



Abstract
Purpose: This study assessed the oral health knowledge, confidence and practices of Virginia personnel in the Special Supplemental Food Program for Women, Infants and Children (WIC).
Methods: In 2009, 257 WIC personnel were electronically emailed via an investigator-designed 22-item Survey Monkey® questionnaire. Descriptive statistics, Chi-square and Fishers Exact tests compared personnel demographics and oral health knowledge, confidence and practices at the p≤0.01 and 0.05 significance level.
Results: Response rate was 68%. WIC personnel were knowledgeable about basic oral health concepts. More than half of those reporting were not confident assessing for visual signs of dental decay and do not routinely assess for visual signs of decay. Only 4% of personnel apply fluoride therapy.
Conclusion: Findings support the need for health promotion/disease prevention at WIC.
- early-severe childhood caries (E-SCC)
- fluoride varnish therapy
- oral health promotion knowledge confidence and practices
- WIC personnel
Introduction
Early-severe childhood caries remains a significant public dental health issue in the U.S. and internationally.1 The most common chronic disease in children, dental caries is 5-times more prevalent than asthma and 7-times more prevalent than hay fever.2 Approximately 19% of U.S. children aged 2 to 4 have experienced visually detectable dental decay. Data from the National Health Nutrition Examination Survey (NHANES) reveal that the number of children aged 2 to 5 with dental caries increased from 24 to 28% from 1999 to 2004.3 Nineteen percent of U.S. children aged 2 to 4 have visually detectable dental caries.4 Overall, children of poverty experience more extensive dental disease and have less access to dental care.5,6 For example, 25% of children living in poverty have not seen a dentist before the age of 5, experience twice the dental caries as their more affluent peers and are more likely to have untreated oral disease.4-6
In 2005, the Virginia Department of Medical Assistance Services introduced the Smiles For Children (SFC) program, providing coverage for diagnostic, preventive and restorative/surgical procedures, as well as orthodontic services for Medicaid, Family Access to Medical Services Plan (FAMIS) and FAMIS Plus children.7 The program also provides coverage for limited medically necessary oral surgery services for adults age 21 and older. Reasons cited by parents for not involving their children in preventive dental programs or establishing an ongoing dental provider or dental home include the inability to take time off from work, living a transient lifestyle and being unable to find a dentist who participates in the SFC program.7-11 Dentists are reluctant to participate in SFC because of the perceived low fee-for-services reimbursement, and high no-show rates for appointments undermining profit margins.12 Since 2005, provider participation has more than doubled. Children receiving dental services has increased, from 24 to 45%.7
The U.S. Public Health Service and Department of Health and Human Services (DHHS) also documented substantial barriers to oral health preventive measures. These barriers include lack of access to community water fluoridation in rural areas. Although 95% of Virginia residents are receiving the recommended community fluoridated water levels, others living in rural areas have difficulty in accessing SFC.13,14 Lack of dentists, and the need to expand access to professional oral health care services, has led to training of non-dental providers and dental hygienists in public health programs to screen children for oral disease, educate parents on nutrition, encourage use of preventive modalities and refer children to participating dentists who can prevent or treat early-severe childhood caries.13-15
A population-based health program to improve children's overall health is the Special Supplemental Nutritional Program for Woman, Infants, and Children (WIC). Originated in 1972 from the Federal Assistance Program of the Food and Nutrition Service (FNS) of the United States Department of Agriculture (USDA), WIC provides food to supplement the diets of millions of lower income women, infants and children under the age of 5, breastfeeding promotion and support strategies, dietary counseling, and referrals for welfare/social services and health care.16 The WIC program benefits pregnant and breastfeeding women during critical times of their infant's growth and development and encourages health promotion practices in the prevention of childhood obesity, infant mortality, and other lifestyle, diet-related or chronic diseases. Some participants may receive more frequent health and nutritional counseling from WIC program personnel (nutritionists, dieticians and nurses) than from their children's pediatricians. Participation, eligibility requirements and the complicated application process vary by state.16
The purpose of this study was to assess the current oral health promotion knowledge, confidence and practices of WIC personnel to improve the oral health of WIC participants. Does Virginia WIC personnel knowledge, confidence and practices provide insight to build programs and extend training to both dental and non-dental health professionals?
Severe–Early Childhood Caries
The Centers for Disease Control (CDC) uses the term early childhood caries (ECC) or severe-early childhood caries (S-ECC) for the occurrence of rampant decay in infants and toddlers.17 S-ECC is the most common chronic, preventable dental disease affecting smooth surfaces of primary teeth (Figure 1).18 The American Academy of Pediatric Dentistry (AAPD) defines S-ECC as the presence of 1 or more decayed noncavitated or cavitated decayed lesions, missing teeth, or filled tooth surfaces in any primary tooth in a child 71 months of age or younger, or any sign of smooth-surface decay in children younger than 3 years of age.19
S-ECC is caused by a complex interaction among cariogenic microorganisms, fermentable carbohydrates and susceptible teeth.20-22 Using selective detection, Tanner et al identified Scardovia wiggsiae in the mouths of children with severe ECC when other pathogens were not detected.23 Microorganisms play a major role in tooth demineralization and vertical transmission of caries from a mother or caregiver to child through close contact, shared food utensils and saliva.24-27 The earlier the microorganism colonizes the primary teeth, the more likely the demineralization process begins.27

Clinical Signs of Severe–Early Childhood Caries17
Li and Caufield's27 longitudinal study of 34 mother-infant pairs determined how infants acquire pathogenic bacteria.6 Bacterial samples were obtained at 3-month intervals from mothers and their infants to approximately 3 years of age. Almost 71% of infants and toddlers showed DNA patterns harboring genotypes of bacterial microflora identical to those of mothers. Female infants were 6-times more likely to match their mother's genotypes. Male infants and toddlers were 13-times more likely to exhibit dental decay and the MS strain than female children, even though male infants usually have later tooth eruption. This finding remains unexplained until future immunology research is conducted. Researchers strongly suggest that mothers are the major source of MS transmission to their infants and toddlers and recommended future immunology studies.23-27
Palmer et al found food frequency, cariogenicity and bacterial pathogenesis to be associated with S-ECC and caries recurrence.26 Bacteria metabolize carbohydrates or liquids, initiating acid demineralization of tooth enamel. A combination of bacteria, saliva, defective tooth about the transmission of bacteria enamel, parental behaviors and attitudes increases S-ECC risk.26
Oral Health Promotion
Caries control should start prenatally with screening and treating the mother. Following birth, the infant should be screened and parent and child provided with continued preventive care throughout childhood.24-26 First dental care visits for infants and toddlers should occur by 12 months of age or when the first tooth erupts.19,20,25 To monitor the caries balance, infant's knee to lap examinations are recommended biannually by the American Academy of Pediatrics (AAP).28 Periodic fluoride varnish therapy, parental counseling and establishing a relationship with a dental provider has been shown to be effective in reducing S-ECC.28-31 Fluoride varnish frequency is recommended every 6 months for children at high risk for dental caries, according to the Medicaid Early and Periodic Screening, Diagnosis, and Treatment Benefits Program (EPSDT).31 Varnish therapy can also be applied up to 4 times annually.
According to Bandura's Social Learning Theory, human behavior is acquired through observation, experience, modeling, self-efficacy, confidence and positive reinforcement.32 Self-efficacy and self-confidence are qualities for promoting behavioral change.33 Positive reinforcement of oral health concepts and behavior by WIC educators and parents results in positive behavioral and clinical outcomes for children and parents.33-34 Oral health education aimed at parents or caregivers in the WIC program can improve children's dental and overall health.35-39
Schick and Rozier conducted a 1 year study of North Carolina nutritionists' effectiveness in oral health promotion among WIC participants.40 Researchers found nutritionists with a greater sense of self-efficacy and outcome expectancy were more confident in oral health promotion. The nutritionists were more likely to perform oral risk assessments, counsel parents and make dental referrals than those who lacked confidence.40 One study revealed nurses and dental hygienists were more likely to discuss oral health promotion if they were more confident in oral health practices.41 Pediatricians with greater confidence in oral health screening for dental decay were more likely to make referrals of Head Start children than those with lower self-confidence.42 Physicians' confidence in ability to screen for risky health behaviors was positively related with the promotion of disease preventive practices.43 WIC nutritionists often see children before they see a dental health professional.37-41 Therefore, WIC nutritionists' ability to examine for caries, promote oral health practices, and make referrals is important in preventing S-ECC in low-income populations.
Yost and Li suggested that nurses apply anticipatory oral health guidance for infants and children.24 For example, this guidance includes teaching caregivers to use a damp, warm washcloth to clean infant's gums after eating and before bedtime, putting an infant to bed with a bottle containing water rather than one with fermentable carbohydrates, and avoid on-demand breastfeeding during night. After tooth eruption, caregivers should clean their infant's mouth with a washcloth and slowly progress to a soft child toothbrush. A pea-size or smear of toothpaste should be introduced at approximately 18 to 24 months of age and hands-on parental or caregiver toothbrush instruction should be taught and reinforced.25 Researchers emphasize the importance of making the first dental visit within 6 months of tooth eruption or by 12 months of age.19,25,28
Weinstein, Harrison and Benton demonstrated that motivational interviewing (MI) techniques are helpful in reducing or preventing S-ECC by counseling mothers during the first year following the birth of a child.34 MI is a collaborative, client-centered form of guiding to elicit and strengthen motivation for change.33,34,36 MI focuses on skills to educate and motivate others in making health-promoting behaviors based on a client's stage of readiness.34,35 Children in the MI group exhibited significantly less new caries. The guardians and/or parents of 2 year olds displayed greater compliance with recommended fluoride varnish treatment regimens than the control group without the MI. Weinstein and associates concluded that MI intervention improves health-promoting behaviors of mothers and their young children at high risk for dental caries.34
Freudenthal and Bowen examined MI techniques to decrease parental risk-related behaviors for S-ECC.36 Positive changes in valuing oral health, permissiveness, change difficulty and openness to health information were studied in a population of WIC mothers in Southeast Idaho using a pre- and post-test questionnaire. Avoidance of sharing utensils during feeding and number of times per week mothers brushed or cleaned their child's teeth significantly increased in the group of mothers exposed to the MI counseling techniques. Researchers concluded that using MI with diverse populations at WIC sites would most likely have a positive impact on oral health practices.36
Oral Health Confidence
Oral health confidence among WIC providers studied by Butani et al found those with some oral health training are more likely to counsel mothers and their children about dental disease prevention than WIC providers void of confidence and oral health training.37 Nurses were most likely to discuss oral health issues with WIC clients when compared to other WIC providers. Furthermore, the researchers observed that providing appropriate oral health training to WIC providers increases their confidence and encourages discussion of oral health issues and S-ECC prevention with clients.37 Researchers recommend oral health training for WIC personnel so that they are comfortable with current dental concepts for improving the oral health status of their WIC clients.37
Nurko et al compared the prevalence of caries in children (n=120) of parents or caregivers who had participated in the WIC Infant Oral Health Educational Program (IOHEP) to children of parents who never participated.38 Participants were mostly of Hispanic descent, ages 1 to 5. Parents at the WIC program received counseling and participated in a survey and children in both groups had their decayed and filled teeth (DFT) scores evaluated by pediatric dental faculty and pre- and post-doctoral students. Findings revealed that children whose parents participated in an IOHEP experienced significantly fewer overall caries from 57 to 39% following a 5 year IOHEP community-based program. Findings support oral health promotion by WIC personnel on oral hygiene instructions, proper diet and nutrition, and periodic fluoride applications aimed at reducing the incidence of S-ECC.37-39
Underserved preschool-aged children rarely visit a dentist, and often receive their first oral screening and dental referral through a public health program such as WIC or Head Start. Virginia Division of Dental Health implemented a Maternal and Early Childhood Oral Health Program called Bright Smiles For Babies.44 This program followed the structure used by North Carolina's Into the Mouths of Babes program.39,40,44,45 Virginia's's Bright Smiles For Babies program offers oral health training to non-dental personnel in occupations who legally can apply fluoride varnish and bill Medicaid, i.e., physicians, physician assistants, pediatric nurse practitioners, family nurse practitioners and registered nurses.44 Effective July 2008, the Pharmacy Act allows dentists or physicians to provide standing orders for dental hygienists or nurses to place fluoride varnish on the teeth of children 6 months to 3 years of age at home visits, pediatric and immunization clinics, WIC clinics, and other health district programs.45 To operationalize the Pharmacy Act, WIC personnel should first be trained on the demineralization-remineralization process, caries risk and protective factors, oral health risk assessment and screening, oral health information documentation, and prevention guidance to WIC children and families.45
Bright Smiles For Babies training is comparable to the Open Wide training for health professionals available through the National Maternal and Child Oral Health Resource Center.44,46 In 2009, Virginia's Division of Dental Health began a pilot project allowing dental hygienists who hold a Virginia license issued by Virginia Board of Dentistry (Sec.54.1-2722) under a remote oral health care model to provide educational and preventive dental care in designated dental professional shortage areas.45
California has the nation's largest number of WIC sites (n=82). In 2001, WIC began First Smiles with dental services provided once a week using portable dental equipment. After 2005, the application of fluoride varnish was introduced. First Smiles' goal is to significantly reduce the incidence of dental decay in young children. Dental and medical providers are trained to increase the number of dental visits for at-risk 1 year olds. Since few dentists treat low-income one year olds, California WIC programs collaborate with dental providers to treat the WIC participants at selected WIC sites.15
Lee and Rozier compared dental services among children enrolled at WIC to those not enrolled at WIC.39 Children participating in WIC programs are more likely to use preventive and restorative services and less likely to use emergency services than non-WIC participants. Since WIC program participants fall below the 185% Federal Poverty Level, all are considered high risk for dental decay.
Methods and Materials
After approval from Old Dominion University College of Health Sciences Human Subjects Committee, a pilot study of 15 nursing students and 32 dental hygiene students was conducted to determine reliability of a test-retest procedure for a 22-item investigator-designed questionnaire. Content validity was established involving a panel of experts (20 dental hygiene graduate students and faculty). Once revisions were made and validity and reliability were established, a cover letter and questionnaire were electronically mailed via Survey Monkey® to a convenience sample of 257 WIC personnel provided by the Virginia Department of Health Services WIC director.48 For inclusion, participants had to be professional staff members with direct contact with WIC clients (children, prenatal or postpartum women, or children's guardians). Anonymity was insured by not requiring names on the questionnaire instrument, and data were reported in group-form among districts only. A questionnaire was selected as the instrument of choice as the large geographically diverse sample could be assessed cost effectively, respondents' anonymity could be maintained and the questionnaire completed at their own leisure.
Questionnaire content was guided by the knowledge, confidence and practice objectives of the overall study and the review of the literature. The objectives investigated WIC personnel oral health knowledge, confidence and practices to help improve access to care for underserved communities. Some questions were derived from previously developed and tested questionnaires.36,37,41 The instrument asked WIC personnel about their demographic characteristics: age, sex, race, educational level, job title, WIC district and years employed at WIC. Lickert-type questions obtained information on oral health knowledge, confidence and practices.
Four items on oral health knowledge were self-ranked as: knowledgeable, not knowledgeable or no opinion. Five items measuring confidence on oral health confidence were self-ranked as: confident, not confident and no opinion. Six items on oral health promotion practices were ranked as: frequently, never and no opinion. For the last question, item 23 (not included in Survey Monkey®), respondents were emailed in October 2010 asking if they received any oral health training at WIC.
Statistical analysis was performed using Survey Monkey® and SPSS 18 (Statistical Package for Social Science, Inc., Chicago).48 Data were nominal or ordinal scaled and discrete. Descriptive analysis was calculated within Survey Monkey®. Inferential analysis between respondent demographics and their oral health knowledge, confidence, and practices were identified using bivariate analysis with Pearson Chi-square and Fisher's exact test. The test of independence was set at one and the level of significance was p≤0.05 in knowledge, confidence and practices (Table I, II and III) and p≤0.01 (Table I and III).
Results
Respondents were dispersed uniformly throughout Virginia. The 42 Virginia districts were categorized as either rural or urban for comparison purposes (Table IV).49 An incentive Target gift card raised the response rate from 64 to 68%. The first analysis of 176 subjects revealed no statistically significant difference in subjects' demographics and oral health knowledge, confidence and practices. A total of 17 subjects were eliminated because they completed less than 75% of the questionnaire or were WIC office service specialists or administrators who worked indirectly with WIC clients, and 159 participants were used in the final statistical analysis resulting in a 62% final response rate. The sum of percentages reported may not equal 100% due to rounding.
Descriptive statistics identified that, except for 4 male respondents, the WIC respondents (n=153) were female with 2 respondents' sex unreported. The predominated age range was between 50 to 59 (n=61) (Figure 2).
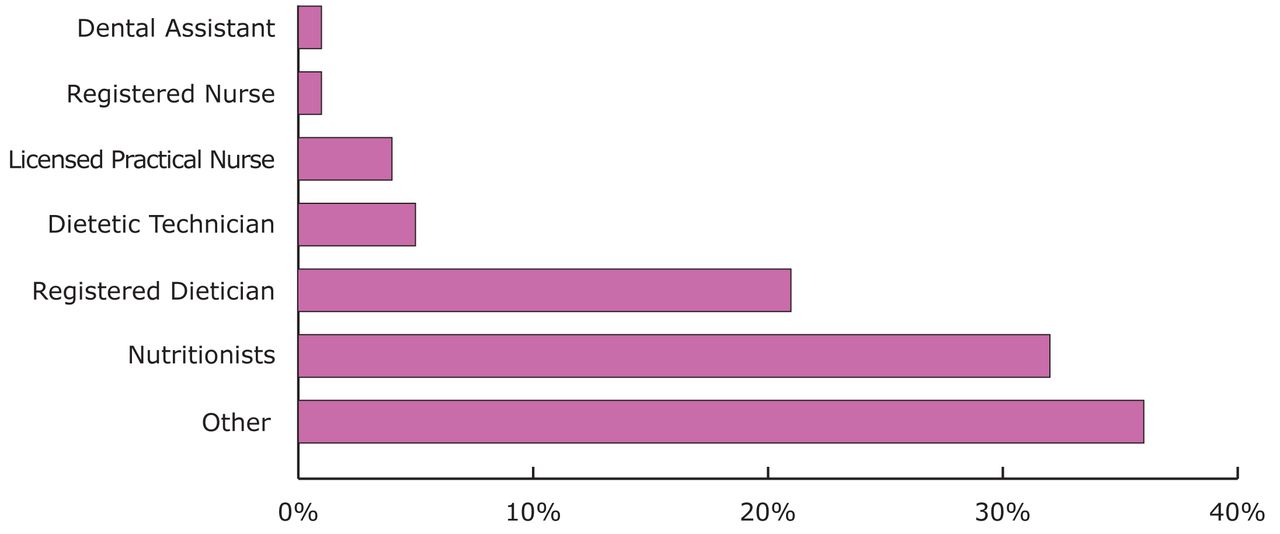
The majority of WIC personnel were White (n=105), followed by Black (n=36), Asian (n=8), multi-racial (n=5), American Indian (n=1), Native Hawaiian (1) and 3 ethnicities unreported. Office service specialists (n=58) and nutrition associates or assistants (n=50) were the predominant occupations followed by registered dieticians (n=32), dietetic technicians (n=8), licensed practical nurses (n=6) and registered nurses (n=2). No registered dental hygienists were in the sample; however, there were 2 former dental assistants and 3 respondents not reporting occupation (Figure 3).
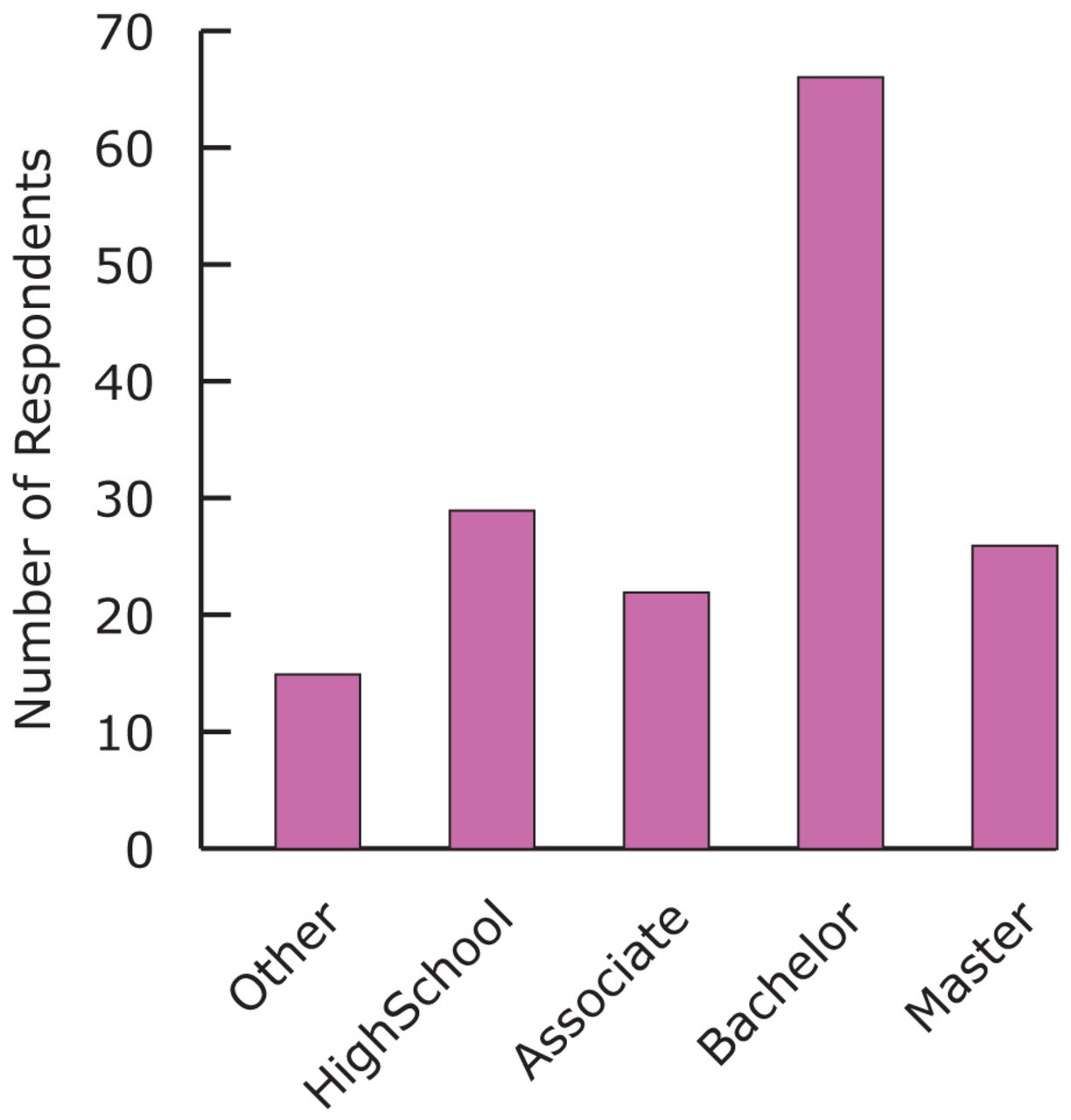
Respondents predominately reported earning a bachelor's degree (n=66), followed by a high school diploma (n=29), master's degree (n=26), associate's degree (n=22), other (n=15) and non-reporting (n=1). The majority of respondents (n=90) were employed at WIC for over 10 years followed by 6 to 10 years (n=26), 3 to 5 years (n=18), 1 to 2 years (n=16), less than 1 year (n=8) and 1 non-reporting.
Knowledge: A total of 94% of WIC respondents who were aged 40+ years indicated they were significantly more knowledgeable about oral bacterial transmission compared to 83% of respondents aged 18 to 39. A total of 97% of WIC respondents who had 10+ years of experience were significantly more knowledgeable about oral health transmission compared to 87% of WIC respondents aged 18 to 39. A total of 87% of WIC respondents who were aged 40+ years indicted they were knowledgeable about the dental decay process compared to 72% of aged 18 to 39 respondents. Respondents ages 40+ and 10+ WIC experience were 0.01 significantly more knowledgeable (Table I).
Confidence: A total of 90% of WIC personnel with education beyond high school were significantly more confident in explaining oral health-related dietary habits compared to 75% of WIC respondents with a high school diploma. A total of 64% of respondents (n=101) reported they were not confident in performing oral assessments, while 31% (n=49) were confident in their ability to perform an oral assessment. No statistically significant difference (p>0.05) was found between confidence and WIC personnel demographics, their performing oral health assessments for dental decay, their referrals made to dentists, their providing oral hygiene instructions and advising families about fluoride supplements or treatments. The researchers were 95% confident the results did not occur by chance and that WIC personnel aged 40 and over or possessing education beyond high school were confident in explaining oral health dietary habits (Table II).
Self-Reported WIC Ages and Experience with Knowledge and Practices
Self-Reported Oral Health Promotion Confidence
Self-Reported Districts and Practices
Practices: Less than half of WIC respondents assessed their children for visual signs of dental decay. About 53% of WIC respondents aged 40+ years assessed clients significantly more than 28% of respondents in the 18 to 39 year bracket at the 0.01 level. About 87% of WIC respondents who had 10+ years of WIC experience provided significantly more parental counseling on toothbrushing than those with less than 10 years of experience. WIC respondents who were significantly more likely to refer participants to dentists were over aged 40 years, and had greater than 10 years of experience at WIC. Rural WIC respondents were significantly advising parent/guardian on fluoride supplements or treatments more than urban WIC respondents. Urban WIC respondents significantly referred WIC participants to a dentist more than rural WIC respondents at the 0.01 level (Table III).
Discussion
Results suggest that the majority of WIC personnel who responded to the convenience survey are knowledgeable about oral health and confident in making dental referrals for infants and children as needed. Findings also suggest that WIC personnel are familiar with AAPD referral guidelines.19 A noteworthy finding of this study is the majority of WIC personnel who were not confident in performing visual oral assessments to identify dental decay in children. Less than half of WIC personnel stated they assessed for visual signs of dental decay suggesting that this is an important area for future training. This finding can be explained by the Bandura self-efficacy social cognitive theory, which states that the greater one's self-efficacy for successfully completing a task, the more likely that a person is to engage in the task.32,33 Training in dental caries assessments is indicated to increase both oral health knowledge and confidence of WIC personnel in identifying dental decay.

Percentages of WIC Respondents Occupations
Few studies have focused on confidence and oral health promotion behaviors by WIC personnel, however, a number of studies in pediatric medicine and nursing demonstrate the effects of practitioner self-confidence on professional practices.37,41,43 For example, one study revealed nurses and dental hygienists more likely promoted oral health if they were more confident in the process, supporting the need to build confidence in oral health promotion and disease prevention in WIC personnel.39 Silverstein found that pediatricians with greater confidence are more likely to make dental referrals at Head Start program populations than those with lower self-confidence.42 Also, Ozer found that physicians' confidence in their ability to screen for risky health behaviors was positively related with their promotion of disease preventive practices.43 If WIC personnel are to help decrease dental disease in their clients, then the research evidence supports the need for additional and regular training to boost confidence and oral health promotion practices.
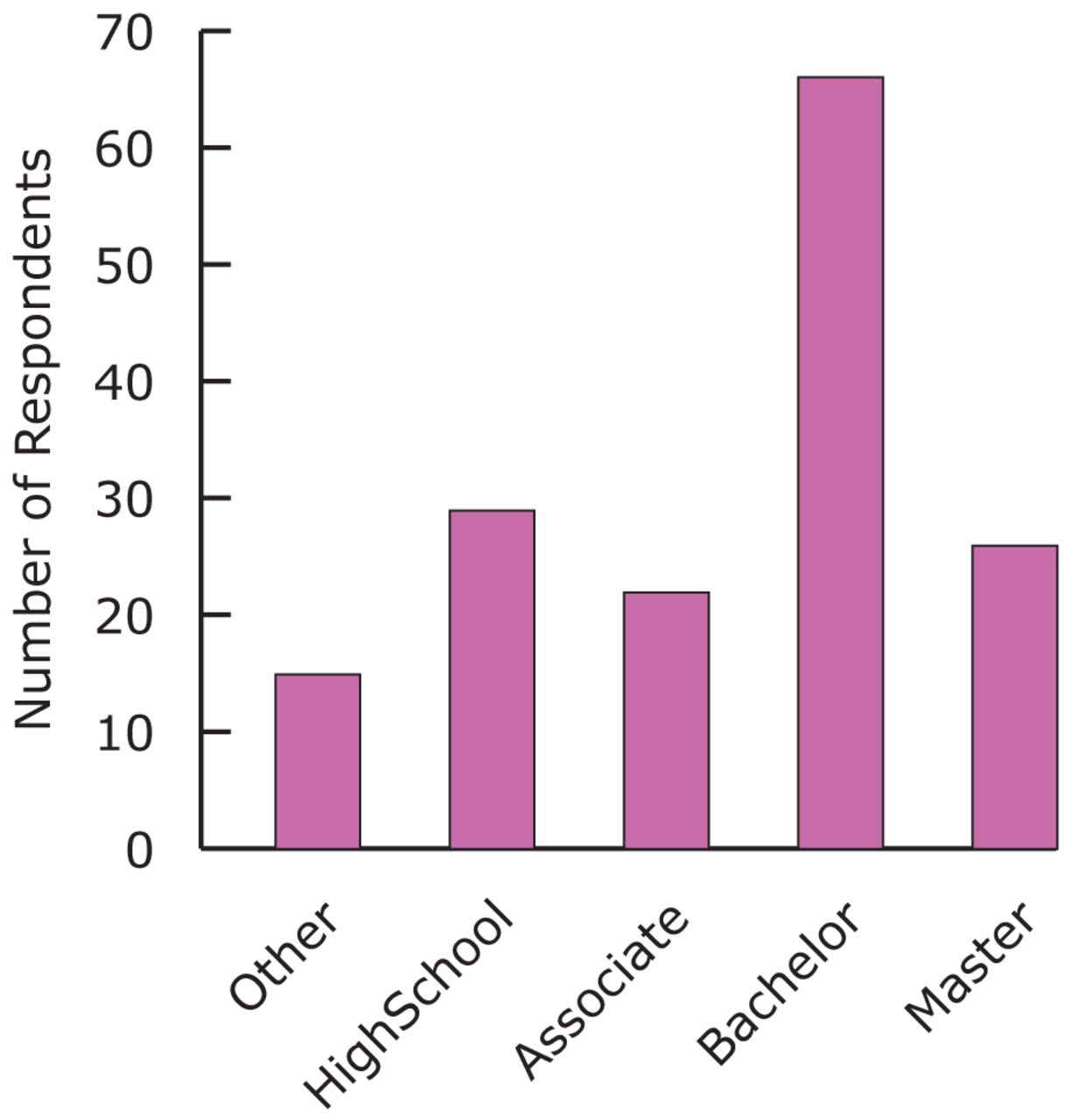
Educational Levels of WIC Respondents
Only 4 out of the 176 respondents apply fluoride varnish on WIC children since registered nurses, dental hygienists, physicians and dentists are permitted to apply fluoride varnish. Given that most WIC personnel were office service specialists and nutritionists, and not nurses or dental hygienists, it is understandable that fluoride therapy is not routinely provided to WIC clients in some WIC programs. The Health Resources and Services Administration (HRSA), California Healthcare Foundation, Institute of Medicine (IOM) and National Research Council (NRC) experts believe separating oral health care from overall care is limiting access to oral care for many Americans.15,47,50
Virginia Health Districts and WIC Personnel Frequencies (n=42)
Recommendations include proper training of non-dental health professionals to assess for dental diseases and implement preventive oral care services in a variety of settings. Some alternative training models to help improve access to oral care in underserved communities include Minnesota Advanced Dental Therapist (DT), Dental Therapist (DT), Alaska Dental Health Aide Therapist (DHAT), California Registered Dental Hygienists in Alternative Practice (RDHAP), Oregon Expanded Practice Dental Hygiene Permit (EPP), Oral Preventive Assistants (OPAs) and Community Dental Health Coordinators (CDHCs).50 These allied dental health models were designed to promote oral care for the underserved and dental professional shortage areas. Strategies to recruit dental providers in underserved communities include: option for new graduates with loan repayment, gaining experience working with the underserved and expanding the scope of practice for dental auxiliaries. Clearly, if more health professionals employed at WIC could apply fluoride varnish, caries activity in the infant and children population would decrease.
Future research could include surveys for WIC clients and other allied health providers to assess their oral health knowledge, beliefs and practices. Additional studies about the use of fluoride varnish knowledge and practices should also be conducted. A cost-effectiveness study to explore the value of other allied health professionals and dental health providers in reducing the need for expensive dental care in WIC populations is also indicated. This line of research may lead to identifying potential cost saving programs for states whose budgets are already depleted by Medicaid, SCHIP, and other entitlement programs.
Conclusion
There is a need for WIC personnel and other allied health professionals in the state of Virginia to receive oral health promotion and dental disease prevention training. Topics to consider include oral health assessments, basic evidence-based practices such as hands-on toothbrush instruction, fluoride varnish and referring to dentists. This could also be accomplished by employing more dental providers at WIC. This study and current literature suggests that oral health training among non-dental professionals such as WIC personnel could reduce the incidence and prevalence of dental decay in the high-risk population of infants and children. WIC personnel make logical partners to collaborate with Virginia Division of Dental Health and the HRSA for support in providing oral health education and basic preventive services to WIC participants.
Footnotes
-
Lorraine Ann Fuller, RDH, MS, is currently employed at Tahoe Family Dentists. Sharon C. Stull. CDA, BSDH, MS, is a Lecturer and Community Health Coordinator, as well as Program Director for both the BSDH Degree Completion Program and Study Abroad at Old Dominion University School of Dental Hygiene. Michele Leonardi Darby, BSDH, MS, is professor emeritus at the Old Dominion University School of Dental Hygiene. Susan Lynn Tolle, BSDH MS, Professor, University Professor, Director of Clinical Affairs.
-
This study supports the NDHRA priority area, Health Promotion/Disease Prevention: Validate and test assessment instruments/strategies/mechanisms that increase health promotion and disease prevention among diverse populations.
- Copyright © 2014 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}