



Abstract
Purpose: Evidence suggests that musculoskeletal disorders are a significant health issue for dental health care professionals. The purpose of this study was to compare head tilt angles among dental hygiene students and faculty members when wearing through-the-lens (TTL) as compared to vertically-adjustable-front-lens-mounted (VAFLM) magnification loupes while simulating dental hygiene scaling procedures (DHSP) on a manikin. A secondary purpose was to compare head tilt angles when wearing TTL and VAFLM loupes, to safety glasses while simulating DHSPs.
Methods: A within-subjects, crossover design was used with a convenience sample of dental hygiene students and clinical faculty (n=29). Head tilt angles were measured while participants simulated DHSP wearing TTL and VAFLM magnification loupes. Additionally, head tilt angles were calculated in a subgroup of ten participants while performing DHSP with safety glasses and with TTL and VAFLM loupes. Static photographic images were taken at three time points for each lens type while working in the maxillary and mandibular arches. A video analysis software program was used to calculate calculate head tilt measurements at each time point for each lens types. Data were analyzed using repeated measures ANOVA and Cohen’s d.
Results: Mean head tilt angles were significantly lower when the VAFLM loupes were used in both maxillary and mandibular arches (p = 0.000). Cohen’s effect size value suggested a high practical significance for VAFLM loupes with the mandibular arch (d = 1.21) and a medium to high significance for the maxillary arch (d = 0.70).
Conclusion: Participants demonstrated greatly reduced head tilt angles when using VAFLM loupes as compared to TTL. The magnitude of effect size suggests VAFLM loupes may have a positive impact on in reducing excessive head tilt angles, a known risk factor for musculoskeletal disorders among dental health care professionals.
Introduction
Musculoskeletal disorders (MSDs) represent conditions affecting muscles, nerves, tendons, ligaments, joints, cartilage, or spinal discs. Disorders that worsen in severity and/or duration by specific work conditions are referred to as work-related MSDs.1,2 According to the Occupational Safety and Health Administration (OSHA), work-related MSDs are the leading cause of pain, suffering and disability among American workers.3 The development of work-related MSDs increases significantly when individuals maintain a fixed, awkward posture or perform repetitive routines in the workplace. The maintenance of a fixed, awkward posture while performing a repetitive work routine are common during the provision of dental and dental hygiene care.4,5 The prevalence of work-related MSDs among dentists and dental hygienists has been reported to be between 64 - 93% for all body regions, with the neck, shoulder, wrists/hands, and lower back sustaining the highest percentage of injuries.4-6 Further, evidence suggests MSDs are also a significant health issue for dental and dental hygiene students, developing at higher rates compared to cohorts in other health science programs.7-10
Recommendations for preventing or reducing MSDs include correcting static or awkward posture and minimizing repetitive movements for prolonged periods of time. These recommendations encompass maintenance of a neutral working posture by positioning of patient and operator chairs, using magnification and optimal illumination, taking micro-breaks between patients, and practicing daily preventive exercises.11 Forward bending and repeated rotation of the head, neck, and trunk to one side are frequent upper body positions sustained by dental hygienists during clinical practice. Any type of sustained forward head position is considered detrimental, but a forward head posture of >20° for an extended time is a high risk for clinicians to experience upper extremity pain and discomfort.12
Magnification loupes are considered a principal apparatus in the prevention of excessive forward bending of the head and neck. A body of research supports the use of magnification as an important factor in improved ergonomic posture for both students and practitioners.13-17 However, a systematic review verifying the various aspects studied regarding the influence of magnification on work posture of dentists, reported that the advantages related to ergonomics were based primarily on daily clinical experiences, expert opinions, case reports and data obtained from self-administered questionnaires.14 While there is extensive evidence suggesting a positive impact of magnification loupes (versus no loupes) on posture and work-related MSDs, comparisons between different loupe design features and their ergonomic benefits are limited.
There is a paucity of evidence in the literature demonstrating an association between magnification loupe design, declination angle and ergonomic posture. The most popular design is through-the-lens (TTL) in which the oculars (telescopes) are permanently mounted into the frame’s carrier lens. A randomized controlled intervention with dentists and dental hygienists examined the difference in head and neck flexion angles between TTL loupes (intervention) and safety glasses (control) and identified that TTL loupes decreased head and neck flexion angles by 8.7° and 8.2° respectively, as compared to the control. While it was concluded that magnification loupes can decrease forward head tilt, declination angles were not identified.18
Another design commonly used in dentistry is the front-lens-mounted (FLM) loupes featuring a fixed ocular position on the frame itself. Maillet et al. investigated FLM loupes compared to safety glasses for improvements in working posture. Dental hygiene students were videotaped during clinical procedures while using FLM loupes and safety glasses and their postures were assessed with Branson et al.’s Posture Assessment Instrument (PAI). Results demonstrated that participants using FLM loupes scored significantly closer to ideal posture as compared to using safety glasses alone.16 However, Hayes et al. surveyed practicing dental hygienists to determine their opinions regarding the use of loupes. Only half of respondents indicated that there was a positive change in their posture. While nearly all respondents indicated loupes were a benefit to identification of calculus deposits, only half self-identified a positive change in their posture while wearing loupes.9
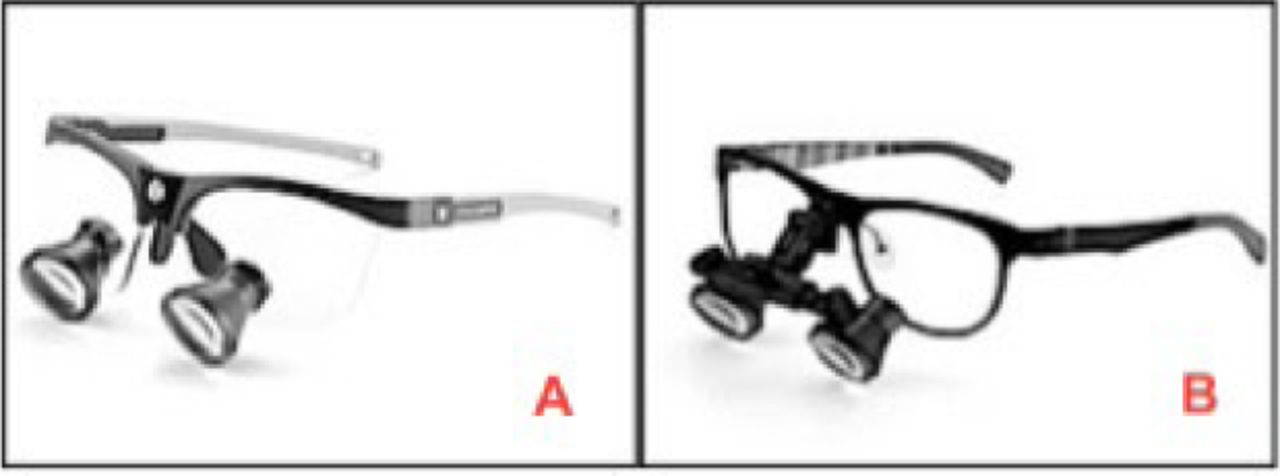
Neither the TTL nor FLM loupe design allows for adjustment of the oculars to increase the declination angle (the angle that the clinician’s eyes are inclined downward toward the work area). The declination angle should be steep enough (40° – 50°) to maintain a minimal forward head posture.19 The recent development of a vertically-adjustable-front-lens-mounted (VAFLM) loupe design incorporates a vertical adjustment of the oculars allowing for a steeper declination angle (40° – 45°) and the potential for a decreased head tilt angle. Through the lens and VAFLM loupes are shown in Figure 1.

Through-the-lens (A) and vertically-adjustable front-lens-mounted (B) magnification loupes
To date, no objective studies have compared the traditional TTL or FLM loupes, routinely used in dentistry, to those with vertical adjustability for declination angle differences relative to forward head tilt. The purpose of this study was to compare head tilt angles among senior dental hygiene students and clinical faculty while wearing TTL loupes and VAFLM loupes during simulation of dental hygiene scaling procedures (DHSP) on a manikin. A secondary purpose was to compare the head tilt angles of a subset of participants while wearing the TTL and VAFLM loupes as compared to safety glasses during the simulated DHSP procedures.
Methods
The study protocol was reviewed and approved by the Institutional Review Board at Idaho State University. A within-subjects, crossover design was employed to identify head tilt angles under two lens types, through-the-lens (TTL) and vertically-adjustable-front-lens-mounted (VAFLM) loupes, during simulation of DHSP on a manikin. A nonprobability, purposive sample of second-year dental hygiene students (n=20) and clinical faculty (n=9) were recruited for this simulation study. A subgroup of participants (n=10) performed DHSP while wearing the TTL loupes, VAFLM loupes, and safety glasses. This subgroup of participants completed the same DHSP procedure with the safety glasses to allow for comparison of results with previous research studies. Only 10 study participants completed the third lens type (safety glasses) due to the overall amount of time needed to complete the simulated procedures and availability of participants. Inclusion criteria required that volunteers only used TTL loupes with 2.5x magnification for training procedures and provision of patient care and previous working distance measurements were on file with the manufacturer (Orascoptic; Madison, WI). Volunteers requiring prescription lenses were excluded from the study; co-axial illumination (head lamp) was not used during any simulation procedures. Written consent was obtained from all participants prior to the simulation exercise. To counterbalance for order, practice, fatigue, and sequence effects, all participants were randomly assigned a sequence for loupe type and alveolar arch order for performing the DHSP.
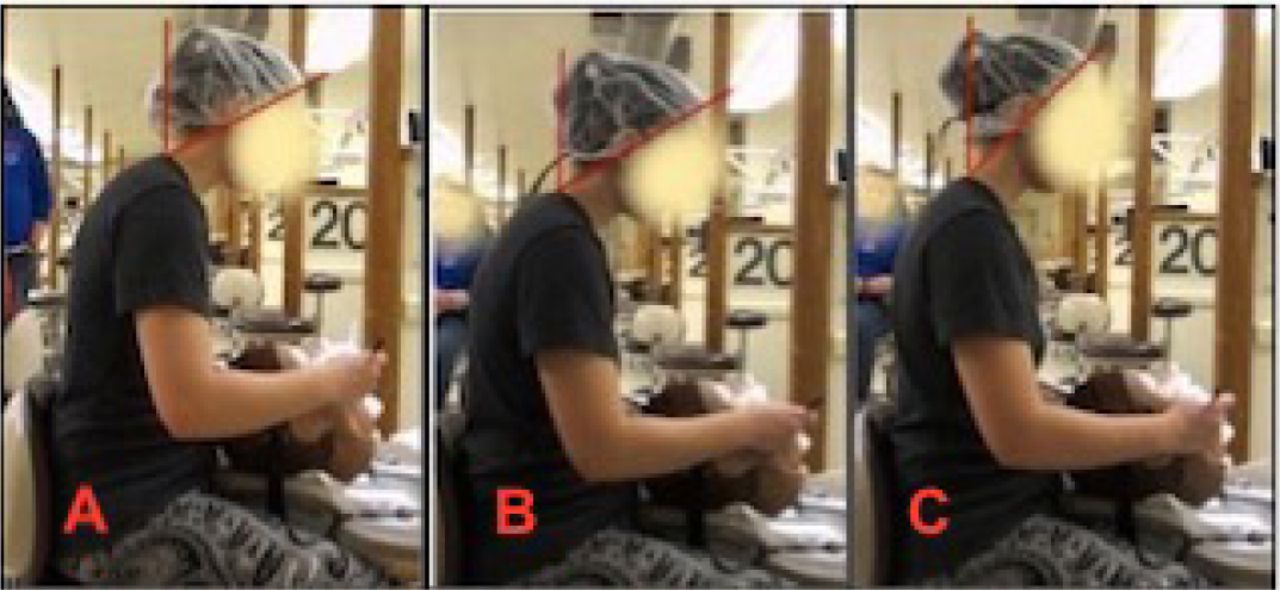
Two weeks prior to the simulation exercise, student and faculty participant names were forwarded to the manufacturer for referencing the previously recorded measurements on file, and fifteen sets of VAFLM loupes with custom working distance ranges were provided for use in this study. Participants signed up for one of three scheduled sessions and two operatories were set up in the dental hygiene clinic for simulation procedures and data collection. Prior to each data collection session, the declination angle and inter-pupillary setting for the VAFLM loupes were adjusted for each participant by the principal investigator (PI) according to the manufacturer’s online tutorial. Participants were allotted two minutes per arch (four minutes total for each loupe type) and asked to complete the simulated DHSP on the lingual surfaces of the upper and lower anterior teeth (canine to canine) of a manikin. Each participant sat at the 12 o’clock working position and used a universal curette and dental mouth mirror for the DHSP simulation. A one-minute rest interval was given to each participant before data was collected for the next loupe type. To capture head tilt angles for each loupe type, two camcorders on tripods, placed to the side and front of participants, were used to record the DHSP. Static photos from the three time points were extracted from the recordings and 2D motion analysis software was used to measure head tilt angles for each lens condition for all time points. Head-tilt angles for each variable are shown in Figure 2.

Head tilt angles during simulated dental hygiene scaling procedures using safety glasses (A), through-the-lens magnification loupes (B), and vertically adjustable front-lens-mounted magnification loupes (C)
Statistical Analysis
Static video images at 50-, 80- and 105-seconds were obtained from the video recordings and analyzed to determine head tilt angle measurements (measured in degrees). Analysis of the static video images was completed using a free, open access 2D motion analysis software program (Kinovea, 0.8.15 version 2). Data were compared for means and standard error of head tilt angles for type of loupe and time when simulating DHSP for anterior teeth of mandibular and maxillary arches on a manikin. Separate repeated measures ANOVA procedures were used to analyze the maxillary and mandibular data. Bonferroni adjusted dependent t-tests and a family-wise error rate of FWE=.05 were used for post-hoc mean comparisons. Cohen’s d (d) was used to identify the magnitude of effect size between the conditions. The effect size interpretation was set at small=0.2, medium=0.5, and large=0.8. All data were analyzed using SPSS version 24 (IBM, Armonk, NY, USA). Significance level for all statistical tests was set at α=0.05.
When analyzing the data for all three conditions, the preliminary statistical analyses indicated the statistical assumption of sphericity for repeated measures of ANOVA was violated for the loupe type and the data of the examination of the maxillary arch, but not of the examination of the mandibular arch. Therefore, the result of the lower-bound conservative test was reported for the maxillary arch data. All other statistical assumptions were met for the statistical analysis. Results for means, standard error, and confidence intervals were reported in degrees.
Results
At total of participants, including dental hygiene students (n=20) and clinical faculty members (n=9) met the inclusion criteria. All participants were female, and the student participants ranged in age from 21 -36 years while the faculty participants ranged in age from 42-61 years. Three fixed time intervals (50-, 80-, and 105-seconds) were examined while performing simulated DHSP on the mandibular and maxillary arches while wearing TTL and VAFLM magnification loupes.
Mandibular arch effects
The main effect on the neck flexion angle for each loupe type was statistically significant (F (1, 28)=63.97, MSE=26.58, p=.000, partial η2=.70) in the mandibular arch. The proportion of variance by the loupe type was 70%, indicating a moderate effect. Flexion angles were significantly lower when participants were working on the mandibular arch while wearing VAFLM loupes (M=49.19, SE=1.28, 95% CI=46.56 – 51.82) than when wearing the TTL loupe (M=55.44, SE=1.13, 95% CI=53.12 – 57.76). The effect size for the difference was large (d=1.21). The main effect for time was significant (F (2, 56)=4.25, MSE=2.67, p=.019, partial η2=.13). There was a slight decrease in the neck flexion angle at the 80-second measurement when compared to the 50-second measurement. However, it was less than a 1° decrease, which is a small effect on the overall neck flexion experienced. While neck flexion increased at the 105-second measurement as compared to the 80-second measurement, this was not significant. The interaction of the loupe type with time was not significant for the mandibular arch (Table I).
Decreased flexion angle of the (vertically-adjustable-front-lens-mounted) VAFLM and the through-the-lens (TTL) loupes and safety glasses (SG) for all participants (n=29) and the subset (n=10)
Maxillary arch effects
The main effect on the neck flexion angle for each loupe type was statistically significant (F (1, 28)=21.55, MSE=37.81, p=.000, partial η2=.44) in the maxillary arch. The proportion of variance by the loupe type was 44%, indicating a small to moderate effect. Flexion angles were significantly lower when participants were working in the maxillary arch while wearing VAFLM magnification loupes (M=41.71, SE=1.18, 95%CI=39.30 – 44.12) as compared to the TTL loupes (M=45.80, SE=1.03, 95% CI=43.92 – 48.15). Effect sizes for the differences were moderate (d=0.70). The main effect for time was not significant (F (2, 56)=1.47, MSE=3.14, p=.24, partial η2=.05). The interaction of loupe type with time was not significant for the maxillary arch (Table I).
Magnification loupes versus safety glasses
A subset of the participants (students, n=7; faculty, n=3) performed the DHSP procedures while wearing safety glasses in addition to the two types of magnification loupes. When comparing the head tilt angles while using TTL and VAFLM magnification loupes, repeated measures ANOVA indicated head tilt angles during instrumentation procedures for both arches were significantly lower when wearing the VAFLM loupes as compared to wearing either the TTL loupes or safety glasses alone. Moderate to large effect sizes of decreased head tilt angles were found when wearing the VAFLM loupes type during simulated procedures performed in both arches while seated in the 12 o’clock position (Table I).
Discussion
To the authors’ knowledge, research comparing the effects of magnification loupes with vertical adjustment on forward head posture (head tilt angle), working posture or upper extremity pain and discomfort has not been reported in the literature. Results of this study indicated head tilt angles when using VAFLM magnification loupes as compared to TTL were significantly decreased during simulated DHSP performed on a manikin. Findings were similar in a subset of the sample when with the added variable of safety glasses. While the use of TTL loupes showed a slight decrease in head tilt angle (<2°) as compared to safety glasses alone, VAFLM loupes displayed the greatest reduction in head tilt angle. The VAFLM loupes allowed the participants to maintain a decreased head tilt angle when viewing either arch in the manikin’s oral cavity. This decrease in head tilt angle may be related to the adjustability feature of the VAFLM lenses for full coaxial alignment.18 Through the lens and FLM magnification loupes have a higher likelihood of coaxial misalignment, which may result in increased head tilt angles.
Perhaps the most remarkable finding arising from this study was the magnitude of effect size exhibited by use of VAFLM loupes compared to both TTL loupes and safety glasses. The effect size of the VAFLM on head tilt angle was large for all conditions in both arches, indicating that the VAFLM has a clinically significant effect on head tilt angles during a simulated DHSP. Effect size provides a truer measure of the magnitude of effect between variables over statistical significance alone because the influence of sample size is minimal.20,21 Similarly to other studies, VAFLM magnification loupes were associated with clinically relevant improvements in head tilt angle as compared to TTL loupes and safety glasses.22
The amount of decrease in head tilt angle was dependent on which arch was being assessed. Thus, the declination angle required to maintain a neutral head tilt may be different when assessing the mandibular arch than the declination angle required for the maxillary arch. Additional research is needed to determine the optimal declination angle for each arch. This study was carried out on manikins from a 12 o’clock position. The declination angle required for performing dental hygiene procedures may differ depending on the position where the procedures are performed. Future research is needed to provide optimal declination angles for both arches at different seating positions.
The findings demonstrating no difference in head-tilt between using the TTL and safety glasses are consistent with those of Ludwig et al.23 on the effects of magnification loupes on posture. However, other studies have demonstrated that magnification loupes improve posture.15,16 While neck pain was not analyzed in this study, research has shown that magnification loupes may have a positive effect in decreasing neck pain.19 Additional research is needed to determine the effect of VAFLM loupes on neck pain.
Due to the amount of time to complete the simulated procedures and the availability of the participants, only 10 study participants completed the safety glasses portion of this study, limiting the findings. The small number of participants may have affected the ability to detect true differences in head- tilt positions. During analysis of the data for all three conditions (VAFLM, TLT, safety glasses), the statistical assumption of sphericity for repeated measures of ANOVA was violated for the DHSP performed in the maxillary arch. This violation likely occurred due to the small number of participants (n=10) who completed all three conditions. Additional research is needed with a larger sample to further determine the differences between the head tilt angles when conducting objective measurements while performing simulated DHSP.
This study has other limitations. A convenience sample of students and clinical faculty was used for recruitment of participants and results may not be representative of the entire population. Participants were video recorded during DHSP and may have modified aspects of their posture in response to being recorded. Several extraneous variables may have influenced outcomes as well. The lever to open and close the manikin’s mouth protruded two inches beyond the dental chair headrest, making it difficult for participants to get close enough to the dental chair for optimal intraoral visualization. Participants may have already adapted a less than optimal working posture from previous clinical experiences, or the established TTL loupe working distances may not have been accurate. All instrumentation procedures were performed from the 12 o’clock position, and some participants may have been trained to approach anterior teeth from different clock positions. Future studies should include a broad sample of practitioners and students with varying levels of experience. Further studies should examine effects of magnification loupes on overall posture during instrumentation in all six sextants of the mouth in patients.
Conclusion
Vertically adjustable, front-lens-mounted magnification loupes demonstrated greater reductions in head tilt angles as compared to TTL loupes and safety glasses among dental hygiene students and clinical faculty participants. The large scale of effect size for VAFLM loupes resulted in a clinically relevant improvement in head tilt angles which may translate into enhanced overall posture and ultimately, a reduction of upper extremity MSDs among dental health care providers. More research is needed to compare the various types of magnification loupes in a larger population. Further study is needed to identify the ergonomic benefits of improved posture over time, to the reduction of pain and prevention of work-related MSDs.
Footnotes
This manuscript supports the NDHRA priority area Professional development: Occupational health (determination and assessment of risks).
Disclosure
Orascoptic™ (Madison, WI) provided the vertically-adjustable-front-lens-mounted magnification loupes for the study. The company had no role in the design, conducting of the study or in reporting of the results.
- Received February 6, 2020.
- Accepted March 10, 2020.
- Copyright © 2021 The American Dental Hygienists’ Association





{kind=link}
{kind=link}