




Ann Eshenaur Spolarich, RDH, PhD, FSCDH
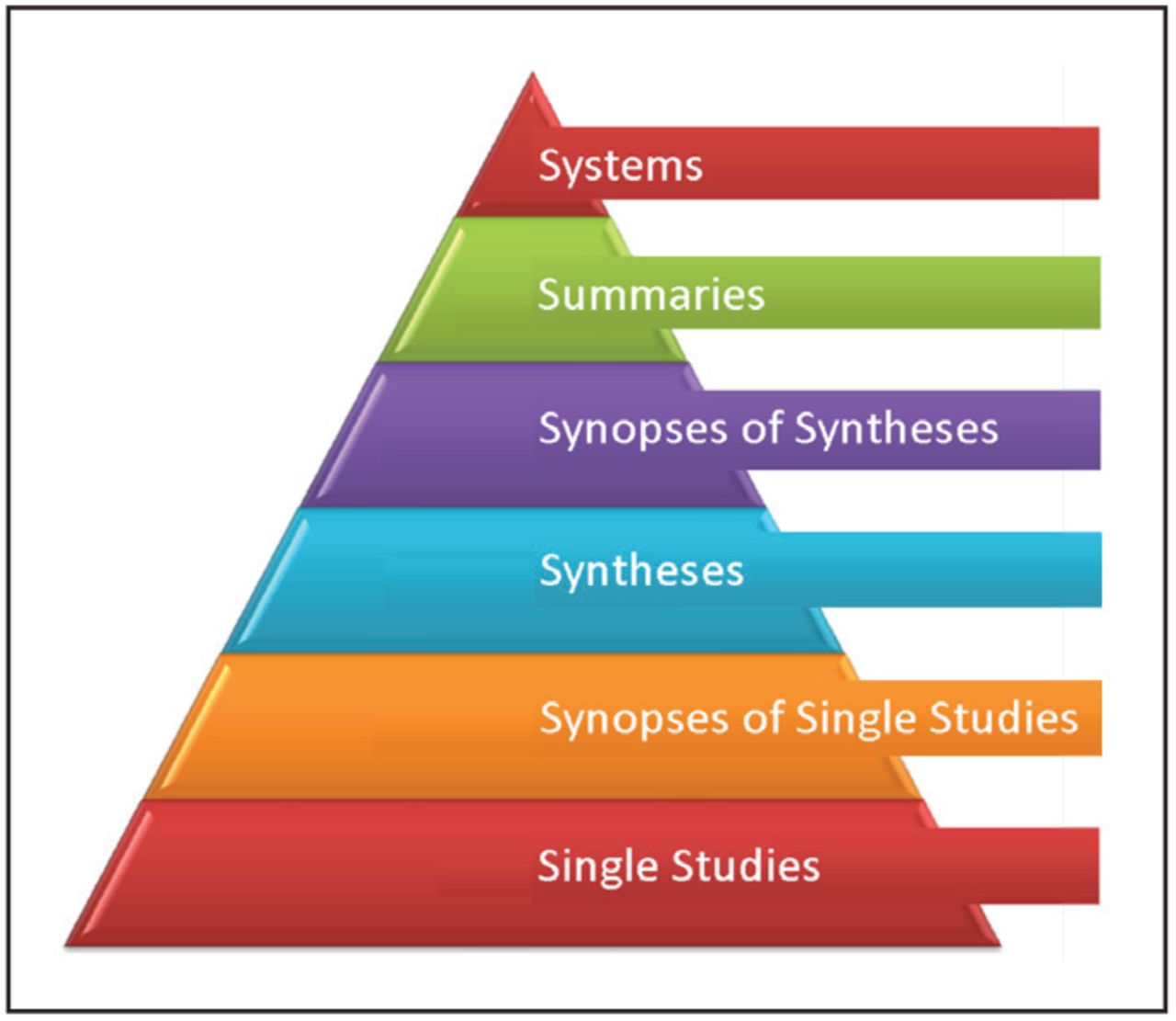
In 1997, the American Dental Hygienists' Association (ADHA) House of Delegates approved a policy supporting that dental hygienists should adopt an evidence-based philosophy of practice.1 Inherent in this philosophy is the emphasis placed on patient-centered care which requires practitioners to use and apply current research findings in clinical decision-making and for the planning and delivery of care. Since its inception, the model of evidence-based practice (EBP) has evolved tremendously, bringing together the clinical setting with patient preferences, healthcare resources, and the best available research evidence to reach a final course of action informed by clinical expertise.2 The manner in which clinicians obtain current best evidence has also evolved, as depicted by the updated evidence pyramid known as the 6S pyramid.3 (Figure 1) The hierarchy depicted in the 6S pyramid implies increased validity and applicability with synopses and summaries of pre-appraised evidence, as single studies are not likely useful to clinicians as they often lack the necessary skills to identify and appraise these studies for application to practice.4 The highest levels of evidence integrate evidence-based information about specific clinical problems and include summaries which contain updated clinical practice guidelines (CPG) and clinical decision support systems for use at the point of care.3
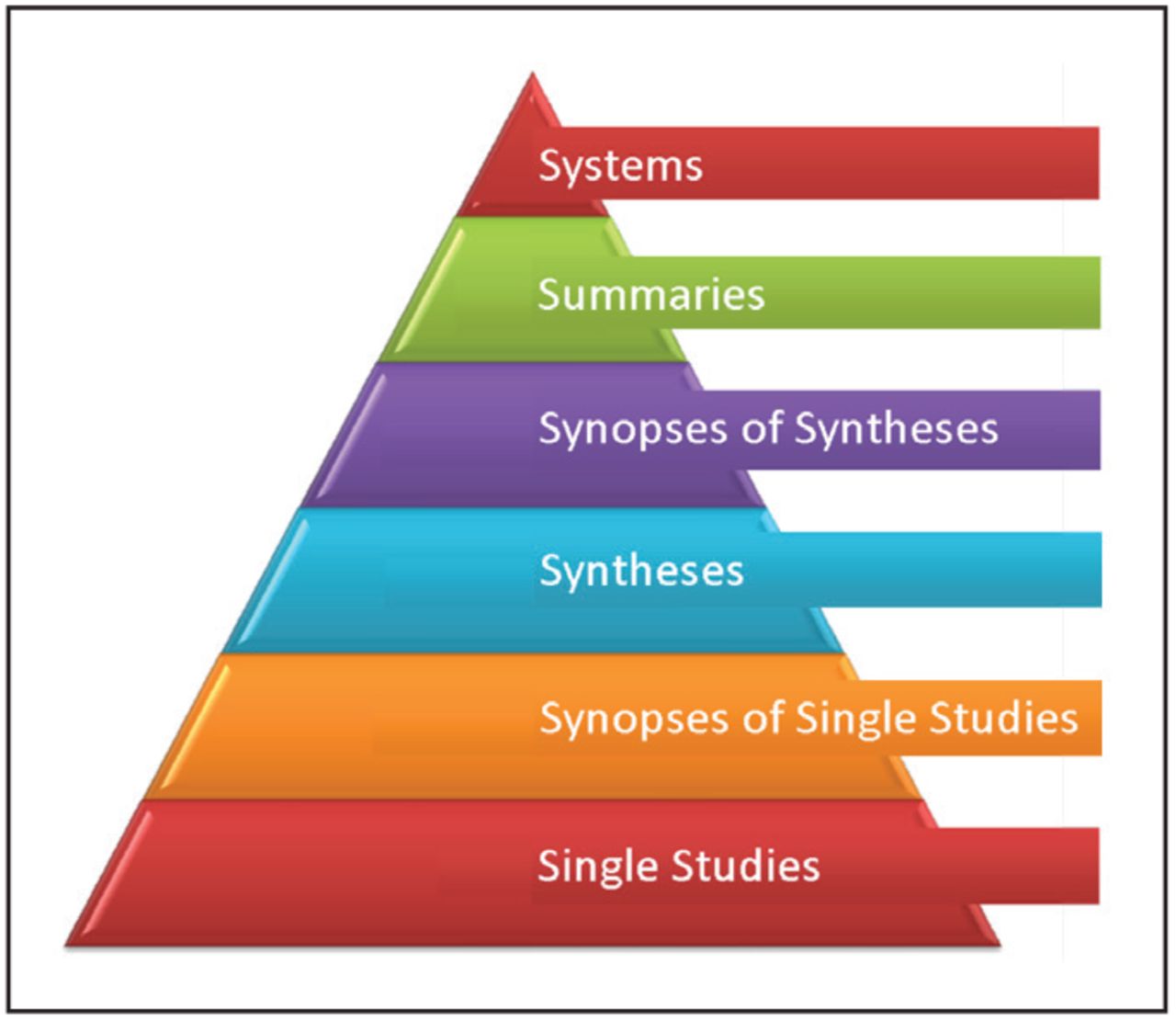
The 6S Pyramid3
The American Dental Association (ADA) Center for Evidence-Based Dentistry defines CPG as “the strongest resources to aid dental professionals in clinical decision making and help incorporate evidence gained through scientific investigation into patient care. Guidelines include recommendation statements intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options.”5 CPG are widely available in the published medical literature for hundreds of health conditions, yet adoption of these guidelines is often poor and/or slow. Barriers to implementation and adherence are attributed to various practitioner, patient and environmental factors. There are far fewer published CPG in dentistry, yet similar problems with adoption and application can be observed.
There are good examples of barriers to implementation and adherence to published CPG by dental hygienists. Two studies have been published that document poor adherence to the ADA and US Food and Drug Administration (FDA) guidelines for Dental Radiographic Examinations.6 First, a survey was done with a nationwide sample of practicing dental hygienists to assess their knowledge and practice behaviors related to the guidelines.7 The majority of the 517 respondents reported that there were times when a clinical examination was not performed before imaging and that images were ordered based upon a set time interval, such as insurance reimbursement criteria, as opposed to determining need for imaging based on actual patient risk assessment data as outlined in the guidelines for frequency of exposure. Behaviors also differed by type of practice setting (general/private, corporate or academic).7
A second study with a convenience sample of 1,500 dental hygienists assessed practice behaviors related to respondents use of the guidelines, including use of patient selection criteria and radiation safety.8 Most of the 566 study participants had an associate's degree (62%) and the majority had over 30 years of experience. Study findings revealed that dental hygienists with more years of experience were more likely to follow selection criteria from the guidelines, and those with higher levels of education (eg. bachelor's degree or higher) or who had recently taken continuing education about dental radiation safety were more likely to use techniques to reduce radiation exposure.8 Both of these studies demonstrate provider barriers: poor knowledge about and failure to apply and adhere to CPG.
The Ask-Advise-Refer guideline has been widely used by healthcare professionals for smoking cessation, but implementation remains low.9,10 A recent cross-sectional study examined to which extent 883 healthcare providers from different professions expressed their intention to implement a smoking cessation program with their patients and identified barriers to implementation; 58 participants were dental hygienists.11 Hygienists scored as “average” on their intention to use the guideline compared to other professionals, but scored higher on intention than cardiologists and internists, and similarly to dentists. Sixty-four percent of hygienists reported “asking”, 41% reported “advising” and 26% reported “referring” all patients for smoking cessation. Only 66% of the hygienists reported that they documented smoking status for all patients. For patients who were smokers, 45% reported assessing motivation to quit, 53% discussed barriers to quitting, 14% helped patients make a quit plan, 10% advised the use of pharmacotherapy, 12% arranged a follow-up discussion, but 41% reported doing some type of short, motivational intervention to assist with quitting. Half reported advising all new patients to quit, with higher rates of quit advice given to those patients who reported smoking-related complaints (64%), those who were about to undergo surgery (72%) and those who were pregnant (76%). Identified provider barriers to implementation were lack of formal training in the guidelines (59%) and the sensitive nature of the topic (60%). The largest environmental barrier identified was lack of time (40%).11
A qualitative study of 30 dentists, dental hygienists, dental assistants and dental practice managers examined factors that influenced implementation of the pit and fissure sealant guidelines in the Kaiser Permanente Dental Program.12 Data from focus groups revealed that environmental barriers to implementation included a lack of infrastructure for guideline communication and dissemination, and resource constraints, including adequate space and materials. Provider confusion about their roles and responsibilities for implementing the guidelines was also attributed to the lack of infrastructure. The investigators concluded that establishing a robust infrastructure that contains standardized, predictable mechanisms for implementation is necessary for adoption of CPG in the dental setting.12
Several studies have been done to examine dental hygienists use of adjunctive screening devices for detection of oral cancer.13-15 The ADA CPG for evaluating potentially malignant oral lesions concluded that none of these adjunctive devices demonstrate sufficient diagnostic test accuracy to support their use as triage tools for lesion evaluation.16 Anecdotally, use of these devices continues in practice, despite strong evidence that these devices lack specificity and sensitivity.17 No studies have been done to assess dental hygienists adherence to the published ADA CPG for assessing oral lesions in practice.
Compliance with well-established guidelines for antibiotic prophylaxis (AP) to reduce risk for infective endocarditis (IE) and prosthetic joint infection is an ongoing challenge despite the availability of updated consensus guidelines and clinical decision support tools.18-20 Reasons for lack of compliance include but are not limited to fear of litigation, deference to a medical provider's opinion, perceived safety of a single antibiotic dose, lack of understanding of risk: benefit and patient selection criteria, confusion with conflicting guidelines, habitual prescribing habits, pressure from patients and peers, and apathy. Clinical decision-making is often hampered by these implementation barriers, as evidenced by several studies.21,22 Of note, new CPGs recommend involving the patient in shared decision-making when discussing AP;19,20 however, there is no data about whether dental hygienists engage in shared decision making (SDM) with patients when determining need for AP.
The premise of SDM is based on the concept that the clinician serves as expert about scientific evidence and the patient serves as expert on what matters most to them.23 Numerous models of SDM have been proposed to identify key components and to better define who is responsible for which elements during information exchange.24 Newer models place a greater emphasis on the patient who is facing the treatment decision, expanding patient-centered care to relationship-centered care or humanistic communication.25,26 A recent systematic review examined 40 SDM models and identified critical components that are common to most models regardless of healthcare setting: describe treatment options, make the decision, and patient preferences.24 Model components that differ between settings include create choice awareness, provide recommendations, and offer time.24 Of note is that patient expertise and healthcare professional expertise are rarely present in any SDM models; however, learning about the patient is an important strategy when determining patient expertise.24 SDM is especially important when treatment decisions are preference-sensitive, when benefits are limited or uncertain, or when potential harms may impact a patient's quality of life.27 Dentistry faces the same dilemma as oncology: it is unknown if recommendations in current CPGs identify preference-sensitive decisions that require patient engagement in SDM and ultimately, for implementation.27
To illustrate the concepts of SDM and CPG adoption, 2 examples from the literature are presented here. The evidence-based National Institute for Health and Clinical Excellence (NICE) recommendations for AP before dental treatment were released in the United Kingdom in 2008, eliminating the need for AP to prevent IE in children and adults with structural heart disease when undergoing dental procedures.28 One team of investigators conducted a qualitative study to identify patient attitudes and views about barriers and facilitating factors that could influence implementation of the new guidelines in nine patients who were at risk for IE and had a history of receiving AP.29 Framework analysis30 revealed that patient barriers to acceptance were related to fear of IE, which was strongest among those who had experienced IE. Personal experience with antibiotic side effects was an influencing factor more so than the scientific evidence presented. Beliefs that dental treatment was a cause of IE and that AP acts as “insurance” against developing IE with dental treatment made patient acceptance of the guidelines difficult. However, the other major barrier to acceptance was the lack of consensus among health professionals about the recommendations in the guideline which caused patient confusion. Patients understood that advances in science change the standard of care but preferred an individualized assessment over just following the guidelines alone for determining need for AP. The key take-away was that scientific information provided to the patients did not change their beliefs, who stated that information about a guideline recommendation should come from an expert clinician who was known and trusted. If the dentist and cardiologist reached consensus, then patients felt more confident in adopting the recommendation.29
A different study explored patient-related implementation barriers among individuals with total prosthetic joint replacement (TPJR).31 An identical survey measuring compliance with recommendations for AP was given to 263 patients with TPJR: 143 at an orthopedic center and 120 at a dental center. The investigators identified the primary outcome as the percentage of patients who complied with their recommendations to take AP prior to undergoing a dental procedure. Their secondary outcome was to assess whether patients believe that antibiotics should be taken indefinitely or for a shorter, arbitrary duration. The practice environments were selected because clinicians in both settings always recommend AP prior to dental treatment for patients with TPJR. In the orthopedic clinic, 50% of the patients complied and in the dental setting, 21% complied. More than half of the patients in both groups reported that APs was “not applicable” to their condition. There were no differences in perceived necessity of use between the groups: approximately half of subjects in both groups deemed AP as appropriate after TPJR in some form, but perceptions about when and for how long AP was necessary varied considerably among patients in both groups. The investigators reported that all patients received consistent education about the need for prophylaxis from their orthopedic surgeon, but there was no mention on what information that education was based. No mention was made as to whether patients participated in SDM; however, lack of compliance infers that patients made their own decision about AP independently from the education provided. The investigators also discussed that clinicians and patients are challenged by conflicting CPG between professional organizations, citing an older guideline32 versus updated consensus guidelines, inadvertently illustrating their point.20,32 Findings from these small studies underscore the importance of patient participation in SDM for guideline implementation as part of patient-centered care, where patients and clinicians negotiate application of the evidence on an individualized basis.33
Dental hygiene researchers have several unique opportunities to further explore the concepts presented in this paper. First, there is a need to study patient preferences and participation in SDM in response to treatment recommendations presented as part of the dental hygiene process of care. Attention should be paid to the selection of and reporting of the SDM models used in this research. Second, barriers to implementation of CPG in dental hygiene practice need further identification. Documentation of provider, patient and environmental factors that influence adoption and application of CPG should be consistently reported as new CPG evolve. Third, researchers require additional training in implementation science methods to conduct robust studies that will meaningfully contribute to the dental hygiene body of knowledge and support evidence-based practice. Finally, our academic institutions must model the implementation of CPG as they are released, including use of SDM with patients, so that dental hygiene students are socialized to practicing with current best evidence.34
Footnotes
Ann Eshenaur Spolarich, RDH, PhD, FSCDH is a professor and the Director of Research, Arizona School of Dentistry & Oral Health, A.T. Still University, Mesa, AZ.
A message from the Editor
As part of our editorial theme for 2020, “Critical Issues Facing the Profession,” we asked Dr. Ann Eshenaur Spolarich, to comment on the challenges we face in applying evidence-based research to clinical practice. Professor Spolarich is the Director of Research, Arizona School of Dentistry and Oral Health, A.T. Still University. While the examples used in the editorial were not drawn from our current pandemic, the application of current research findings to patient care has become even more significant as we navigate the challenges that lie ahead. It is vital that all oral healthcare professionals learn and utilize evidence-based decision making throughout their professional careers.
I wish you all safety and good health always…but especially during this challenging time!
Rebecca S. Wilder, RDH, MS
Editor-in-Chief, Journal of Dental Hygiene
- Copyright © 2020 The American Dental Hygienists’ Association





{kind=link}
{kind=link}