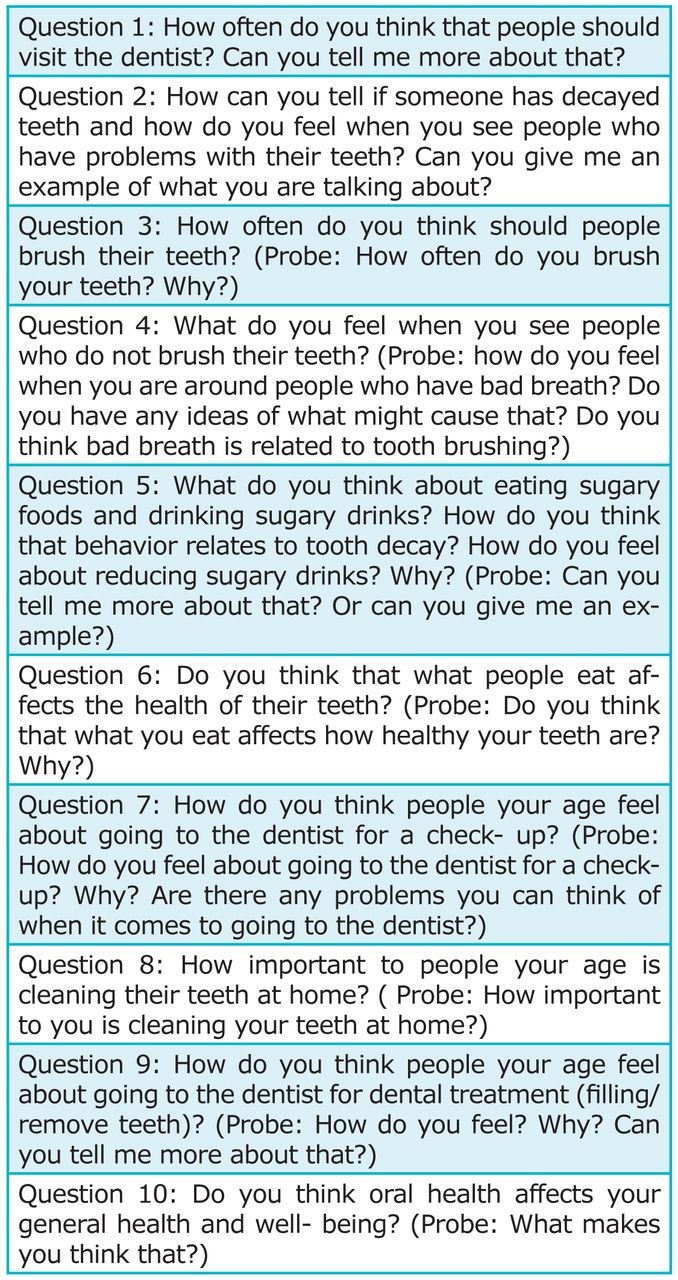
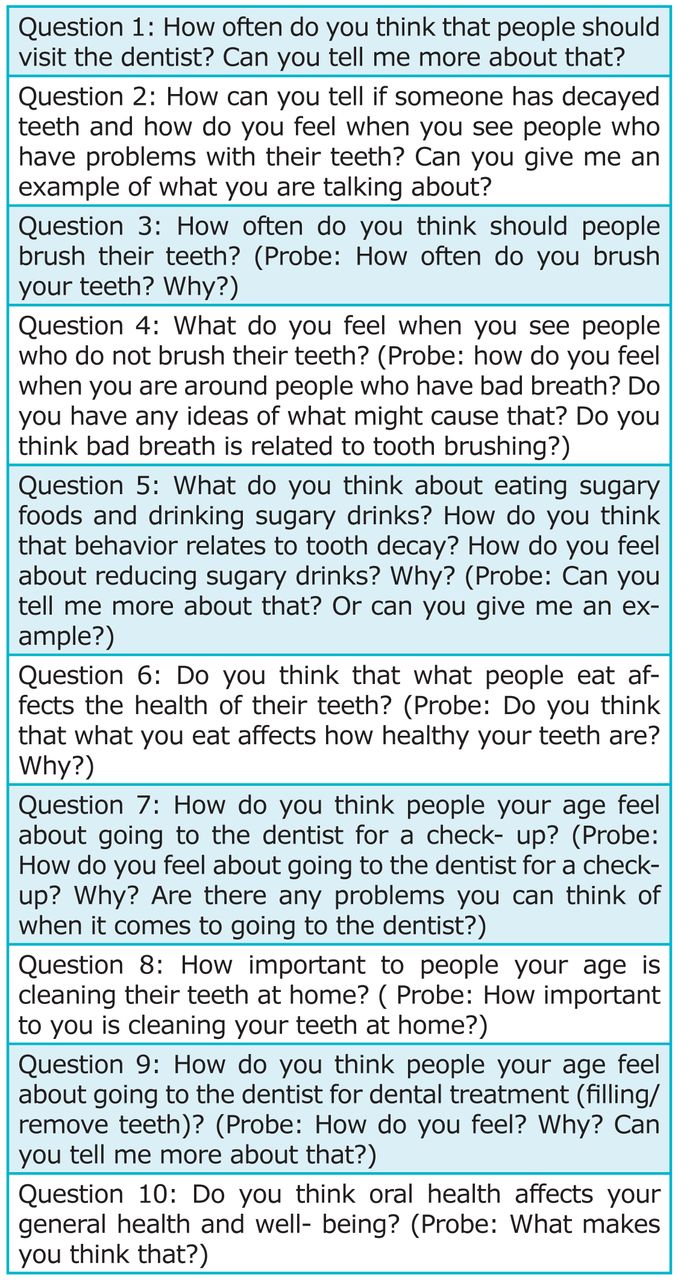
During 2013, individual, digitally-recorded, confidential, semi-structured interviews were conducted using the interview guide in a private room at the Temple for each subject. All semi-structured interviews were conducted by the same investigator. This investigator was the principal investigator, spoke both English and Vietnamese, and underwent training in the interview protocol by another experienced qualitative researcher. The interview consisted of asking demographic questions (gender, age, length in the U.S, place of birth) and 10 open-ended questions that addressed oral health perceptions and behavior (Figure 1). Open-ended questions were used to guide, rather than to direct, the discussion. As described in the consent and assent forms, upon interview completion, the investigator gave each participant a $10 gift certificate as a thank you for study participation.
Data Analysis
Audio-recorded interview data were transcribed by the principal investigator verbatim manually without personal identifiers using Microsoft Word®. Data were stored in a secured password-protected computer stored in a locked office. Audio recordings were destroyed upon study completion.
Data analysis consisted of the following: First, the researcher listened to the tape while reading transcripts to become familiar with the data and correct any transcription errors. Next, all of the transcriptions were read carefully, and the researchers grouped all similar statements into 8 coded categories:
Attitude toward dental visits
Reasons for oral care
Dental experiences
Importance of oral health
Perception of healthy and unhealthy teeth
Diet
Barriers to oral care
Health beliefs and behaviors
Subsequently, the researchers re-read the transcripts to refine the categories. For example, when the responses assigned to the coded categories of “reasons for oral care,” “perception of healthy and unhealthy teeth” and “ health beliefs and behaviors” were reviewed, it became apparent that there was overlap. As a result, responses in the categories “reasons for oral care” and “perceptions of healthy and unhealthy teeth” were combined with some of the responses in the “health beliefs and behaviors” category into a new category entitled “other oral health beliefs.” The remainder of the behavior-related responses in the original category “oral health beliefs and behaviors” were assigned to a new category entitled “oral health behaviors.” Thus, oral health beliefs and behaviors were assigned to separate categories.
In a similar manner, the responses in the category “attitudes toward dental visits” were combined with the category “dental experiences” to create a new category entitled “attitudes toward dentists and dental visits” to eliminate overlap and duplication of responses. As a result of this process, thematic categories decreased from the original 8 categories to the final 6:
The importance of oral health
Attitudes toward dentists and dental visits
Other oral health beliefs
Figure 1:Interview Guide Questions
Oral health behaviors
Diet
Barriers to oral care
The resultant categories were then compared to check if there were any overlapping and duplicating responses within themes. Upon determining that there was no further overlap or duplication of responses, the 6 categories were accepted as unique themes.12 Typical responses - direct quotations - that depict the full range of responses coded together into each thematic category are used here to illustrate main findings upon study completion.
Results
Ten adolescents (50% male, 50% female) were interviewed. The median age was 15 years (range 13 to 17 years) with a median residency length in the U.S. of 6 years (range 4 to 9 years). All participants were born in Vietnam and their native language was Vietnamese.
The 6 major themes discerned in the data are discussed as follows:
Importance of Oral Health
Adolescents considered how their teeth could influence their confidence and perception of others. Most thought oral health was important for social reasons and that appearance of their teeth could affect their careers. Adolescents stated:
“I want to have shiny and white teeth like my friends…I want to have a fresh breath so that I feel comfortable in front of people. I can talk loud and laugh out loud when I have nice teeth. Healthy teeth give you more confidence.”
“You can easily get a job with a beautiful smile. Like if you look for a marketing job or customer representative job. They really want to hire a person with nice teeth…. Easy to find a job, easy to get a boyfriend, and easy to get attention from people. I think I have nice teeth. So I feel very confident in front of my friends.”
Attitudes toward Dentists and Dental Visits
A little more than half of the participants reported positive attitudes toward dentists and the need for dental visits. Sample comments were:
“Dentist will find out if I have any problems and will fix it. Dentist will give me a good education about oral health care so that I know how to take a good care of my teeth.”
“Dental treatment is very important…I would see a dentist right away when I have problems because I don't want to lose my teeth”
“Cleaning helps prevent cavities and remove all the stuffs that you can't do by brushing”
Many reported their dental visits were influenced by families and friends:
“I see my dentist in every six months. My family and most of my friends see the dentist twice a year. This is like our culture and habit … It is up to my parents.”
Some adolescents had a negative attitude about visiting the dentist:
“You don't know what is going to happen when you go there. Scare. I hate getting my teeth out.”
Most of the participants thought U.S. dentists were more gentle than dentists in Vietnam, as demonstrated in the following quotes:
“I had a bad experience about my dentist in Viet Nam when they did a filling. They did not give me anything when they did the filling. It was horrible … The dentist in Viet Nam hurt you a lot, and they don't really talk to you. They just do whatever they need to do. But the dentist in U.S is so nice. They talk to you more. They are very gentle. And especially they give you anesthesia when they do the filling … I scare of the dentist in Viet Nam. But I don't really scare to see a dentist in U.S.”
“I think a dentist in U.S. talk to me more; teach me more about oral care compared to the one in Viet Nam. And dentist in U.S. send me a reminder in every 6 months. And you don't need to get in line to wait for so long like the one in Viet Nam. They give you exactly day and time to come. You don't have to make an appointment when you see the dentist in Vietnam, first come first serve.”
“I had a bad experience with my dentist when I was in my country. They were terrible when they pull my teeth. They did not talk to me and did not numb me at all.”
Other adolescents, however, felt there was no difference between dentists in the U.S. and Vietnam and some even wanted to see Vietnamese dentists in the U.S. because they can speak their language.
“I think dentists in Vietnam and US are the same. They do everything the same. They treat me the same. I think nothing difference.”
“Vietnamese dentist speak my language so it is easier. I can communicate with them more. I can tell them what I want.”
Oral Health Beliefs
Several individuals recognized the relationship of oral health to general health. The following are some sample quotes:
“You will have heart attack and stroke if you have a lot of problems with your teeth. Teeth are also damage to your general health. You will get sick if you have tooth pain cuz you cannot eat.”
“You will have a lot of medical problem if you have bad teeth like you may have periodontal disease and stroke. You may have heart attack and infection as well.”
All of the participants perceived healthy teeth as teeth that have no signs or symptoms of a problem. Many viewed healthy and unhealthy teeth in terms of pain. Several defined a healthy mouth as:
“No cavities, no tooth pain, no bad breath.”
“My teeth are good … I don't have any pain. You can eat whatever you want when you have good teeth. You don't feel sensitive when you eat sweet foods.”
Many defined unhealthy teeth as having:
“Pain, bleeding, red gum, smell bad, and you can't eat anything.”
Some of the participants did not know what infection was. One participant explained:
“I never heard about it [infection]. But I don't think I have one because my parents and my dentist would tell me if I have it.”
Oral Health Behaviors
All adolescents interviewed reported brushing, but not always after breakfast and lunch; some also reported flossing. Sample comments were:
“I brush twice a day and floss once a day … I get up in the morning, brush, and then eat. I brush before I go to bed.”
“I don't have time in the morning [because I have] to run after I have breakfast. And I don't have time at lunch because … I always have lunch with my friends and I like to chat so much so no time to brush.”
“… it is hard to floss and it takes so much time.”
Diet
All of the participants had knowledge about the linkage between diet and oral health. For example, one adolescent explained:
“Whatever we eat will affect the health of the teeth. If you eat unhealthy food, you will have unhealthy teeth … you will have a lot of cavities if you eat too much candies and cookies.”
Some of the adolescents mentioned they eat a lot of sugary foods and drinks:
“[I eat candy] Maybe like four to five times per day and I eat one to two candies each time. I love chocolate.”
“I love coke … But I only drink one a day so I think it is ok … I just like coke. No, I will not reduce it. I love it.”
All of the participants were concerned about their high intake of sugary foods and drinks because they were aware that these substances cause cavities. Some explained:
“… candy caused a lot of cavities.”
“Sweet is always bad for your teeth.”
Some indicated that they wanted to avoid sugary foods and drinks, others said they could not control themselves. For example:
“I really want to reduce it [sugary foods] because I don't want to have any problems with my teeth.”
“I know [candy causes cavities] but I love it. I can't control myself.”
“I love coke even though I know it is not too good for my teeth.”
Barriers to Dental Care
The adolescents were asked about barriers associated with visiting a dentist. The major barrier reported was fear:
“I'm scared of the filling and pulling teeth out. I think it has a lot of pain.”
“I think most of the kids are afraid of teeth removal. I am not an exception.”
Another barrier reported by subjects was the expense of dental care as indicated by the following statements:
“[I] … don't want to go [unless I] … have a pain because it is so expensive. We don't have insurance. We pay cash.”
“If my parents can't afford it, I may not go.”
Another barrier reported by a few was the long waiting time for care:
“Every time we see a dentist, it takes us almost 4 hours. We have to wait for so long. They book so many patients. I hate to wait.”
Discussion
All Vietnamese adolescents interviewed thought oral health was important for social reasons and believed that appearance of their teeth affected their confidence and ability to attract friends as well as influenced their ability to gain employment. This finding is consistent with those of other researchers who found that common health concerns reported by adolescents include those related to appearance and dental health.13-20 In a 7-year cohort study of 2,406 sixth graders in 2 communities in the U.S. who were followed annually through the twelfth grade, physical appearance was found to be the most valued characteristic and the only one that grew in importance over time.20 It appears that relating good dental health with an attractive facial appearance would enhance adolescent motivation to perform recommended personal oral hygiene behaviors.
In this study, most adolescents generally described brushing twice a day, but not always after breakfast and lunch. Although they indicated that they knew they should brush after meals, most talked about brushing before breakfast and not afterwards. Moreover, many said they had no time to brush after breakfast and lunch because they had early school and limited lunch time.
Similarly, with regard to dental floss use, participants talked about not necessarily flossing every day though they knew they should. The findings suggest that when providing care to Vietnamese adolescents, dental hygienists need to reinforce the importance of flossing at least once a day and the best time to brush in relation to food intake; specifically, the importance of brushing after meals, rather than before meals, to reduce acid attacks on teeth as a strategy for preventing dental caries needs to be emphasized. In addition, having adolescents demonstrate correct tooth brushing and flossing technique in their own mouth would ensure competency to perform the behaviors. It was discovered that it is not motivation they need so much as encouragement to act on their knowledge and development of skill by actually engaging in the behaviors.
At least half of the adolescents in the study were aware of the relationship of oral health to general physical health, such as heart attacks and stroke. Nevertheless, half of the participants did not know the meaning of the word “infection” as it related to dental caries and periodontal diseases. These infectious and transmissible oral diseases are caused by microorganisms in oral biofilms as a result of poor oral hygiene.21 Dental hygienists need to discuss the concept of infection and its relationship to dental caries and periodontal infections as part of oral health education to encourage Vietnamese adolescents to perform recommended oral hygiene behaviors.
Although many participants talked about poor oral health in terms of having bad breath, bleeding gums and gum disease, most defined the health of their teeth not in these terms but in terms of the presence or absence of pain. This latter finding suggests a lack of understanding of the early signs of cavities and gum disease and that although early dental problems can be painless they should be treated before they become painful. Thus, dental hygienists need to educate their Vietnamese adolescent clients about the early signs of cavities or gum disease, how to recognize them, and how to respond properly to address them. Pointing out in an adolescent's own mouth such things as a white spot lesion as a sign of early dental caries and bleeding gums as a sign of early gum disease to promote understanding of how to detect problems early is recommended. If no problems are seen in the individual's mouth, then use of color pictures of such problems in another's mouth also can enhance awareness of how to recognize signs of problems early. In addition to having regular dental exams, educating adolescents on use of topical fluorides to re-mineralize early carious lesions, and having them demonstrate the proper use of floss in their own mouth, will help promote understanding of how to address problems early.
Most of the participants reported positive attitudes toward dentists and having regular dental visits, but their dental visits were influenced positively by families and friends. Other studies on adolescents have reported similar views about dentists and the importance of family support in accessing care.22,23
In this study, all of the adolescents realized the importance of the benefits of having healthy teeth. These findings are consistent with those found in the 2009 California Health Interview Survey of Adolescents that reported approximately 70% of adolescents in California had their last dental visit less than 6 months previously and only 0.9% had never visited the dentist.24 The 2007 California Health Interview Survey of Adolescents reported that adolescents living below the federal poverty guidelines were more likely to report that the condition of their teeth was fair or poor than were adolescents whose families had higher incomes.25 This finding suggests that the positive attitudes toward oral health among study participants might be due at least in part, by socio-economic status. Although not directly assessed, and based on the fashionable clothes worn by the respondents many of whom owned cell phones, the bilingual field researcher observed that most participants appeared to come from families with a modest but not affluent income, rather than very low income families. Nevertheless, it would have been helpful to have collected quantitative data on socioeconomic status since that is a known factor in oral health status. Indeed, the cost of dental care was an issue with the participants and there is no evidence that these students were not from a low-income household.
Most of the interviewees thought dentists in the U.S. were gentler and better communicators than dentists in Vietnam. This finding suggests that educational explanations by dental hygienists would be equally well received. It is important to note, however, that some respondents wanted to see Vietnamese dentists in the U.S. because they spoke their language.
While all of the participants were concerned about their high intake of sugary foods and drinks because they were aware that sugar caused cavities, more than half of the participants said they had trouble controlling themselves when it came to consuming sugary foods and drinks. This association between adolescents' diet and knowledge of dental caries has been reported by others.22 The findings also are consistent with those of the 2011 California Health Interview Survey of Adolescents that reported 22% of adolescents between 12 to 17 years of age consumed 2 or more glasses of sugary drinks a day.24 Dental hygienists need to focus on sources of sugar in the diet among Vietnamese adolescents. For example, recommending the use of non-sugar snacks to replace chocolate and candy consumption and discussing the importance of drinking fluoridated water rather than sugary drinks to promote oral health would be consistent with the findings.
Fear of dental treatment and the expense of dental care were the most frequently reported barriers to visiting the dentist. Fear of pain from dental treatment based on past dental experiences, especially in Vietnam, was a universal concern among our study participants. Dental hygienists need to highlight the availability of pain control in dental settings to help address this barrier. Moreover, emphasis should be placed on the point that early detection and treatment of problems could eliminate the need for later treatments that may require more invasive or distressing work by the dentist.
Despite the apparent modest income appearance of these teenagers, the expense of dental care was a frequently reported barrier for seeking dental care. Similar findings have been reported elsewhere.25 Recommending dental clinics with sliding fee scales to low-income Vietnamese parents may help decrease this barrier and increase access to care.
This study has several limitations. First, the findings are limited due to the inability to reach data saturation on all aspects of some questions. However, for many questions more than half the adolescents agreed with each other or gave the same responses, some degree of data saturation was reached for certain aspects of those questions/topics. Second, there could be sample selection bias due to the small sample size and the convenience sampling technique. Participants were recruited from only one particular location - the Buddhist Temple in San Jose, Calif. Study participants may have been more supportive of oral health care than those adolescents who did not participate in Temple activities. Therefore, the study findings cannot be widely generalized. Third, although the interview guided questions were tested for content validity, they were not tested for reliability.
Conclusion
The purpose of this qualitative exploratory study was to develop an understanding of the oral health perceptions and practices of Vietnamese adolescents in San Jose, Calif. Based on the findings conclude that when educating Vietnamese adolescents, dental hygienists need to highlight: the importance of oral health to physical appearance, the availability of pain control in dental settings, and the importance of flossing at least once a day and brushing after meals to prevent dental caries and periodontal disease infections. Recommending dental clinics with sliding fee scales to low-income Vietnamese parents may help increase access to care. The role of parents and friends serving as external factors to promote oral health among adolescents appears to be important but needs to be further studied. Findings from this study offer valuable first insights into migrant Vietnamese youths' understandings about oral health and provide a basis
Acknowledgments
The authors wish to thank Barbara Heckman for her assistance with the UCSF Committee on Human Research application process. We also wish to thank the Duc Vien Buddhist Temple in San Jose and the Vietnamese parents and adolescents who participated in this study.
Footnotes
Kelly Pham, MS, RDH, works in clinical practice in San Jose, California. Judith C. Barker, MA, MSc, PhD, is a Professor, Dept. Anthropology, History & Social Medicine, and Associate Director, Center to Address Oral Health Disparities, University of California San Francisco. Ann A. Lazar, PhD, MS, is an Assistant Professor, Department of Preventive and Restorative Dental Sciences, University of California, San Francisco. Margaret Walsh, MA, MS, EdD, RDH, is a Professor Emerita and Director of the Master of Science Degree Program in Dental Hygiene, Department of Preventive and Restorative Dental Sciences, University of California San Francisco.
This study supports the NDHRA priority area, Health Promotion/Disease Prevention: Assess strategies for effective communication between the dental hygienist and client.
- Copyright © 2015 The American Dental Hygienists’ Association





{kind=link}