



Abstract
Purpose: Patients with HIV/AIDS deserve to be treated with compassion and receive comprehensive care by their dentist and dental hygienists. Previous studies have shown that many dental and dental hygiene students had negative attitudes towards treating such individuals. This article addresses the effectiveness of a program that trains dental hygiene students in the issues of treating this population. All pre–doctoral students at the Loma Linda University School of Dentistry are required to receive this training. Dental hygiene students complete a pre–session survey during their first year and a post–session survey as they complete the training during their second year. The survey questionnaire was administered during the period of 2003 to 2009, during which 197 students completed responses to the post–session survey. Five questions in the survey address self–evaluation of knowledge, attitudes, confidence in the efficacy of Universal Precautions and Post–Exposure Prophylaxis (PEP) following blood borne exposures. This study reports on 5 overlapping 2 year testing cycles and shows significant shifts in all 5 areas surveyed. The most significant gains were in “Familiarity with PEP” and “Confidence in the Efficacy of PEP.” These data support the usefulness of an HIV program in preparing future dental hygienists to deliver appropriate care to persons living with HIV/AIDS.
Introduction
HIV/AIDS first emerged as a recognized disease in 1981. No one could have predicted how this disease would evolve over the next 3 decades, the impact it would have worldwide and the enduring difficulties associated with preventing and treating it. The disease remains a great challenge to public health and human rights worldwide. In the heavily impacted developing countries, it is so devastating that it can impact the fabric of society and national security.1 Due to the advances and accessibility of anti–retroviral therapy, HIV/AIDS is no longer considered an immediate death sentence, and is now being viewed in the wealthier developed countries as a chronic illness.2 However, both a cure and effective vaccines remain elusive, and the successes of anti–retroviral therapy have also led to complacency, particularly among populations who are at risk of acquiring the disease.1 A pressing problem in the developed countries lies in the fact that, although people with HIV are living longer, the number of new infections has not been reduced.3
The estimated number of new cases per capita in the U.S., according to the Center for Disease Control and Prevention (CDC) 2005 to 2008 surveillance report, went from 37,000 to 42,000 based on better and more complete reporting of new HIV infections.3 The report further stated that this incidence rate has been roughly stable since the early 2000s.1 Studies have shown that about 19.3% of HIV infected medical patients in the U.S. have unmet dental needs that have not been treated in the previous 6 months.4 This number is much higher in states without dental benefits, where unmet dental needs may reach as high as 31.5%.4 The highest recorded unmet need of 43% occurs predominantly among lower income African American women.5 Formicola et al found that disparities exist in health care with respect to minority groups, and that bias and stereotypic beliefs held by providers may contribute to the disparities.6 Dental professionals provide a unique role that can help alleviate pain and infection, which may increase the quality of life and ultimately impact the course of the disease.4 This points out the need for knowledgeable and dedicated dental communities, who not only assist in early diagnosis, but also treat these HIV/AIDS patients in a compassionate, comprehensive manner to improve the lives of those who are living with the disease and ultimately help the reduction of new infections with early detection.
There is not a great deal of scientific literature regarding the effects of educational efforts on the attitudes and beliefs of dental and dental hygiene students with respect to treating HIV–positive patients. Previous studies in the field of dental education suggested that male dental students had significantly stronger negative attitudes towards patients at risk for HIV/AIDS than female students.7 The findings also pointed out a lack of knowledge which was significant due to the fact that it could “translate into a potential risk both for the patients and providers.”7 In this same study, the students suggested including case studies, discussion groups and possibly supervised clinical rotations to improve their curriculum. A more recent study demonstrated that dental students' knowledge of an HIV–seropositive status, and perceived responsibility of the patients for contracting HIV, could be predictive of negative attitudes towards the treatment of these patients.8 In this study, Seacat et al recommended interaction between dental care providers and persons living with HIV/AIDS (PLWHA) that intermingled the classroom and clinical experience, as a mandatory component in the dental curriculum.8 Other data also showed that negative attitudes and discrimination continues beyond the 4 year dental program and that dentists in postgraduate programs can also have a negative bias towards PLWHA and also toward homosexuals.9
In a study by Rohn et al that reviewed the social and psychological concerns that impede delivery of care to HIV–positive patients in the dental education arena, it was found that fear of status disclosure to health care workers among PLWHA was a significant barrier in access to care.10 Their findings suggested ways to improve students' attitudes to reduce prejudicial or discriminatory behaviors, which in turn might improve patient confidentiality. These recommendations included:
Inviting HIV–positive individuals to talk with students and to share their perspectives as patients
Have faculty model appropriate ways of interacting with patients and discussion confidential information
Provide role–playing opportunities for students as they start seeing patients in the clinic, so they have the chance to apply what is learned in the classroom
These, along with other recommendations, were made to prepare students to ultimately “enhance access to health care.”10
In a study involving dental students and their comfort level in treating vulnerable populations and future willingness to treat, only 47.4% expressed comfort in treating HIV/AIDS patients, while 17.1% expressed willingness to treat PLWHA in the future.11 Most of the students did not have any experience with seropositive patients, and only 22.7% had some experience. Generally, prior experience, such as community–based clinical experiences, had a positive impact on the comfort level of the students and, in some instances, translated into future willingness to treat vulnerable populations.12,13 Mulligan et al also recognized the importance of providing continuing dental education on HIV after graduation that covers oral pathology, medical issues, medications, psychological issues, legal and ethical implications, risk assessment and OSHA principals.14
There are a few studies that specifically address the concerns of dental hygienists or dental hygiene students with respect to HIV/AIDS. King et al mailed a survey to practicing dental hygienists in the U.S. and received 856 responses.15 A majority of respondents (53.9%) felt that treating patients with HIV/AIDS increased their personal risk, and 63.5% reported always using extra precautions with known HIV/AIDS patients. A total of 38% believed that double–gloving was appropriate when treating this population and 25.4% indicated that different sterilization and disinfection methods were necessary. The authors concluded that the attitudes and practices reported by many of the respondents suggest a lack of understanding of the concepts of infection control and standard precautions. They also recommended that dental hygiene students should have multiple experiences providing treatment for persons with infectious diseases such as HIV/AIDS.15
Cohen et al conducted a one–time survey of dental hygiene students to determine student attitudes toward persons with 2 different diseases (AIDS and leukemia) and sexual preferences (heterosexual and homosexual).16 The survey indicated no bias toward homosexuals but found there was bias towards persons with AIDS. Giulani et al surveyed practicing dental hygienists in Italy and found that 5.9% of respondents indicated they had denied treatment based on patients' HIV status, and 80% of these respondents did so due to fear of getting the disease themselves.17 Those who refused treatment reported a lower use of personal protective equipment, particularly eyewear, than those who did not deny treatment. These authors cited an older survey of dental health care workers from the pre–anti–retroviral therapy era, which found that willingness to treat HIV–infected persons was proportional to the individuals' practice of more thorough infection control procedures.18
Dental Partnership Grant under the Ryan White Program
The Health Resources and Services Administration (HRSA) acknowledged the need for improved training of dental and dental hygiene students in the care of individuals with HIV. In 2002, HRSA announced a grant opportunity for funds under Part F of the Ryan White CARE Act. This grant established the Community–Based Dental Partnership Program in which dental education institutions were chosen to partner with community–based dental providers to train students in community clinical settings where dental care is provided to an HIV–positive clientele.13 The Loma Linda University School of Dentistry partnered in the program with the Social Action Community Health System (SACHS) that operates a low–cost community dental clinic in nearby San Bernardino and has a large HIV–positive clientele. The Program and Application Guidance document for the grant indicated that grantees would have to “develop innovative curriculum design, quality improvement programs and program assessment methods.”19
Development of the Loma Linda University School of Dentistry Program
The original faculty of the HIV and the Dentist program at Loma Linda University School of Dentistry reviewed the existing curriculum content of those pre–doctoral courses that addressed HIV disease to better understand what was actually being taught elsewhere in the predoctoral dental and dental hygiene programs. The intent was to build on what was already being taught and to minimize presentation of redundant material. The faculty also attended the continuing education program of the Pacific AIDS Education Training Center at the University of Southern California (USC) School of Dentistry. In reviewing the literature for this course, it was noted that participation in the USC program resulted in significantly changed HIV–related knowledge, attitudes and beliefs among course participants, as well as enhanced commitment to infection control and screening for risk behaviors and presence of HIV infection.20 During this course, the Loma Linda University School of Dentistry faculty were able to interact with HIV–positive patients in a clinical setting, along with observing a role–playing experience that demonstrated possible ways of interacting with such patients.
In the Loma Linda program, there was an extensive effort to develop an innovative curriculum that involved faculty, dentists and staff at SACHS, and the community advisory group that was formed to give input on the program. Loma Linda University established this program as a required rotation for all predoctoral students during their senior year. Completion is a requirement for graduation. The program is conducted entirely at the SACHS clinic and has both clinical and didactic components. The didactic component includes lectures, discussion of cases, interaction with staff dentists, interviews with patients, role playing to illustrate possible responses to various clinical situations and viewing a video that was produced specifically for this program. The clinical component involves students providing dental care to the HIV–positive clientele under the supervision of faculty. During program development, it was decided to train the students in small groups (5 to 7 students) over 2 half–day periods. The students in each group spent a total of 8 hours during 1 week periods in the HIV training program at the community clinic so that every student could have direct interaction with HIV–positive patients. With this scheduling, it requires most of the academic year to train all of the dental and dental hygiene students each year. The curriculum for the HIV and the Dentist program is presented in Table I.
In the development of the HIV and the Dentist curriculum, the authors took advantage of the close proximity of the School of Dentistry and the SACHS clinic (3 miles). This allowed students to attend a 4 hour session in the morning at SACHS and still be able to attend the 4 hour afternoon session at Loma Linda University on the same day. The brevity of each student's training experience (8 hours) and the inability to predict the patient–care experiences that would be available each week contributed to the decision to consider the patient–care component as service learning. The authors also decided to assess program outcomes by means of pre–session and post–session surveys to determine if attitudinal shifts and self–reported gains in knowledge were occurring with respect to treating HIV–positive individuals. Rubin stated that there is evidence that service learning experiences help “develop cultural literacy, improve citizenship, enhance personal growth and foster a concern for social problems.”21
The aim of this program is to help students at the Loma Linda University School of Dentistry manage the oral health care needs of persons with HIV infection. The purpose of this article is to discuss the impact the training program had on these students regarding the issues related to treating patients with HIV/AIDS. This discussion presents the results of pre– and post–session surveys of dental hygiene students administered over a 6 year period. These surveys focused on attitudes towards the HIV–positive clientele, comfort with treating this group, confidence in the effectiveness of Universal Precautions and Post–Exposure Prophylaxis (PEP) following blood–borne exposures, and self–assessment of understanding the issues involved.
HIV and the Dentist Curriculum at the Loma Linda University School of Dentistry
Methods and Materials
Assessment of program effectiveness has been measured since the program's inception by means of pre– and post–session surveys of the student participants. The survey questions were developed with the assistance of staff from the Behavioral Health program at SACHS. The pre–session survey is completed by dental hygiene students during the spring quarter of their first year in the Medically Compromised Patients course. The post–session survey is completed by the same students at the end of their second and final session each week as they complete their rotations during the second year. The surveys contained 5 statements regarding HIV general knowledge, attitudes towards the HIV–positive clientele, comfort with treating this group, confidence in the effectiveness of Universal Precautions and PEP following blood borne exposures, and self–assessment of understanding of the issues involved.
Analysis occurred with 6 years of pre– and post–session survey results (composed of 5 overlapping 2 year cycles). During 2003 to 2009, the surveys were distributed to 197 dental hygiene students, with 172 (87.31%) completing the post–session survey. Slight modifications were made to the surveys during the 6 year period, but general content remained the same. For example, at the end of the survey there was a place for student comments. The most frequent comment made was that students wanted to have more time with patients. The next most frequent comment was that there was some overlap of information from previous courses. A few changes were made in the course as a response to those comments cited above to eliminate unplanned redundancies. There was also a small reduction of didactic material presented to allow for more clinical time during the second day of the rotation. The range of student responses did not change substantially from year to year during the 6 year period of the study.
Statistical Analysis
Statements used in the surveys and the student responses during the study period are summarized in Table II. All statistical analysis was done using SAS 9.2. Those dental hygiene students who did not complete post–training questionnaires were excluded from the analysis. Descriptive statistics were generated, including means. The normality distributions were examined using histograms and Kolmogorov–Smirnov normality tests. Given the nature of the data, the non–parametric Wilcoxon Signed–Rank Test was performed between data recorded in pre–session and post–session surveys. A p–value of <0.05 was considered statistically significant. The data was compared on a 6–point Likert Scale ranging from “none” to “high” in all 5 areas surveyed as displayed in the header of Table II. The overall change in means was compared to generate the final result.
Percentages of dental hygiene student responses to the statements about general knowledge and treatment of HIV patients
Results
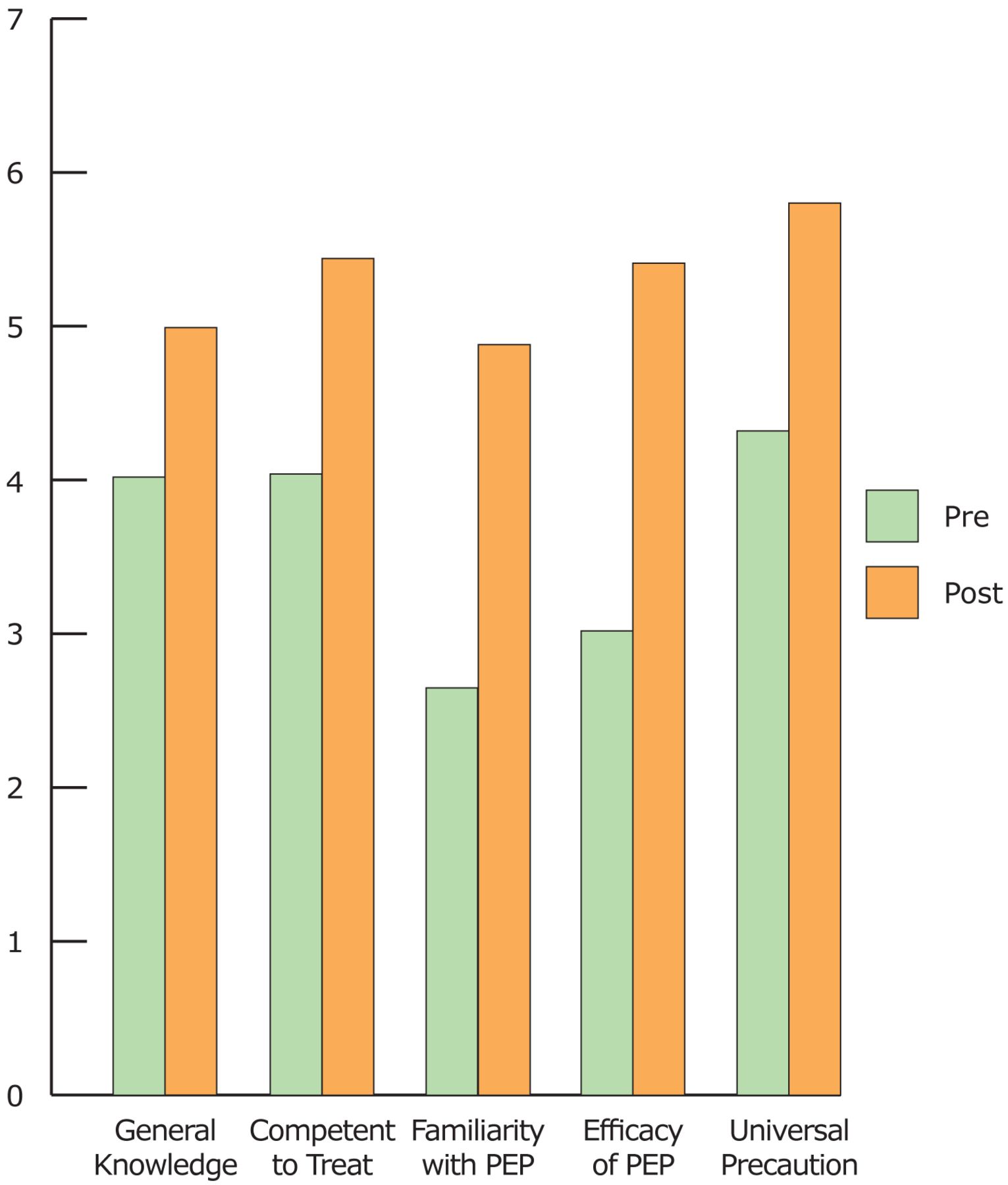
The Wilcoxon Signed–Rank Test revealed positive changes in all the categories that were highly statistically significant at a p–value of 0.0001 (Table II). The categories included “general knowledge about HIV infection” where there was a 24.1% change in the positive direction (pre–session mean equaled 4.02, and post–session mean equaled 4.99). The category “feeling competent in treating HIV positive patients” had a change of 34.7% (4.04, 5.44). The category of “familiarity with PEP” had a change of 84.5% (2.65, 4.88). The category of “confidence in the efficacy of PEP after an exposure to a contaminated dental instrument” had a change of 79.1% (3.02, 5.41). The final category addressed the “level of comfort with effectiveness of Universal Precautions in the dental office with reference to HIV infection,” and had a positive change of 34.3% (4.32, 5.80). The overall change in all the areas about the knowledge and treatment of HIV patients was in a positive direction, with the most convincing results seen in the area of familiarity with PEP and confidence about the efficacy of PEP following a blood borne exposure. A graphic presentation of a comparison of the means of the pre– and post–session responses to the 5 survey items is presented in Figure 1.
Discussion
A goal of the HIV and the dentist program was to improve the students' knowledge, attitudes and beliefs regarding the provision of dental treatment to PLWHA. Significant changes were observed in all 5 areas surveyed as reported in Table II. The observed changes are taken as evidence that student competence in dealing with HIV–positive patients has been improved by this program. It is also evident from Figure 1 that the differences in the pre– and post–session responses were substantially different in the 2 responses involving PEP as compared to the other 3 areas. The most likely reason for this is that the 3 items with the least pre– and post–session change are those areas to which the students had more substantial curricular exposure prior to the HIV and the Dentist training experience. Due to the fact that the second year dental hygiene students have already been introduced to HIV–related topics in the school curriculum, we expected the students to already have some HIV knowledge, resulting in less of a measurable difference in the post–test data regarding general knowledge of HIV infection. This was also the case for feeling competent to treat HIV–positive patients and belief in the efficacy of Universal Precautions. The other 2 items, which addressed familiarity with PEP and confidence in the efficacy of PEP, had been minimally addressed elsewhere in the curriculum, and these were the areas where the greatest changes were observed in the positive direction. All areas surveyed had a significant p–value of <0.0001.
One of the predictable findings of this program has been that, after completion of the externship, an increased number of students felt competent treating an HIV–seropositive patient. The data in Table II show that 60.1% of the first year dental hygiene students already expressed a feeling of competence to treat HIV–positive patients in the pre–session surveys. The expression of competence to treat rose to 98.9% in the post–session surveys. Part of this increase in confidence may be attributable to the additional clinical experience of the second year students (as compared to their first year status when completing the pre–session survey). The remainder of the increase is most likely attributable to the HIV training program. One of the unique features of this program that may have increased confidence has been the personal interview of an HIV positive patient by the students. This degree of personal interaction may have been the major factor in the most frequently observed comment in the post–session surveys in which students requested more patient contact time.
The most significant change was in the area of PEP. The “Familiarity with PEP” protocol had the greatest statistical change in the desired direction at 84.5%. Confidence in the efficacy of PEP after a blood–borne exposure had the second highest positive change at 79.1%. A likely explanation for these findings is that the HIV and the Dentist rotation is the only place in the dental hygiene curriculum where PEP is described in detail. Students show a high level of interest in strategies to protect themselves from acquiring an infectious disease like HIV due to occupational exposure. In addition, magnitude of the change may also be related to the fact that PEP was the last topic reviewed prior to the treatment of the patients during the second training session. Students were always encouraged to ask questions or make comments, and PEP has been one of the subjects where there has been high student participation in the form of questions and comments.

The Means of Pre– and Post–Session Responses to the 5 Survey Items
A less predictable finding was in reference to the increased confidence of Universal Precautions in relation to preventing transmission of HIV, with a 34.3% change in the response mean. There was a brief review of Universal Precautions since the students had already been exposed to the subject multiple times in the Loma Linda University School of Dentistry curriculum, yet there was still a highly significant change in a positive direction in this survey item. The categories of “Effectiveness of Universal Precautions,” “General Knowledge of HIV Infection” and “Feel Competent about Treating an HIV Positive Patient” had the most significant shift in the 2 lowest categories (None and Insufficient) from the pre– to the post–session surveys. All students expressed at least a marginal comfort level in these 3 areas after the externship. A possible future study could be to survey those students that participated in the training program after graduation, to determine if the positive outcomes observed in the study translated into an increased willingness to treat HIV patients. Additional questions in such a study could include reflecting on the importance of this rotation in their pre–doctoral training and whether it inspired them to continue to learn about treatment issues regarding people with HIV disease and other medically compromising illnesses.
Future modifications to the HIV and the dentist program could include training dental and dental hygiene students to conduct rapid HIV testing in the dental setting. An estimated 1.1 million persons in the U.S. are living with HIV/AIDS, and an estimated 24 to 27% of these people are undiagnosed and/or unaware of their HIV–positive status.22 Patients who become aware of their HIV diagnosis are more likely to reduce high risk behavior.23 It is estimated that approximately 25% of HIV–positive patients are responsible for 55% of the new cases, and most of these individuals are in the unaware category.23 Dental professionals are an untapped resource to access patients for HIV testing. Knowledge of a positive sero–status can help with early access to treatment, along with ultimately reducing further transmission.24 A study was conducted in a dental clinic to see how patients would respond to oral HIV testing in the dental setting. In that study, 73% of patients were willing to undergo HIV testing, and 37% actually preferred their dentist above any other provider.25 The CDC launched the Advancing HIV Prevention initiative in 2003, which allows testing to be conducted in a variety of settings, aimed at increasing the early diagnosis of HIV positive people.26 A separate study also determined that one–third of dental educators would consider offering rapid oral HIV testing in their clinics.27
Conclusion
The pre– and post–session survey data gathered over a 6 year period demonstrated that the program was successful in fulfilling the original goals of HRSA to impart a social context for health care and a greater understanding of the health needs of the HIV–positive population. The most significant changes in student knowledge were in the areas of PEP, followed by “Familiarity with PEP” protocol. Future studies may investigate teaching dental hygienists and dental students to conduct rapid HIV testing the dental setting.
Footnotes
-
Periza Zaninovic, DDS, is employed at the Mendocino Community Health Clinic, Ukiah, California. Zuhair S. Natto, BDS, MBA, MPH, DrPH (candidate), is currently a resident in the graduate program in Periodontics at Tufts University, Boston, Massachusetts, and is also a Lecturer in Community Dentistry, School of Dentistry, King Abdulaziz University, Saudi Arabia. Rodney Turner, DDS, is employed as a community dentist at the SAC Health System in San Bernardino, California. Gerardo Toledo, DDS, MA, is employed at Gerardo Toledo DDS – practice limited to Endodontics, Redlands, California. Graciela Duran, RDH, is employed at the Loma Linda University School of Dentistry. James Trott, DDS, MPH, MS, is employed at the Loma Linda University School of Dentistry. Thomas Rogers, DDS, MPH, MA, is employed at the Loma Linda University School of Dentistry.
-
This study supports the NDHRA priority area,
XXX:
XXX.
-
Disclosure
This project was supported by a Community–Based Dental Partnership Grant issued under Part F of the Ryan White Program by the Federal Health Resources and Services Agency (HRSA) HIV/AIDS Bureau, Grant number H65HA00004.
- Copyright © 2013 The American Dental Hygienists’ Association





{kind=link}