



Abstract
Purpose: Obstructive sleep apnea (OSA) is a common breathing disorder; however, many individuals remain undiagnosed. The purpose of this study was to assess the comfort level of community-dwelling adults to participate in OSA screening in a dental office setting and survey the OSA risk levels of an adult population.
Methods: This cross-sectional study was conducted among adults presenting at the University of Minnesota Driven to Discover Research Facility during the 2018 Minnesota State Fair. Participants completed a brief survey including the eight-item STOP-Bang questionnaire for OSA screening. Electronic tablets were used for data capture. Data analyses included descriptive statistics, t-tests, and Chi-square tests.
Results: A total of 639 adults met the survey inclusion criteria (n=639). The majority of participants (88%) reported no prior OSA diagnosis. Based on STOP-Bang criteria, 61% (n=344) of the participants were at low, 29% (n=161) intermediate, and 10% (n= 56) high risk of OSA. A majority (64%) of participants reported being either “comfortable” or “very comfortable’”with OSA screening performed in a dental office setting.
Conclusion: Over one third of participants with no prior OSA diagnosis were at moderate to high risk for OSA, and the majority stated that they would be comfortable undergoing OSA screening in a dental office setting. Dental hygienists screening patients for OSA with the STOP-BANG questionnaire are likely to have a high level of patient acceptance. Referring patients to the appropriate health care provider for further testing may increase timely diagnoses and treatment of OSA.
- obstructive sleep apnea
- sleep disordered breathing
- STOP-Bang questionnaire
- health screenings
- dental hygienists
Introduction
Sleep disordered breathing (SDB) has risen along with obesity in the United States (US). A recent estimate of the prevalence of mild to severe SDB is projected to be 26% for persons 30–70 years of age.1 Although obstructive sleep apnea (OSA) is one of the most common sleep disorders among US adults, an estimated 80% of cases remain undiagnosed.2,3 Obstructive sleep apnea is characterized by repetitive collapse of the airway during sleep,4,5 followed by arousal, which reverses airway collapse and restores normal oxygenation and ventilation. These episodes are associated with dysfunction of the autonomic nervous system and increases in oxidative stress.6 These episodic processes may explain the association between OSA and cardiovascular diseases including hypertension, heart failure, arrhythmias, and stroke.7, 8, 9 Of specific relevance to oral health care providers, OSA has also been identified as a contributing factor to inflammation, as measured by elevated levels of inflammatory cytokines,10 with several studies reporting an association with periodontal disease.11-14
Key risk factors for OSA include obesity, hypertension, large neck circumference, advanced age, and male gender.4,15 Symptoms of OSA include general fatigue and excessive daytime sleepiness; loud snoring; and witnessed apneic events.4 A useful clinical screening tool that is rapidly becoming the standard for a quick OSA assessment is the 8-item STOP-Bang questionnaire (see Figure 1).16 The instrument consists of four subjective items (STOP: Snoring, Tiredness, Observed apnea, and high blood Pressure) and four demographic items (Bang: BMI, age, neck circumference, and gender).17 Total STOP-Bang scores range from 0 to 8, with scores of 0-2 indicating low risk for OSA, whereas scores of 3 or more, demonstrate a significantly increased risk of OSA.5 The questionnaire can be completed in 1-2 minutes and requires minimal training to administer.
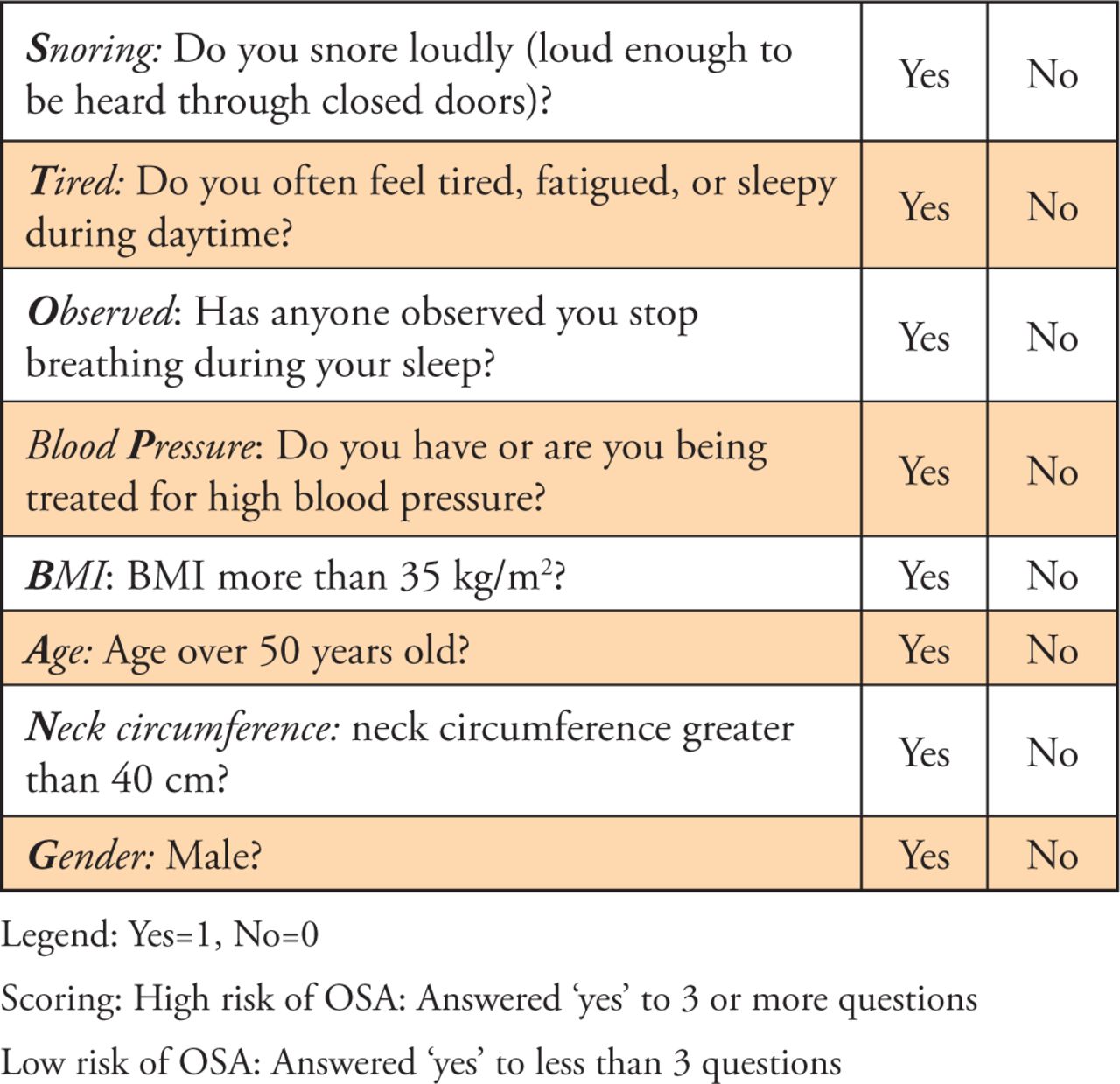
STOP-Bang Questionnaire20
Patients assessed at increased risk for OSA should be referred to the appropriate health care specialist for further testing and diagnosis. A definitive OSA diagnosis is obtained by conducting a polysomnograph (i.e., sleep study), in consultation with a sleep medicine physician.10,18 Based on this essential information, the etiology and severity of the OSA is determined, followed by an appropriate treatment plan. Continuous positive airway pressure (CPAP) is the gold standard treatment for most patients diagnosed with OSA. The CPAP uses high pressure to force air through the airway to prevent collapse during periods of sleep.4
For individuals who are intolerant of CPAP treatment (25-58%), other treatment options are prescribed.19 Mandibular advancement devices (MAD) are oral devices that advance the mandible and tongue to prevent the collapse of the upper airway during sleep.20-22 These devices are fitted and maintained in dental settings, in collaboration with medical professionals. Several visits are often required to adjust these devices to the ideal position for patients. Similar to the CPAP, patient compliance is a concern, with only 32% of patients using an oral appliance regularly.23 Long-term compliance is also a concern, with many as 55% of patients stopping use of the oral appliance within the first year. Of those who discontinued treatment, 62% reported an inability to adapt to the device and 38% reported temporomandibular pain associated with device use.23 Additional treatment options include airway surgery and hypoglossal nerve stimulation during sleep.24 Successful treatment has been shown to improve both quality of life and cardiovascular outcomes.24,25
Dental hygienists are well-positioned to screen and refer patients for further diagnostic testing, due to their knowledge of head and neck anatomy and because routine dental visits often occur at a higher frequency than primary care visits.26 While the STOP-Bang questionnaire can easily be used in dental offices to identify patients at risk for OSA, it is not clear whether patients would be comfortable undergoing OSA screening during dental visits. The purpose of this study was to determine individuals’ comfort level in completing the STOP-Bang questionnaire in the dental office setting. Secondary goals were to determine the proportion of patients at risk for OSA in an adult population and assess their most recent dental and medical visits.
Methods
This descriptive study was conducted among a convenience sample of adult attendees at the Minnesota State Fair in August 2018. A short survey was administered during two five-hour data gathering sessions at the University of Minnesota Driven to Discover Research Facility. The study was described to potential participants who approached the study booth, and written consent was obtained. Subjects were asked to complete the survey using an electronic device with a touchscreen. Research staff were available to assist participants who needed technical assistance. No personal identifying information was obtained from the participants. Inclusion criteria were age 18 and older and English literacy.
A brief original survey was designed for specific use in this study. Demographic and health history questions were included to assess participants’ most recent medical and dental care visits, age and sex assigned at birth, and prior medical diagnoses. Prior medical diagnoses questions (yes/no) included OSA, hypertension, cardiovascular diseases, stroke, periodontal disease, and diabetes. The risk of OSA was determined using the STOP-Bang questionnaire. The final item asked the participant’s level of comfort completing a similar survey in the dental office setting: response choices used a 5-item Likert scale, ranging from 5=very comfortable, to 1=very uncomfortable.
While the overall survey instrument was not validated, the psychometric properties of the STOP-Bang questionnaire have been tested extensively.27 Development of the instrument was based on initial factor analysis of the STOP questionnaire components, selected from 14 initial questions designed to reflect snoring, daytime tiredness, observed breathing cessation, and high blood pressure. The “Bang” items were chosen based in univariate analysis of items predictive performance. Subsequent analysis have focused on the predictive validity of the screening instrument compared to definitive sleep study results. In a recent meta-analysis, the instrument sensitivity was shown to be high (90 to 96%) although specificity was somewhat low (25-49%).17 This combination of high sensitivity and lower specificity allows the questionnaire to capture almost all participants who truly have OSA for further diagnostic screenings, which uses the definitive sleep study to rule out OSA diagnosis for those not having it.
The study was submitted to the University of Minnesota Institutional Review Board and deemed exempt from further review. The study staff communicated to participants that study participation was not a substitute for a medical assessment. Resources and educational materials were available for participants who were concerned regarding their OSA risk. A paper copy of the STOP-Bang was available for attendees to take home and complete, that included scoring and follow-up recommendations. Referral to a medical provider was also available for interested participants.
Analysis included calculating participants’ risk of OSA using the standard scoring of the STOP-Bang questionnaire. Scores of 5-8 were deemed high risk, scores of 3-4 moderate risk, and scores of 0-2 low risk.28 Descriptive statistics (means and standard deviations for continuous measures; counts and proportions for categorical measures) were used to describe the sample. Characteristics were compared between those with and without an OSA diagnosis and between OSA risk categories (low, moderate, high) for those with no prior OSA diagnosis using two-sample t-tests or one-way ANOVAs for continuous variables and Chi-square tests for categorical variables.
Results
A total of 646 adults completed the survey. Responses from seven participants were excluded from the analysis due to participants not providing written consent, despite completing the survey, for a sample size of 639. Table I displays the characteristics of the study participants. The majority of participants were female (59%) with a mean age (standard deviation [SD]) of 51.1 years (17.0). A majority reported having a medical (83%) or dental visit (84%) within the past year. The most frequently reported OSA comorbidity was high blood pressure (22%) followed by periodontal disease (15%). Nearly two-thirds (64%) indicated that they would be “very comfortable” or “comfortable” completing an OSA screening questionnaire in a dental office setting.
Demographic characteristics (n=639)
The characteristics of participants with and without an OSA diagnosis are displayed in Table II. As expected, those diagnosed with OSA were older (p<0.001), more likely to be male (p<0.001), had more recent medical visits (p=0.014), and a higher prevalence of diabetes (p<0.001) and hypertension (p<0.001). No statistically significant differences were found for the most recent dental visit or level of comfort with OSA screening in a dental office. Characteristics of participants that had not previously been diagnosed with OSA by STOP-Bang risk category are shown in Table III. Participants in higher risk categories were more likely to be older (p<0.001) and male (p<0.001). A majority of participants with a high-risk score reported visiting a medical (50%) or dental provider (55%) in the last 6 months. The majority of all risk groups were “very comfortable” or “comfortable” with OSA screening in a dental setting. No statistically significant differences were found by risk category for most recent medical or dental visit, or comfort with OSA screening in a dental office.
Characteristics of the study population by prior OSA diagnosis (n=639)
Participant characteristics with no prior OSA diagnosis by STOP-BANG OSA risk (n=561)
Discussion
Obstructive sleep apnea is a common but often undiag-nosed medical disorder that is associated with numerous medical comorbidities including heart disease, stroke, and periodontal disease. Risk factors for OSA, such as advanced age, male gender, obesity and large neck circumference are easily identifiable and can be rapidly assessed using the STOP-Bang questionnaire. Screening for OSA facilitates identification of high-risk patients who could benefit from further diagnostic testing and treatment.
Results from this study identified that, over half of participants who were not previously diagnosed with OSA indicated that they would be either “very comfortable” or “comfortable” completing OSA screening in a dental setting. Only 9.0% indicated that they would be “uncomfortable” or “very uncomfortable” completing OSA screening in the dental setting. These results suggest that the vast majority of adults in the general public may be willing to undergo OSA screening during dental visits. While no other studies of the general public are available, one previous study among dental patients found that approximately 50% expressed acceptance of OSA screenings in a dental office setting.29 However, it should be noted that a variety of OSA screenings exist.
Currently there are few studies regarding OSA screening practices in dental offices and follow-up treatment after OSA diagnosis. One study conducted among practicing Minnesota dental hygienists reported that about 10% had an established OSA screening protocol in their practice settings and no single screening instrument was used more frequently than another.30 In a separate study, dentists were surveyed to establish the frequency of OSA screening in the dental office.31 While 76% of the dentists reported screening for OSA, only 14% screen every patient.31 Unfortunately the low response rate (7%) of that study make the results difficult to generalize the population as a whole.31
In this study, most participants (76.4%) who were categorized as at moderate or high risk of OSA, based on the STOP-Bang scoring, did not report being previously diagnosed with OSA. This is consistent with the estimated 80% of moderate to serve cases of OSA in the US that are undiagnosed.16 This high percentage of undiagnosed individuals may benefit from a screening intervention to help identify, diagnose, and provide treatment before serious medical conditions arise or worsen.
Daytime sleepiness due to OSA has been linked to multiple workplace and public health risks. Individuals with untreated OSA have a two-fold increases in workplace accidents.32 Commercial drivers have been studied with concern over road fatigue and OSA effects, resulting in about 7% of motor vehicle accidents (MVAs).32 Policies for commercial drivers have been developed related to their abilities to perform driving tasks safely, and discussion of the impact OSA on non-commercial drivers has begun.33
In addition to performance issues, OSA is associated with safety concerns for patients undergoing surgery requiring anesthesia. Individuals with OSA are at a higher risk for cardiovascular and cardiopulmonary complications post-operatively.34 Preoperative screenings for OSA, using the STOP-Bang, is recommended to identify patients with moderate to severe OSA risk.17
A percentage of participants in this study indicated that they had seen a dental provider within the last 12 months. Among moderate-risk patients, 79% of patients indicated that they had visited a dentist within 12 months. Among high-risk patients, 89% had visited a dentist within 12 months. Corresponding numbers for physician visits were 84% for intermediate-risk participants and 82% for high-risk participants. This suggests that there is opportunity for OSA screening at either the dental office or medical office for most at-risk patients. However, opportunistic screening medical offices is generally poor, as patients’ primary complaints take diagnostic precedence, thus creating a need which could be filled by dental hygienists.23
The dental office may be an ideal setting for OSA screening, as dental hygienists have the necessary knowledge base to identify anatomical risk factors for OSA and preventative care dental visits occur on a regular basis. A recent study among practicing Minnesota dental hygienists found that participants viewed OSA as either an important, very important, or extremely important clinical disorder (92.9%) with similar responses regarding the importance of identifying patients with possible OSA (92.3%).30 Recognizing the importance of OSA may indicate that dental hygienists would willingly incorporate OSA screening into routine dental hygiene care.
This study had limitations. First, this survey was completed at a research booth by participants who willingly approached the researchers and consented to the study and may not be representative of the general population. Participants in this study, due to selection bias, may be more comfortable completing questionnaires (e.g., the STOP-Bang) than members of the general population or the population that seeks regular dental care. Moreover, it is possible that participants who approached the research booth were more likely than members of the general population to seek either dental or medical care, thus the data for date of most recent dental and physician visits may be biased.
Based on these findings, further research is needed in several areas. The first is to determine the attitudes of dental hygienists regarding OSA screenings in clinical practice and appointment time management. Attitude measures will help project how these screenings can be incorporated into routine dental hygiene care appointments. Additional assessment of current screening protocols will establish further recommendations for development of an OSA screening, referral, and OSA treatment protocol. It is also essential to determine how OSA screenings can be effectively implemented and how to collaborate with medical professionals to obtain a formal OSA diagnosis and assist in treatment implementation.
Conclusion
Results from this study demonstrate that a large proportion of community adults in Minnesota are at moderate to high risk for obstructive sleep apnea. These individuals would be comfortable undergoing screening for OSA in a dental office and had visited the dentist over the previous 12 months. Dental hygienists are well positioned to implement OSA screening and initiate referral protocols in Minnesota dental offices.
Acknowledgements
The authors would like to extend their appreciation to the following dental hygienists who assisted with survey administration and confirmed the ease of administration of the STOP-Bang questionnaire: Kelli Blankenship, Shannon Borowicz, Danna Hickey, Bridget Hotzler, Julie Klegin, and Holly McColl.
Footnotes
This manuscript supports the NDHRA priority area: Professional development: Education (Interprofessional education).
Disclosure
This research was supported by the National Institutes of Health’s National Center for Advancing Translational Sciences, grant UL1TR002494. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health’s National Center for Advancing Translational Sciences.
- Received July 10, 2019.
- Accepted February 26, 2020.
- Copyright © 2021 The American Dental Hygienists’ Association





{kind=link}