



Abstract
Purpose: A total of 40 states to date have expanded the role of dental hygienists with the goal of improving access to basic oral health services for underserved populations. In Kansas, legislative changes have resulted in the Extended Care Permit (ECP) designation. The purpose of this study is to describe the experiences of registered dental hygienists in Kansas holding ECP certificates (ECP RDH) as of July of 2014.
Methods: Secondary data analysis was performed utilizing data collected from a survey conducted in 2014 by Oral Health Kansas. All registered ECP RDH's were sent the 32-item survey via Survey Monkey®. Descriptive statistical analyses consisted of frequency distributions, and measures of central tendency. Inferential analyses using t-tests and ANOVA were conducted to compare groups.
Results: A total of 73 responses were received from the (n= 176) surveys that were e-mailed for a 41% response rate. Of the clinicians who responded, 80%, worked at least part-time and in school settings. The most consistent barriers to providing care were the inability to directly bill insurance (52%), financial sustainability (42%) and physical requirements (42%). Follow-up tests found significant differencs between clinician groups when examining barriers.
Conclusion: Although the ECP legislation appears to be expanding access to care for citizens in Kansas, significant barriers still exist in making this a viable model for oral healthcare delivery.
Introduction
Former Surgeon General Richard H. Carmona released “A National Call to Action to Promote Oral Health” in 2003.1 This Call to Action was designed to further the May 2000 report “Oral Health in America: A Report of the Surgeon General”.2 Call to Action had three major goals: promote oral health, improve quality of life, and eliminate oral health disparities. As of 2016, dental providers, healthcare workers and legislators across the United States continue to work toward accomplishing these goals.
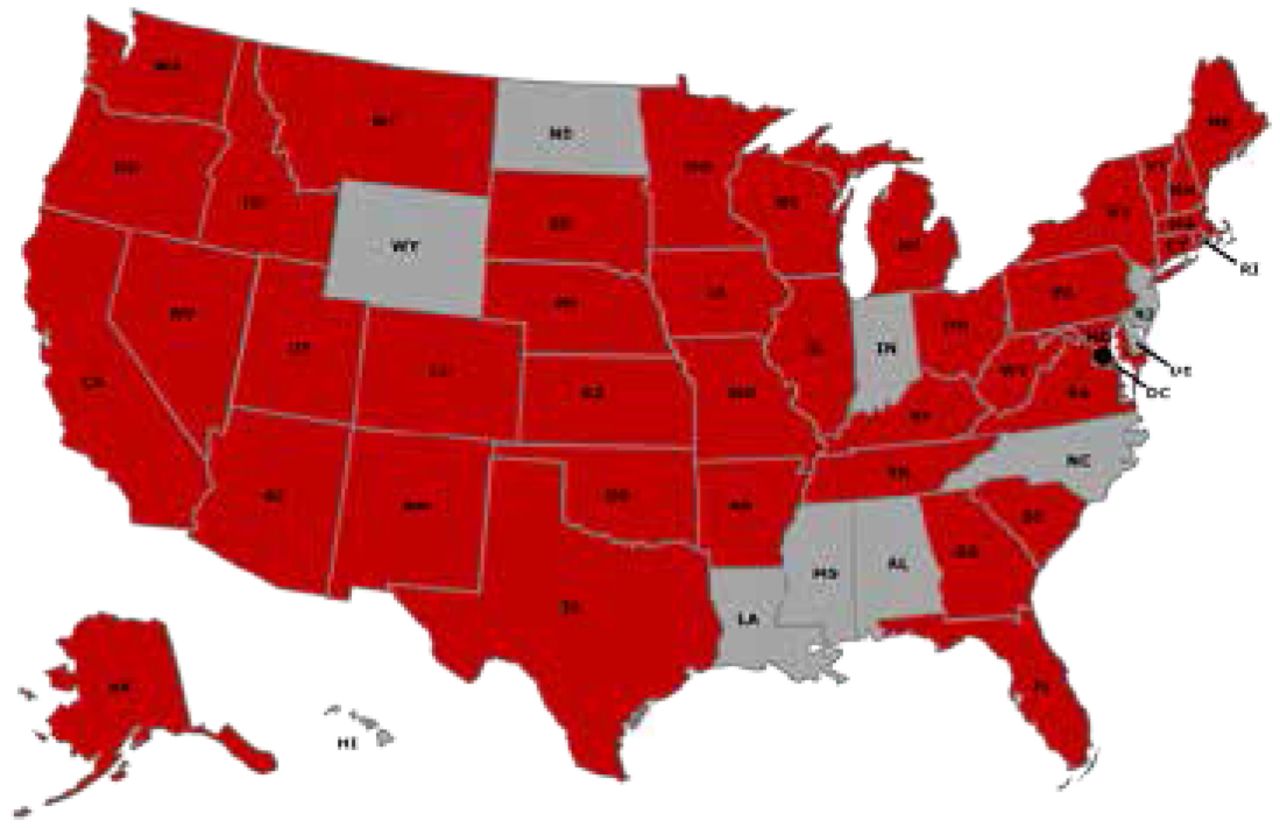
Healthy People 2020 highlights that individuals with less access to preventive dental services have greater rates of oral diseases.3 Individuals without the means, or employer-subsidized benefits, often find themselves in a position of severely limited options for affordable oral care. Direct access to oral care from dental hygienists is one method to combat this problem. Currently, 40 states, including Kansas, have legislated variations on direct access for the practice of dental hygiene. Figure 1.4-5

Direct Access State Map, American Dental Hygienists' Association5
*Red areas denote direct access states
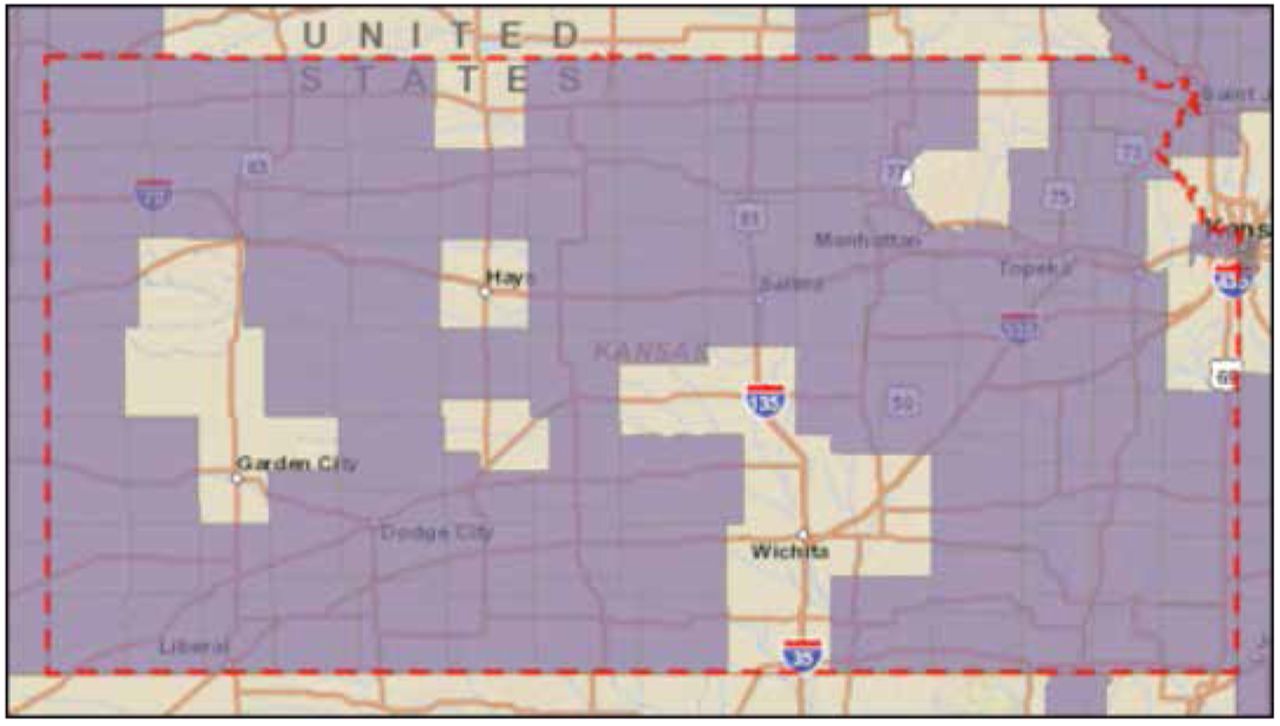
A 2015 report of the U.S. Department of Health and Human Services (USDHHS) outlining the national and state-level predictions for dentists and dental hygienists noted that all 50 states, in addition to the District of Columbia, are expected to experience a shortfall of dentists; while the number of dental hygienists is expected to outpace the number of patients in need of hygiene services.6 Dentist shortfall areas as of March 2016 in the state of Kansas are shown in Figure 2.7 The USDHHS report suggested considering the use of dental hygienists, an existing member of the dental team, to minimize the impact of anticipated dentist shortages.6

Dental Healthcare Provider Shortfall Areas in Kansas7
Dental Practice Models Impact on Access to Oral Healthcare
It has been argued that the structure of a typical dental office contributes to reduced access to care.8-10 Kitchener and Mertz describe the typical model of practice to be a clinic or dental office where dentists and their team members provide a full range of services to patients presenting for care on an autonomous basis. In addressing the issues of access to care for the underserved and unserved, one successful practice model is the safety net clinic, which provides access for all segments of the population regardless of their socioeconomic status.11 Safety net settings can be defined as public clinics, hospitals and community health clinics.12 Federally Qualified Healthcare Centers or FQHCs are a common type of safety net setting.
Alternative practice settings for dental hygienists have also been utilized to expand access to care. In 2012, a case study was conducted in the state of California to examine the experiences of registered dental hygienists practicing in alternative practice (RDHAP).9 California RDHAPs were found to practice primarily in non-fixed settings such as community facilities, residential assisted living facilities, private residences and school-based settings.9 A subsequent study examining the development of the RDHAP in California concluded that while RDHAP providers serve populations with high levels of need, extreme difficulties in accessing those populations via both traditional and alternative practice models still exist.10 Key among the findings were difficulties with payer acknowledgement on the part of Medicare and insurers and Medicaid requirements that continuied to exacerbate access to care barriers.
Alternative Practice Roles in Dental Hygiene
State-specific legislation has created a wide range of roles for dental hygienists to pursue, as well as a variety of specific education and licensure requirements, in order to increase access to care for all individuals. From 2008 to 2014 there was a 32% increase in the number of states adding legislation to expand the dental hygiene scope of practice as a means of improving access to care.13 Examples of states expanding of the scope of practice include Colorado where dental hygienists are permitted to practice independently as well as own and operate their own practice without any additional licensure requirements and Oregon where the Expanded Practice Permit Dental Hygienist (EPPDH) model allows dental hygienists to provide care to limited access populations without the supervision of a dentist.14, 15
Many other states have come up with unique solutions when it comes to alternative practice models for dental hygienists. Notable among these is the mid-level provider role for dental hygienists with legislation that has passed in Minnesota, Maine and Vermont establishing dental hygiene based, oral care provider models. To date, much summary research has highlighted not only the disparity of access to care issues but also the significant variations scope of practice legislation for dental hygienists.16
Kansas Extended Care Permit Program
Specific to Kansas, the so-called “Dental Hub” program evaluations from 2007 – 2011 demonstrated increases in access to care on both geographic and socioeconomic levels through the utilization of a centrally located safety net “hub” clinic offering full-service dental care and combined with remote public health facilities, or “spokes”, for preventive and screening level care.17 Individuals living in remote areas or having limited financial resources were able to receive care through this model. Participants noted the program became significantly more sustainable with the creation of the Kansas Extended Care Permit (ECP) program, as the “spoke” clinics were primarily staffed and run by Kansas ECP dental hygienists.
Development and legislation of the Kansas ECP role for dental hygienists has been a key component to the state's approach to addressing the disparities in access to care. Currently Kansas has three levels of the Extended Care Permit program; Extended Care Permit I (ECP I), Extended Care Permit II (ECP II), and Extended Care Permit III (ECP III).18 (Table I)
Preliminary studies of the Kansas ECP dental hygienist, completed in 2010, demonstrated that this legislation enabled providers to reach previously unserved or underserved populations.19 Qualitative analysis resulted in the emergence of an “entrepreneurial spirit” theme associated with ECP providers willing to work outside of the traditional practice model, learn new skills required to provide ECP services, and tackle a variety of barriers in order to increase access to oral healthcare services.19
Brotzman-Myers et al. conducted a follow up quantitative study in 2012 to examine the perceptions of all registered ECP dental hygienists in the state of Kansas.20 A majority of the respondents (92%) believed that the ECP provides greater access to oral healthcare. ECP providers reported utilizing their permits in a variety of settings including schools, Head Start centers, safety net facilities, and nursing homes. Barriers faced by providers in fully utilizing their ECP permits included difficulties with facility administrators (39%), obtaining start up financing (22%), limited workspace access (14%), and finding a sponsoring dentist (12%). Of the 60 ECP respondents completing the survey, ECPs were shown to be providing oral healthcare services in 58 out of 105 counties in Kansas, with a significant number designated as health professional shortage areas.20
ECP I, II & III Descriptions
A 2015 study of the Kansas school-based oral health program, Miles of Smiles (MOS), utilizing care provided by an ECP hygienist provider in partnership with the University of Missouri Kansas City (UMKC) School of Dentistry, demonstrated that children who had contact with the ECP hygienist had significantly reduced rates of decay, increased provision of restorative treatment and a decreased urgency for dental restorative needs.21
While the Kansas extended care permit dental hygienist does not parallel health provider models such as advanced practice nurses requiring a masters and doctorate level education, it does provide an intermediate step for expanding access to care. It is instructive to know that legislation for a mid-level provider has been introduced every year since 2011 in Kansas with continued opposition from organized dentistry. Similar to other health professions, the proposed Kansas mid-level legislation calls for dental hygienists to complete graduate level education as one of the requirements for mid-level provider status .
As Kansas continues to pursue alternative methods to improve access to care, ongoing research must be done to evaluate how the existing ECP workforce model impacts access to oral healthcare. To that end, Kansas's oral health coalition, Oral Health Kansas (OHK), developed a survey for Kansas ECP hygienists to gain insight into the ECP program. Data were collected in the summer of 2014 to determine the impact of all ECP dental hygienists (Levels I, II and III) in increasing access to oral healthcare services in the state. The purpose of this study is to describe the experiences of registered dental hygienists in Kansas holding ECP certificates (ECP RDH) as of July of 2014.
Methods and Materials
Secondary data analysis was performed utilizing data collected from a survey conducted in 2014 by Oral Health Kansas upon receipt of approval from the University of Missouri-Kansas City, Institutional Review Board (#15-332) .
Subjects
The target population for this study consisted of all dental hygienists in Kansas holding an Extended Care Permit at the time of the survey administration (n=176). The electronic survey was launched on June 16, 2014 and closed on July 5, 2014. A total of 176 surveys were e-mailed and a response rate of 41% (n=73) was obtained. Demographics of the study participants are found in Table II.
Demographics of ECP Provider Respondents
Survey Instrument
The 32-item survey developed by Oral Health Kansas (OHK) was delivered via an online format using Survey Monkey®. The survey employed a combination of response formats from a menu of Likert scales, multiple allowable answers, and open-ended written comments. Questions pertained to demographics and employment statistics, motivation for attaining and using an extended care permit, and barriers to practice. Content validity was ensured through experts employed by OHK with knowledge and involvement in the Kansas ECP dating back to the initial legislative process in 2003.
Statistical Analysis
Quantitative data analysis was performed. Descriptive data analyses consisted of frequency distributions and percentages. Inferential data analysis consisted of the conduct of independent-samples t tests and analysis of variance (ANOVA) to examine group differences.
Results
The majority of the OHK survey respondents reported obtaining an associate degree in dental hygiene between 2000-2009. Thirty-seven percent reported being in practice 3-10 years, and twenty-nine percent 11-20 years. Ninety-three percent reported being currently employed and the majority of ECP dental hygiene respondents (85%) reported maintaining a current ECP status. (Table II)
The survey also examined how many days per week respondents worked in specific settings. The largest number of respondents reporting full-time work (n=12), 5 days/week, were found to be working in an FQHC setting. The second largest practice setting is the traditional privately owned solo/group practice setting (Table III).
For this study, only half (n=37) of the respondents reported actively providing ECP services, and of those, 69% provide ECP services on a limited, part-time basis. Community settings with the greatest number of ECP dental hygienists currently providing care are school-based programs (n=58), followed by skilled nursing centers (n=14), and senior-focused housing and health departments (n=24). Senior–focused housing has experienced the greatest increase over time in the use of the ECP dental hygienist. While hospital settings and Indian reservations were also included in the survey, none of the respondents reported providing services in either of these settings (Table IV).
Besides workplace settings, the ECP clinicians were asked to report on the specific populations currently or previously receiving ECP services. Currently, the respondents provide the greatest concentration of ECP services to school aged children with the greatest increase over time occurring in populations of children with special needs and services to elders (Table V).
The ECP clinicians were asked to identify barriers to rendering ECP care to patients. Fifty-two percent of respondents identified the inability to direct bill private insurance as an ongoing barrier to providing ECP services. Specifically, the inability to directly bill Medicaid was identified as a barrier by 41% of respondents. Roughly half of respondents, 47%, identified consent for care as a current barrier. Similar response rates were noted for financial viability (44%), physical requirements (42%), and inadequate patient numbers (38%). However, more than half of the respondents believed these issues were no longer a barrier to care. (Table VI).
An independent-samples t-test comparing perceived total barriers (dependent variable) between ECP hygienists working in private practice and FQHC practice settings (grouping variable) found a significant difference between the means of the two groups (t(47) = 2.287, p<.05). Dental hygienists in FQHC settings perceived fewer barriers (m=2.05, sd=2.4) than dental hygienists in private practice settings (m=4.04, sd=3.46). An independent-samples t-test was conducted to compare perceived total barriers (dependent variable) between ECP hygienists who reported interest in applying for the next level of ECP and those with no interest in applying for the next level of ECP (grouping variable). There were no significant differences between groups [t(59) = .866, p>.05]. Dental hygienists planning to apply for the next level ECP reported greater perceived barriers (m=4.71, sd=3.29) than those not planning to apply (m=3.83, sd=3.37). These results show that the perception of barriers to providing ECP care did not impact the decision to pursue the next level of ECP.
Employed/Number of Days Per Week x Workplace Setting
Reported Community Settings
A one-way analysis of variance was conducted to evaluate the relationship between years in clinical practice (3-10 years, 11-20 years, 21-30 years, ≥31 years) and perceived total barriers encountered by the ECP dental hygienist. A significant difference was found [F(3,69)= 5.99, p<.05]. Post hoc comparisons using the Scheffe's method indicated that the mean score for the clinicians practicing 3-10 years (m=1.96, sd=2.38) was significantly different than that of the clinicians practicing 21-30 years (m=2.50, sd=3.82). This confirmed the impression that clinicians reporting 31+ years of practice perceived greater barriers in the provision of ECP services.
Discussion
The purpose of this research was to describe the experiences of dental hygienists holding an Extended Care Permit in the state of Kansas by performing secondary analysis of the results of an OHK survey administered in the summer of 2014. ECP I legislation was passed in 2003 and data show a steady increase of dental hygienists seeking an ECP I from 2003 to 2014. ECP II legislation, designed to expand the scope of populations served, was passed in 2007 with the number awarded each year remaining relatively stable from 2007-2014. Conversely, ECP III legislation was passed in 2012 to include minimal restorative dentistry procedures such as decay removal using hand instrumentation and placing of a temporary restoration, however there was a sharp decline in in the number of dental hygienists seeking an ECP III from year one to year two (Table II). It is important to note that the various permits, ECP I, II and III, are not contingent on a progressive order. The legislation enacted in Kansas does not require the dental hygienist to obtain an ECP I, prior to being eligible to apply for the ECP II, or ECP III.
Results from this study show that the vast majority of the survey respondents (93%) are currently employed and the workplace setting where the ECP is most often working a five day week (full-time) is in the FQHC setting. The community setting receiving the highest percentage of ECP services during the period of data collection in 2014, were schools and Head Start settings. These findings contrast with previous research highlighting the entrepreneurial interests of ECP clinicians, who reported working independently in community settings beyond schools, such as senior-focused housing.19 When considering the labor, delay in reimbursement, and added expenses related to billing through a partner dentist (Table VI) these factors may contribute to the study findings showing that ECP dental hygienists are working more frequently in FQHC practice settings versus more autonomous practice settings. It is possible, given the physical demands, reporting requirements, and various billing challenges, that ECP RDHs turn more often to FQHCs or other safety net settings as places of employment to meet their personal needs. Because the legislation in Kansas does not currently support direct billing by the ECP RDH, costs associated with the delivery of ECP services could easily become overwhelming to ECP RDHs attempting to practice independently. In addition, the burden of self-reliant transportation of persons and equipment to a variety of locations, associated with a mobile dental hygiene practice, can be excessive. The long-term financial sustainability of a solo hygiene practice utilizing an ECP RDH in partnership with a dentist may also be an issue, which is consistent with Siruta's findings from 2013.22
Populations Previously and Currently Receiving ECP Services
Respondents' Beliefs About Barriers to Care
A previous example of a successful program reliant on external support is the Miles of Smiles (MOS) program. MOS worked in partnership with the University of Missouri-Kansas City (UMKC) School of Dentistry which contributed substantial supportive resources and infastructure. Possible reasons why ECP providers rely on safety-net settings, such as FQHC's, may be income stability and the ease of compensation for services provided. Further research is needed in this area to identify and strategize how to negate potential barriers.
Growth in care provided to both young and older adults was revealed although the greatest net growth was identified in senior-focused housing populations. This may correspond with the establishment of the ECP II and III which allowed for increases in age ranges, clinical settings and complexity of care. However, the data still revealed that these groups received care in significantly lower percentages than youth populations. This provides another area of future research to examine the progression of these trends.
Survey respondents reported a wide range of years in clinical practice. Clinicians earlier in their careers, 3-10 years, perceived significantly fewer barriers than those practicing 21-30 years. More research is needed to further investigate the relationship between perceived barriers and years of practice. Among theories to explore, include whether educational programs may be providing newer graduates with improved arwareness and preparation to work in alternative practice settings or utilizing expanded scopes of practice.
The significant decrease in the numbers of ECP III permits issued during the first and second years of its availability should be further investigated. Possible causes could include greater acclimation to independent practice settings and the associated perceptions of barriers to providing ECP care in independent or alternative settings. The present study did not find a significant relationship between the ECP RDH's desire to apply for the next level of ECP permit and perceived barriers to care. Future long-term studies should follow how the ECP III is being used to address access to oral healthcare.
Limitations of this study have been identified. The ECP program is specific to Kansas and describing the Kansas ECP experiences may not have direct implications on clinicians in other states with different practice legislation. However, the results of this study may be useful when evaluating outcomes of changes in scope of practice legislation, particularly in Kansas. Other limitiations include the lack of participation in the development and delivery of the original survey, and the inherent nature of self-reported data to bias.
Conclusion
The results of this research suggest that souces of improved access to care include a variety of FQHC's, other safety net settings, senior-focused housing, and private practices utilizing ECP dental hygienists. Even though the ECP model is not available in all states, the use of similar training and practice models can not only be effective, as in Kansas, but in other states with similar access to care issues and provider shortages. One of the greatest barriers to improved access to care is still the lack of direct compensation for allied dental providers which impacts providers as well as patients. It may be unrealistic to consider providing care without means of efficient reimbursement for services rendered. Additional legislation would be required to minimize the obstacles preventing programs from optimally functioning to improve access to care.
Footnotes
Paige M. McEvoy, RDH, MS, is a graduate of the Master of Science in dental hygiene education; Christopher J. Van Ness, PhD. is director of assessment, dental public health and behavioral science; Melanie L. Simmer-Beck, RDH, PhD is a professor and admission enhancement program director for dental public health and behavioral science; Bonnie G. Branson, RDH, PhD is a professor and director of external rotation sites for dental public health and behavioral; Cynthia C. Gadbury-Amyot, RDH, MS, EdD is a professor and director of distance education and faculty development; all at the University of Missouri- Kansas City School of Dentistry, Kansas City, MO.
Kathy Hunt, RDH, ECP II is the dental project director for Oral Health Kansas and project director for the Kansas Head Start Association Cavity Free Kids Program and the Kansas DHL for the Head Start Program of the National Center on Early Childhood Health and Wellness.
This manuscript supports the NDHRA priority area, Population level: Access to care (interventions).
- Received July 26, 2016.
- Accepted March 14, 2017.
- Copyright © 2017 The American Dental Hygienists’ Association





{kind=link}
{kind=link}