



Abstract
Purpose: In 2004, the attitudes toward and use of automated external defibrillators (AEDs) by Ohio dental professionals were examined. While willing to use an AED, most did not have access to one. With new AED-related legislation and increased awareness of the benefits of AEDs since the initial study in 2004, the purpose of this study was to document the prevalence of and attitudes toward AED usage in the dental setting 7 years following the initial study.
Methods: A 2 page survey instrument was mailed to a random sample of 1,629 dentists and 1,801 dental hygienists in Ohio.
Results: A 24% overall response rate was achieved (36% dentists and 64% hygienists). Data were analyzed using SPSS. Results indicate 16% of respondents experienced a cardiac emergency in their practice that required contacting emergency personnel. AEDs are available in 48% of dental practices. Comparing the 2004 and 2011 data, statistically significant differences were found between the responses of dentists and dental hygienists.
Conclusion: While hygienists reported more positive attitudes toward AEDs than dentists, the majority of all respondents feel AEDs should be mandated in the dental setting. These findings suggest an increase in cardiac emergencies in Ohio dental settings, an increase in the prevalence of AEDs in Ohio dental settings and that the perceptions of dental professionals are changing in favor of the use of AEDs in the dental setting since the 2004 study.
Introduction
The American Heart Association (AHA) reports that sudden cardiac arrest (SCA) is the leading cause of death in the U.S. and Canada.1 An arrhythmia, the most common of which is ventricular fibrillation (VF), causes SCA. The only known treatment for VF is defibrillation.2 In the mid-1990s, defibrillation was added to the AHA chain of survival.3,4 An automated external defibrillator (AED) is a small portable device commonly used to treat VF occurring outside of hospitals.1,3 They are commonly found in airports, sports arenas and other public venues.5
While any person can experience SCA, certain populations are at a greater risk, including elderly and medically-compromised individuals. Due to a longer-living population, dental practices are seeing more medically-compromised and aging patients. Due to the risk of SCA in the dental setting, many dental schools include training on AEDs as part of their emergency medical curriculum.6 Additionally, the AHA recommends the placement of AEDs in at-risk locations, such as medical and dental offices.7
At-Risk Nature of the Dental Setting
Many patients experience physical stress and anxiety as a result of dental treatment, increasing the risk of SCA. Accordingly, dental professionals review and collect medical histories as part of their pre-treatment assessment to identify risk factors for potential cardiac emergencies.8 Additionally, dental professionals are educated to screen patients to assess risk. Blood pressures and blood glucose levels are routinely taken, allowing dental professionals to monitor existing or screen for undiagnosed conditions.9
Following these reviews, dental procedures may be invasive, causing physical stress to the patient. In addition, the dental professional may provide various levels of conscious sedation or administer local anesthesia and nitrous oxide.10,11 These procedures, combined with dental patients' pain, such as abscess or tooth ache, result in the presence of physical and cardiac stressors associated with at-risk areas.3
Dental fear and anxiety have been documented as a concern in the dental setting.12-14 Dental fear can range from a patient being mildly anxious to avoiding dental care altogether. Avoidance of dental care can often lead to emergency situations, increasing the patient's need for more complex treatments.12 Anxiety can lead to physiological symptoms and cardiac stressors such as increased heart rate and blood pressure.13,14 Research has found that even routine events, such as radiographs and the presence of dental hygiene instruments, can increase dental fear.12,13 An observation study by Georgelin-Gurgel et al found that the sights and sounds involved with endodontic procedures increased heart rate and blood pressure in patients and recommended the need to monitor vital signs during stressful dental procedures.13
Basic Life Support Training in Dental Education
To prepare dental professionals to deal with SCA and other cardiac emergencies, AED training usually begins in the educational environment and continues throughout their careers. Dental students are generally trained to respond to cardiac emergencies in dental school, and many dental schools include training on AEDs as part of their emergency medical curriculum. A survey of emergency medical training in accredited U.S. dental schools documented CPR and AED training within their curriculums, however, training was neither consistent nor exhaustive in all of the schools. While over 90% of the schools stated they offered training on AEDs, not all schools included CPR training and recertification courses. Seven percent reported they do not offer CPR recertification. Moreover, 2 schools reported offering medical emergency training as an elective course instead of a requirement.6 These findings are inconsistent with the Standards for Pre-Doctoral Dental Education, stating in standard 2–27 that “graduates must be competent in providing appropriate life support measures for medical emergencies encountered in the dental office setting.”10
Dental hygiene education standards are more prescriptive. Standard 6–5 states that “All students, faculty and support staff involved with the direct provision of patient care must be continuously recognized/certified in basic life support procedures, including healthcare provider cardiopulmonary resuscitation with an Automated External Defibrillator (AED).”11 The standard indicates that the student should be able to perform life support measures necessary to the delivery of quality health care. These educational standards, despite some inconsistent results in the research, further demonstrate the significance of AEDs in the dental office setting.
Dental Practice Recommendations
The American Dental Association (ADA) Council on Scientific Affairs suggested that dental offices may want to include AEDs in their medical emergency kits and that all dental professionals maintain training in basic life support (BLS).15 The ADA provides further recommendations in Guidelines for the Use of Sedation and General Anesthesia by Dentists, stating that, during deep sedation procedures, an appropriate defibrillator must be immediately available.16
Despite these recommendations, practice requirements relating to BLS and AEDs continue to vary from state to state. For example, the American Dental Hygienists' Association (ADHA) reports that 45 states require CPR training as part of state continuing education requirements for dental hygienists.17 The ADA State Government Affairs department provided a list of 35 jurisdictions, including Puerto Rico, requiring CPR training for initial licensure or as continuing education.18 Ohio dental hygienists must be certified in health care provider CPR with AED training, while dentists have no CPR training requirement for licensure or renewal. Accordingly, it is not surprising that the Ohio state dental board does not require AEDs in dental offices.19
Conversely, several states now have requirements regarding AEDs in the dental setting. In 2006, Florida was one of the first states to mandate the presence of AEDs in the dental office setting as part of the minimum standard of care.20 The Washington State Department of Health issued regulations in 2009 requiring any dental office administering anesthesia to have an AED available.21 In 2010, Illinois required all dental offices administering anesthesia or sedation to have at least one AED on the premises at all times. All of these states also have some form of CPR certification requirement in connection with licensure of both dentists and dental hygienists.22-25 Some states, such as Wisconsin, specifically reference AED proficiency for dentists and dental hygienists.25
While state legislation, professional recommendations and professional requirements have generally made CPR, AED training and the presence of AEDs standards for public care, little data currently exists to document the presence of AEDs in dental settings or the attitudes of dental professionals toward their use. A study by Kandray, Pieren and Benner in 2004 examined the attitudes and use of AEDs in the dental office setting of Ohio dentists and dental hygienists.26 While this study found that Ohio professionals would be willing to use an AED if one were available, most dental professionals did not have one available for use.
Since the original study was conducted, the Ohio legislative environment has changed. The Ohio legislature enacted House Bill 143 into law on May 12, 2006, allowing Ohio dental hygienists to administer local anesthesia after taking a board-approved course. Additionally, the Ohio legislature passed House Bill 190 in May 2010, establishing the Public Health Oral Supervision Program, which allows dental hygienists to work under certain circumstances in the absence of the supervising dentist in alternative practice settings such as nursing homes, schools, hospitals and public institutions.27 These changes expose dental professionals to more potential medical emergencies, including SCA. Due to these legislative changes and increased awareness of the benefits of AEDs in the 7 years following the initial study, the purpose of this study is to document the prevalence of AED usage in the dental office setting 7 years following the baseline data and to further explore the attitudes of dental professionals toward the use of AEDs in the dental setting.
Methods and Materials
Research Design
This study employed a non-experimental descriptive survey research design. The survey instrument developed for the original study was used so comparisons could be made between baseline data and data collected for this study. The 2011 survey instrument was modified from the previous exploratory study to include questions that would further examine the perceptions and attitudes of Ohio dental professionals regarding AED usage in the dental setting.
Subjects
A random sample of Ohio dentists and dental hygienists were surveyed. In order to generate the sample, lists of licensed dental professionals were obtained from the Ohio State Dental Board. The Statistical Package for the Social Sciences (SPSS) was used to derive the random sample.
A priori calculations of required sample size were computed using G-Power software version 3.0.5.28,29 The power analysis was conducted for analysis of variance (ANOVA) using the effect size of size (f) convention 0.25.30 The use of 7 groups in the final ANOVA analysis, a medium effect size of 0.25, an alpha of 0.05 and power of 0.95 indicated a final target sample size of 343. A minimum random sample of 1,629 dentists and 1,801 dental hygienists, for a total of 3,430 dental professionals, was surveyed to reach the target sample size (assuming a 10% response rate and reflecting the current licensing proportions).
Instrument/Data Collection
To survey dentists and registered dental hygienists on their use of and attitudes toward AEDs in the dental setting, the researcher sent an initial mailing to the random sample of licensed dentists and dental hygienists to gather the self-reported data. This study was approved by the local Social Sciences Internal Review Board at the University of Missouri – Kansas City. The initial mailing included a cover letter, a 2 page survey instrument and a postage-paid return envelope. Two weeks after the initial mailing, follow-up reminder post cards were mailed to the entire sample.
The survey instrument contained 2 parts. Part 1, comprised of questions from a survey instrument used by the investigator in 2004, included close-ended questions seeking to obtain categorical descriptive data and information regarding the presence and usage of AEDs in the dental setting (coded yes=1, no=2). Two questions were added to document the age (age coding: 18 to 30=1, 31 to 40=2, 41 to 50=3, 51 to 60=4, 61 to 70=5, 71 and older=6) of the participant and to ascertain the prevalence of CPR incidents outside the dental setting. One potentially-leading question, regarding perceived barriers, was revised from the original instrument to remove potential bias. Part 2 included questions to determine the dental professional's attitudes regarding AED usage in the dental setting. These questions were close-ended ranked questions utilizing the Likert scale (5=strongly agree, 1=strongly disagree) to measure the attitudes and beliefs. The survey instrument was developed using a systematic process to ensure validity and reliability.
Analysis
An exploratory analysis including measures of central tendencies, descriptive frequencies, t-tests, Chi-squared tests and correlations examining different group variables were completed using SPSS. Additionally, ANOVAs were completed to determine if a relationship/correlation existed between the independent and dependent variables.
Results
Comparison of 2004 and 2011 Demographics
A 24% response rate was achieved compared to 33% in 2004, with a 64% response rate for dental hygienists compared to a 59% response rate in 2004. Hygienists continue to be the majority of the respondents. Private practice was the most common practice setting (Table I). Several participants checking “other” indicated their work environment was governmental, military or correctional facilities. Most continue to indicate that they work in general dentistry (Table II). Of those who indicated they worked in “other” practice types, the most common description was orthodontics. Education was a new category of practice type added in the 2011 survey. The majority of professionals continue to report full-time employment status (Table III), defined as 30+ hours per week.
2004 and 2011 Descriptive Comparisons
A comparison of the descriptive responses from the 2004 and 2011 surveys are identified in Table IV. A new question in the 2011 survey indicated that 12% of respondents reported performing CPR outside the dental setting. While nitroglycerine use remained the same, some individuals in the 2011 survey who responded they had not administered nitroglycerin to a patient in the dental chair wrote remarks such as “Patients have taken nitro before, but I have them place it in their own mouths.”
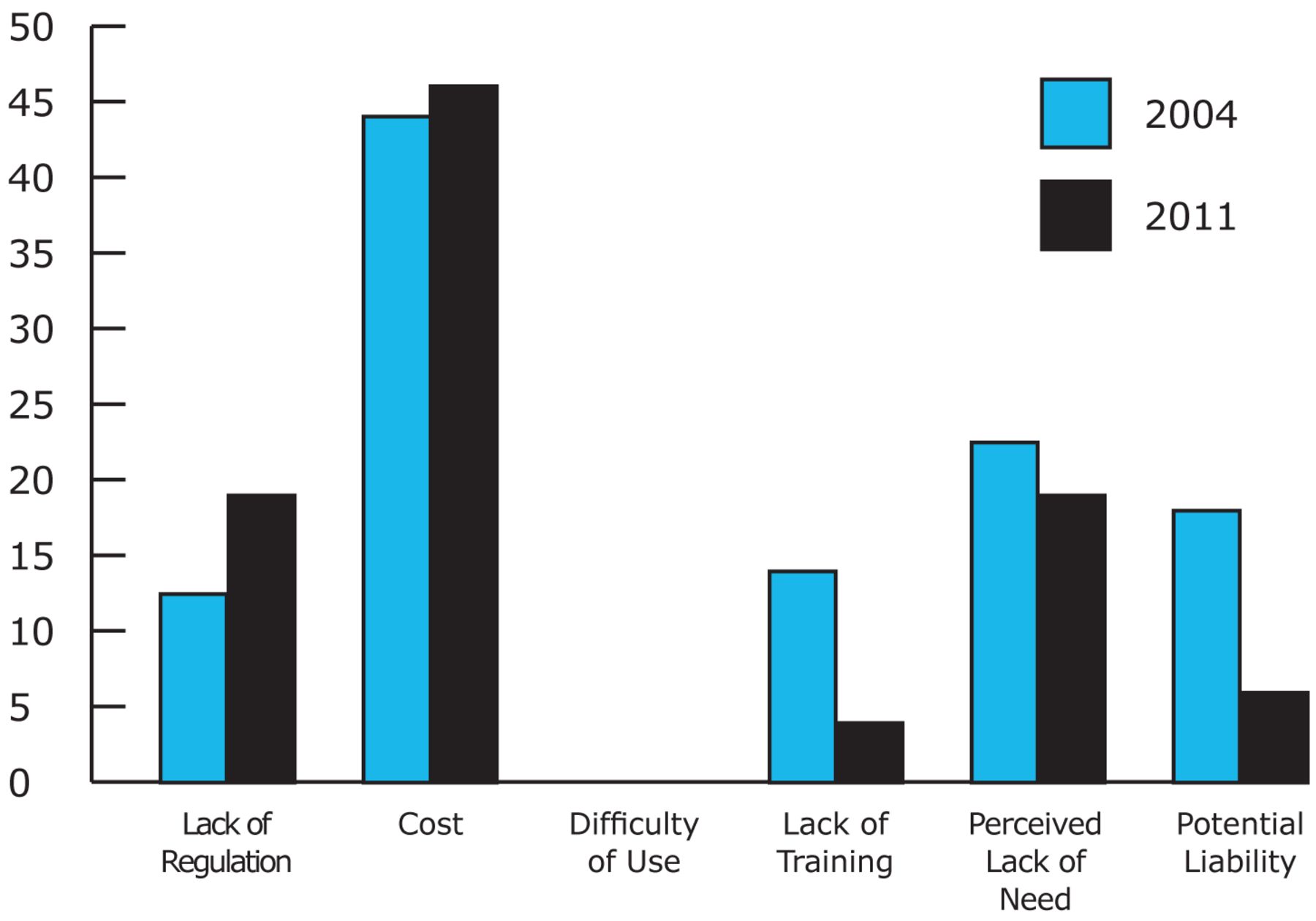
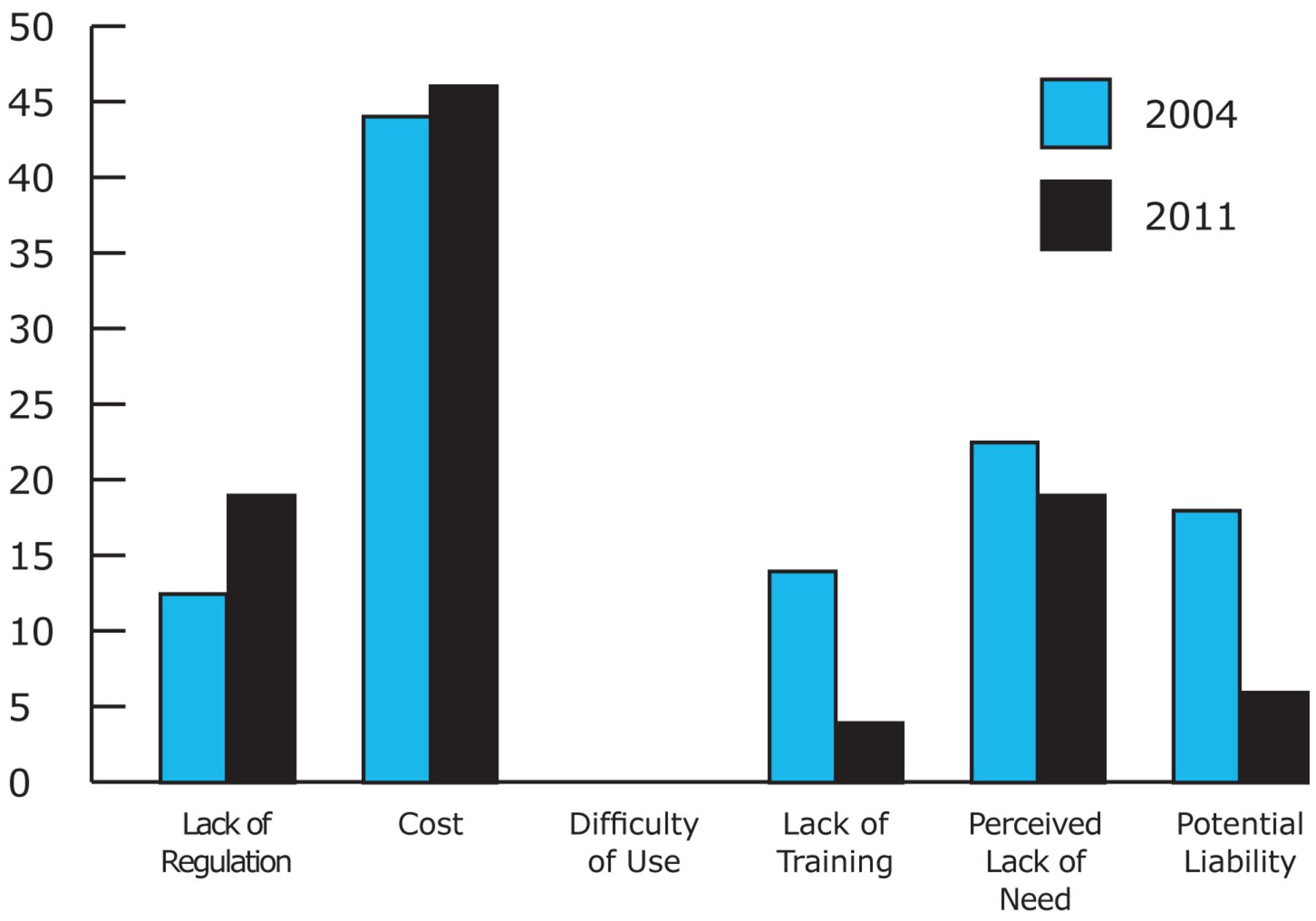
Both 2004 and 2011 respondents indicated that cost was perceived as the most significant barrier to having an AED available in the dental setting (Figure 1). Perceived lack of need was the second most selected barrier. Fewer respondents indicated lack of training was a barrier in 2011. Additionally, perceived potential liability decreased as a perceived barrier in 2011.
Significance testing was completed, including chi-square analysis and Pearson correlations, comparing the study participant responses. Significant changes (p=<0.05 or less) are shown in Table V. More respondents in 2011 indicated that their CPR certification included training for the Health Care Provider or Professional Rescuer, they had training on an AED and they had called emergency personnel for a cardiac emergency for a patient. Fewer professionals in 2011 had to perform CPR in the dental setting than in 2004. The number of respondents with an AED available increased in 2011 from those responding in 2004. More professionals indicated in 2011 that AEDs should be mandated, an AED is important in the dental setting and they would use an AED if available.
Comparison of 2004 and 2011 Work Settings for Dentists and Hygienists
Comparison of 2004 and 2011 Practice Types for Dentists and Hygienists
Comparison of 2004 and 2011 Employment Status for Dentists and Hygienists
Significant differences were found between the responses of dentists and dental hygienists when comparing the 2004 and 2011 data (Table VI). Dentists were more likely to contact emergency personnel for a cardiac emergency, administer nitroglycerin and perform CPR in the dental setting.
Comparison of 2004 and 2011 Responses for Dentists and Hygienists
Negative correlations were noted regarding CPR certification and profession (Table VI). More hygienists reported being certified in CPR as well as being certified as a Health Care Provider or Professional Rescuer in CPR. More hygienists indicated that they had received training on AEDs. Hygienists were more likely to indicate that an AED was important in the dental setting and should be mandated.
2011 Significant Findings
Due to the significant correlations when comparing the 2004 and 2011 data, the 2011 data was further analyzed independently using Pearson correlations and ANOVA tests. Significant correlations were noted between profession and the variables reported in Table VII. Hygienists were younger than dentists. Dentists were more likely to call emergency personnel, perform CPR and administer nitroglycerin to patients. However, hygienists were more likely to report positive attitudes regarding AEDs, indicating that AEDs should be mandated and that AEDs were important in the dental setting. Dentists didn't feel as strongly as hygienists regarding mandating AEDs in the dental setting. Hygienists (M=3.91, SD=1.10) also indicated on a Likert scale that they felt they had more of a legal obligation to use an AED if needed than dentists (M=3.20, SD=1.41) (r(786)=0.272, p=<0.01).
Perceived Barriers to AEDs in the Dental Setting
Significant correlations were noted in the 2011 data between the following variables. Respondents with an AED available in their setting were more likely to indicate that AEDs were important (r(701)=0.315, p=<0.01) and should be mandated (r(653)=0.350, p=<0.01) in dental settings than those who did not. Professionals who were certified in CPR were also more likely to indicate that AEDs were important (r(624)=0.186, p=<0.01) and should be mandated (r(575)=0.082, p=<0.05). Those who had received training on AEDs were more likely to have an AED available (r(740)=0.140, p=<0.01), more likely to feel they were important (r(698)=0.119, p=<0.01), and more likely to feel that they should be mandated (r(650)=0.129, p=<0.01).
Significant Differences in Responses from 2004 versus 2011 for Dentists and Hygienists (p=<0.05)
2004 and 2011 Significant Correlations - Profession
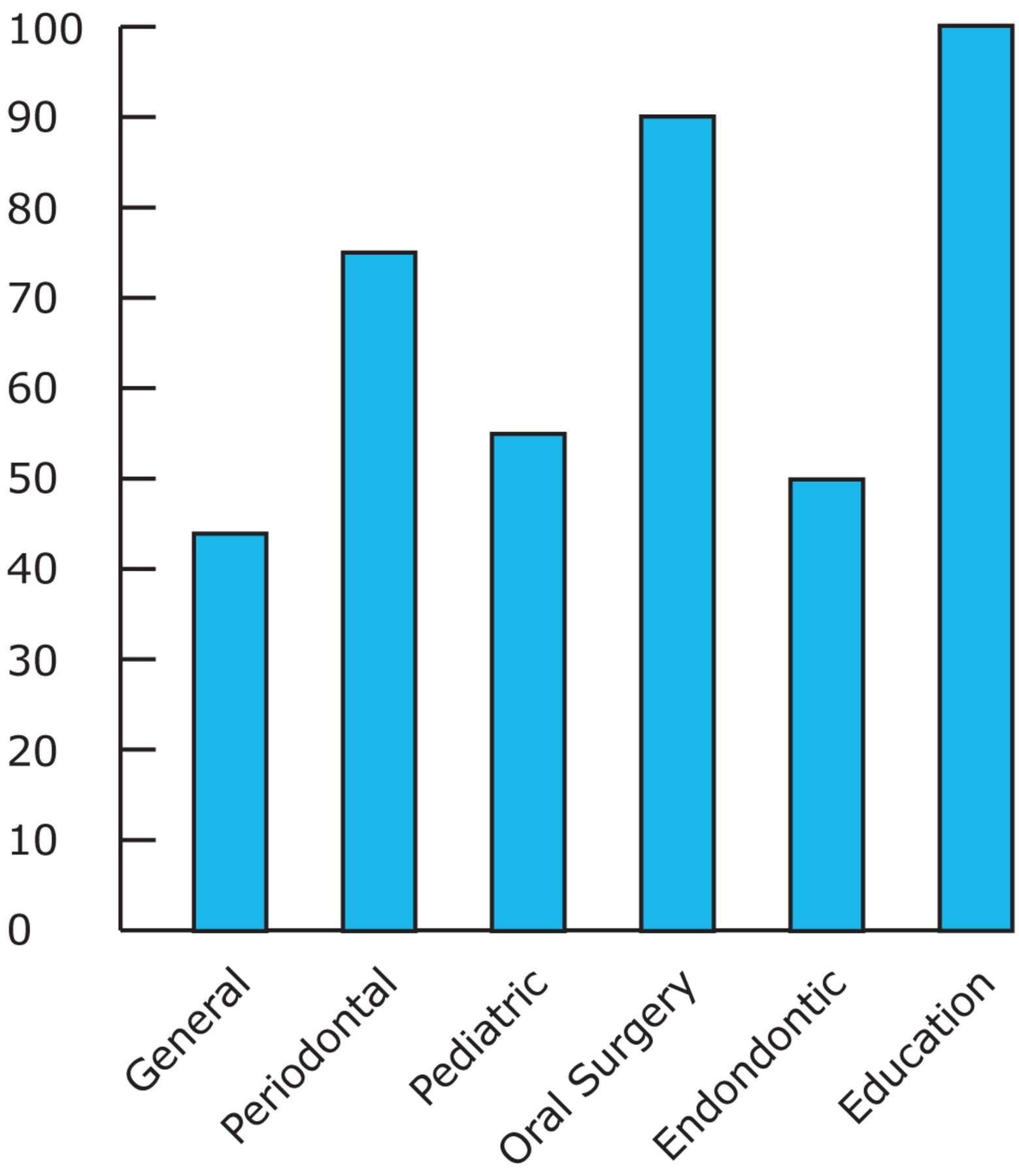
An ANOVA found that hygienists were more likely to be working part time than dentists. Hygienists were more likely to be unemployed or on temporary leave than dentists (F(3,785)=21.38, p=<0.01). Endodontic practices were most likely to call emergency personnel and pediatric practices were least likely (F(6,783)=4.06, p=<0.01). Oral surgery practices were most likely to administer nitroglycerin and pediatric practices were the least likely (F(6,783)=4.49, p=<0.01). Oral surgery practices followed by endodontic practices were most likely to have an unresponsive patient (F(6,779)=2.36, p=<0.05). Respondents participating in CPR outside the dental setting were most likely to be from the oral surgery practice setting, while respondents from the endodontic practice settings participated the least in CPR outside the dental setting (F(6,783)=7.03, p=<0.01). All educational settings surveyed indicated they had an AED available and most oral surgery settings had an AED available. General dentistry settings were least likely to have an AED available for use (F(6,759)=5.56, p=<0.01) as illustrated in Figure 2.
2011 Significant Pearson Correlations - Profession
Attitude questions using the Likert scale were summed to create a new variable for comparison across groups. These comparisons revealed that younger respondents had more positive attitudes regarding AEDs (F(5,785)=5.94, p=<0.01) as seen in Table VIII. However, this result may be influenced by the younger mean age of hygienists, who collectively indicated more positive attitudes. Those practicing in the oral surgery and educational practice settings had the most favorable attitudes regarding AEDs while endodontic practices had the least favorable attitudes (F(6,784)=2.44, p=<0.05).
Discussion
Results suggest that several changes have occurred since the 2004 study. AEDs appear to be becoming more prevalent in Ohio dental settings. The amount of AED training and CPR training also appears to be increasing. These changes may be due to increased awareness of the role of AEDs in BLS and the continued presence of AEDs in public locations.
Respondents were asked if they had administered nitroglycerine or performed CPR on a patient in the dental setting to ascertain the frequency of potential cardiac emergencies in the dental setting. While nitroglycerin use remained the same and CPR in the dental setting had decreased slightly, a 5% increase was noted in the number of professionals who called emergency personnel for a cardiac emergency. Also, practitioners with unresponsive patients and patients experiencing chest pains have increased since 2004. These results may suggest an increasing concern about potential cardiac emergencies in the dental setting. Due to expansions of the services offered by dental professionals, increases in dental professionals' roles outside the dental setting, and an expanding medically-compromised and geriatric patient base that has a heightened risk for SCA, the use of AEDs is becoming an increasingly-important subject for dental professionals.
Another factor is estimated response times for emergency care. Perceived response times were reported similarly in 2004 and 2011 at 3 to 5 minutes for an EMS response. However, health care provider perceptions may be optimistic regarding these response times. Previous studies have confirmed that EMS response times can vary greatly at remote and rural locations. Urban areas also suffer poor response times due to increased traffic and large buildings.5 In many cities, the survival rate is less than 5% due to response times.31
In addition to documenting the prevalence of AEDs and the incidence of cardiac emergencies in the dental setting in Ohio, this study explored the attitudes of dental professionals since use and acquisition of an AED may be restricted by attitude and perceptions. The additional attitude questions in the 2011 survey further demonstrated the differences in attitudes of dentists and dental hygienists. The more positive attitudes of dental hygienists may be explained by the increased exposure to AEDs through CPR training required for CPR certification and specific AED competency in the dental hygiene standards. However, the results suggest that the overall perceptions of both dentists and dental hygienists are becoming more positive regarding AEDs in the dental setting. Practice settings that most often had AEDs available also had the most positive attitudes regarding AEDs. This suggests that exposure to and training on AEDs may also influence attitudes.
As the new 2011 CPR guidelines reaffirm the place of an AED in the event of SCA, public awareness of the benefits of AEDs continues to increase with AED legislation diffusing into dentistry across the nation.32 Several states, although not Ohio, enacted some form of AED legislation in the dental setting since the original study, beginning the process of integrating AEDs into dentistry. While no reported cases regarding the negligence or liability of a physician or dental office for not having an AED on the premises were identified during this review, several well-known lawsuits have been brought against Busch-Gardens, Lufthansa and United Airlines for failure to have an AED.33 Given that health care providers, including dental professionals, are educated in emergency procedures and are aware of the benefits of AEDs, dental professionals could be held to a heightened standard of care regarding the access to emergency equipment to provide emergency care. A commentary by an attorney experienced in AED-related matters has speculated that similar legal action is imminent within the dental community.34
This study should be interpreted in light of several limitations. This study is subject to all limitations inherent with self-reported data, i.e. the validity and accuracy of this data must be questioned. Specifically, self-reports are potentially unreliable because participants may not always report their actual feelings and may respond as they feel they should instead of how they truly feel. The delimitation of this project is the sampling of dental professionals across Ohio; consequently, the size of the sample could also limit the extrapolation or generalization of the findings of this project to the whole dental population in Ohio. Unfortunately, the response rate was slightly lower than the previous study although the overall response was larger due to a larger sample size. Moreover, the only existing research on the use and attitudes of AEDs in the dental setting was obtained from the previous 2004 study. Little other data exists to provide contextual data. Further research on the use of AEDs in the dental setting and the attitudes of dental professionals who use them needs to be completed.

Practice Settings with AEDs
Age and Attitude
Conclusion
This study of Ohio dental professionals affirms the conclusion from the 2004 study that dental professionals, including students, should be familiar with the proper protocol to follow in the event of a cardiac emergency. As public awareness of their benefits increases, AEDs are becoming more common with installations at shopping centers, airports and office buildings. Having an AED on the premises, either in a dental office or dental educational setting, may soon be the standard of care for cardiac medical emergencies. As the standard of care evolves to include AEDs and legislation is passed, dental professionals should be familiar with and able to recognize and treat cardiac emergencies, including use of AEDs. Even if AEDs are not mandated, AEDs can be a critical item to have to save lives and dental settings should consider having one available.
Acknowledgments
This study was funded by the UMKC School of Dentistry Rinehart Foundation and the UMKC Women's Council Graduate Assistance Fund.
Footnotes
-
Jennifer A. Pieren, RDH, MS, is an adjunct faculty at the Dr. Madeleine Haggerty Dental Hygiene Program, Youngstown State University. Cynthia C. Gadbury-Amyot, MSDH, EdD, is an Associate Dean and professor at the University of Missouri-Kansas City School of Dentistry. Diane P. Kandray, RDH, MEd, is an associate professor at the Dr. Madeleine Haggerty Dental Hygiene Program, Youngstown State University. Christopher J. Van Ness, PhD, is a research assistant professor and Director of Assessment at the University of Missouri-Kansas City School of Dentistry. Tanya Villalpando Mitchell, RDH, MS, is an associate professor and the Director of Graduate Studies at the University of Missouri – Kansas City School of Dentistry, Division of Dental Hygiene.
-
This study supports the NDHRA priority area, Occupational Health and Safety: Investigate methods to decrease errors, risks and or hazards in health care and their harmful impact on patients.
- Copyright © 2013 The American Dental Hygienists’ Association





{kind=link}
{kind=link}