



Abstract
Purpose: The purpose of this study was to determine strength of muscles involved with instrumentation (scaling) by dental hygienists and the additive effects of cellular (mobile) phone usage, as indicated by measurements of muscular force generation.
Methods: A convenience sample of licensed dental hygienists currently in clinical practice (n=16) and an equal number of individuals not currently using devices/tools repetitively for work (n=16), agreed to participate in this pilot study. All participants completed a modified cell phone usage questionnaire to determine their use pattern and frequency. Upon completion of the questionnaire, participants' force production in six muscle groups was measured using a hand-held dynamometer. Descriptive statistics were used to analyze the data.
Results: A total of 16 licensed dental hygienists (n=16) and 16 participants with no history of using tools/devices repetitively for work (n=16), comprised the experimental and control groups, repectively. The control group generated greater muscle force than the experimental group for the abductor pollicis longus (p=0.045). Significant differences were identified when comparing the low mobile phone users in the experimental group to the control group for the flexor pollicis brevis (p=0.031), abductor pollicis longus (p=0.031), and flexor digitorum (p=0.006), with the control group demonstrating higher muscle force. Years in clinical practice and mobile phone use was shown to have a significant effect on muscular force generation for the flexor pollicis brevis (F=3.645, df=3, p=0.020) and flexor digitorum (F=3.560, df=3, p=0.022); subjects who practiced dental hygiene the longest produced the least amount of muscle force.
Conclusion: Results from this pilot study indicate there are no significant additive effects of cell phone use and dental hygiene practice on finger muscles used for instrumentation. However, results indicate that dental hygiene practice demonstrated significant effects on muscular strength as compared to individuals who do not use tools/devices repetitively for work. The small sample size may have impacted results and the study should be repeated with a larger sample.
Introduction
Musculoskeletal disorders (MSDs), injuries to muscles, bones, joints, and their associated ligament and tendon attachments, have been identified as an occupational risk factor for dental hygienists.1 There are two classifications of MSDs based on the etiology and duration of the disorder; acute MSDs (i.e. an injury associated with a traumatic event), and chronic MSDs (i.e. an injury that develops over time and is persistent).1 A high incidence of work-related, chronic MSDs in dental professionals have been attributed to the repetitive motions associated with instrumentation in clinical practice.1-11 These repetitive motions place strain on the musculoskeletal system that can lead to pain in the affected areas known as cumulative trauma disorders (CTDs).1-4 Dental hygienists use instruments throughout the day requiring precise movements of the thumb and index fingers during scaling and polishing procdures.7 On average, a dental hygienist spends about 70% of their work-week performing repetitive finger and hand motions that can lead to CTDs.8 In addition, reports have shown dental professionals hold their fingers and hands in positions outside of neutral for long periods of time, further increasing the risk for CTDs.7 Development of CTDs contribute to early retirement, reduced income and productivity, increased medical care costs, and decreased overall health in dental hygienists.1-13 While extensive research has been conducted to examine potential strategies to reduce the effects of CTDs in dental hygiene practice,7,14-21 little is known about the additive effects of repetitive tasks outside of the workplace.
Cell or mobile phone use has increased worldwide, especially among younger individuals over the last two decades.22 The use of cell phones for texting, scrolling, gaming, and various applications leads to repetitive motions similar to those found with scaling and root debridement by dental hygienists.22-30 Observed conditions resulting from cell phone use include pain and inflammation of the fingers, hands, wrists, and forearm muscles, tendons, and surrounding ligaments.22-30 Previous studies have reported on the presence of CTDs in individuals using cell phones frequently with the extent of the disorder dependent on the pattern of usage.22 Texting has been linked to detrimental muscular effects especially in the thumb resulting in pain, De Quervian repetitive strain injury, stenosing tenosynovitis, and other inflammatory conditions and/or disorders.23-27,29 With the increased susceptibility to overuse injuries of the thumb and fingers due to texting, it is important to explore the risk for developing CTDs in dental hygiene clinicians who frequently use a cell phone for text communications. Assessment of the additive effects of repetitive cell phone use and dental hygiene practice have not been reported in the literature. The purpose of this novel, experimental, pilot study was to determine the muscular strength of the muscles involved with scaling and root debridement by dental hygienists in clinical practice, as well as the additive effects of cell phone usage on those muscles, as indicated by muscular force generation.
Methods
A convenience sample of licensed dental hygienists, currently in clinical practice (n=16), and an equal number of individuals not currently using devices/tools repetitively for work (n=16), agreed to participate in this this IRB-approved (Old Dominion University IRB 18-192) pilot study. Power statistics indicated a minimum of 16 subjects per group were needed to achieve a 95% confidence interval and a 95% power.31 The inclusion criteria for the experimental group of the study were right-hand dominant, licensed dental hygienists working in clinical practice, and ownership of a a smartphone mobile device. Inclusion criteria for the control group were that the participants were right-hand dominant, not dental hygienists, did not use tools/devices repetitively for work, and owned a smartphone mobile device.
Following informed consent, participants were asked to complete a modified Cell Phone Usage Questionnaire (CUQ) prior to muscle force measurements. The questionnaire provided information with regards to the types of tasks performed with a cell phone as well as perceptions on the average amount of time these tasks were performed each day.32 The modified CUQ utilized six questions pertaining to e-mail, Internet browser, mobile games, and application use on smartphone devices each day. Additionally, the survey had two items identifying cell phone use while using the fingers, hands, wrists, and/or forearms for other tasks simultaneously, such as texting and driving. Questionnaire items were rated on a 6-point Likert scale with 1 being “never” and 6 being “constantly.” Total scores on the modified CUQ ranged from 6-36. Low cell phone use was identified as scores within the range of 6-16, moderate cell phone use ranging from 16.1-26, and high cell phone use ranging from 26.1-36. The modified CUQ also included demographic questions related to gender, age, race, and years in dental hygiene practice (experimental group).
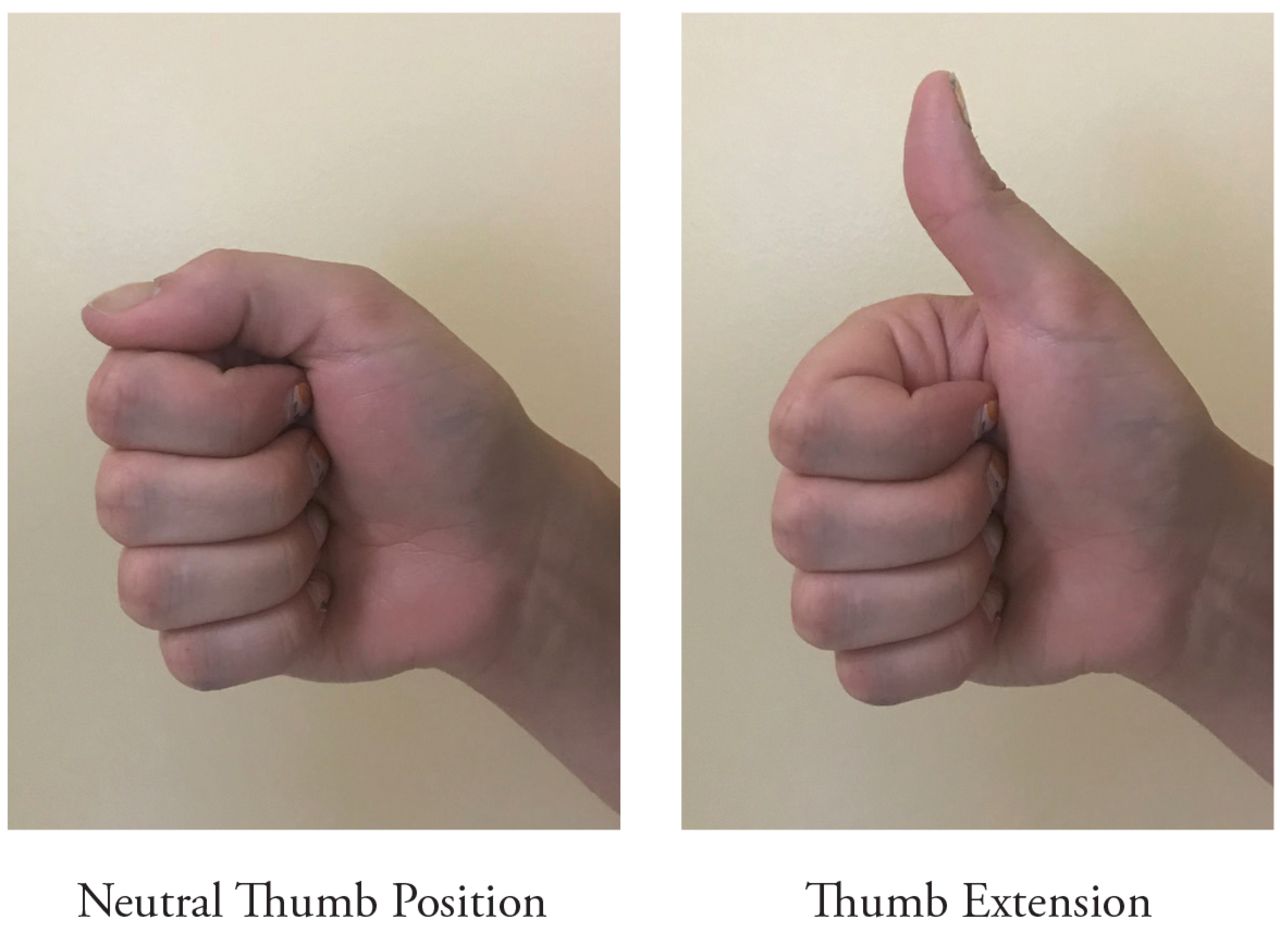
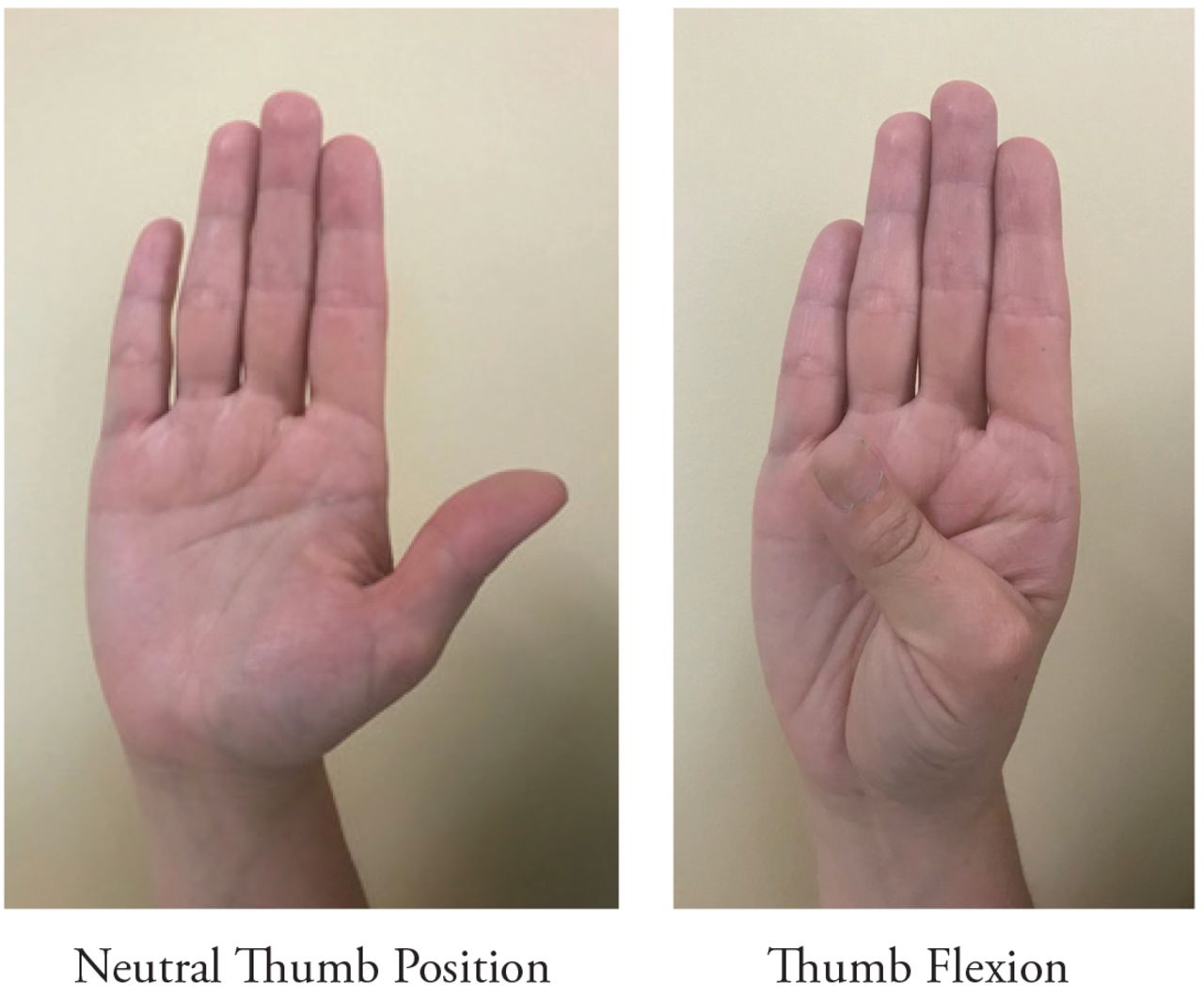
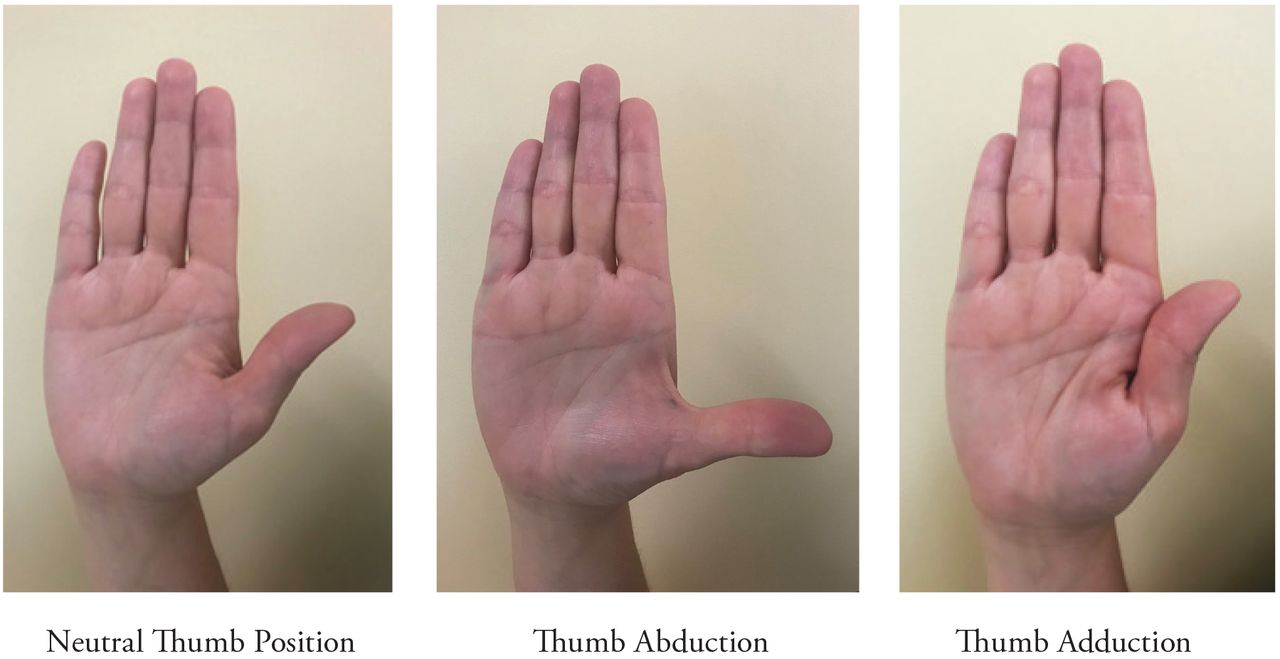
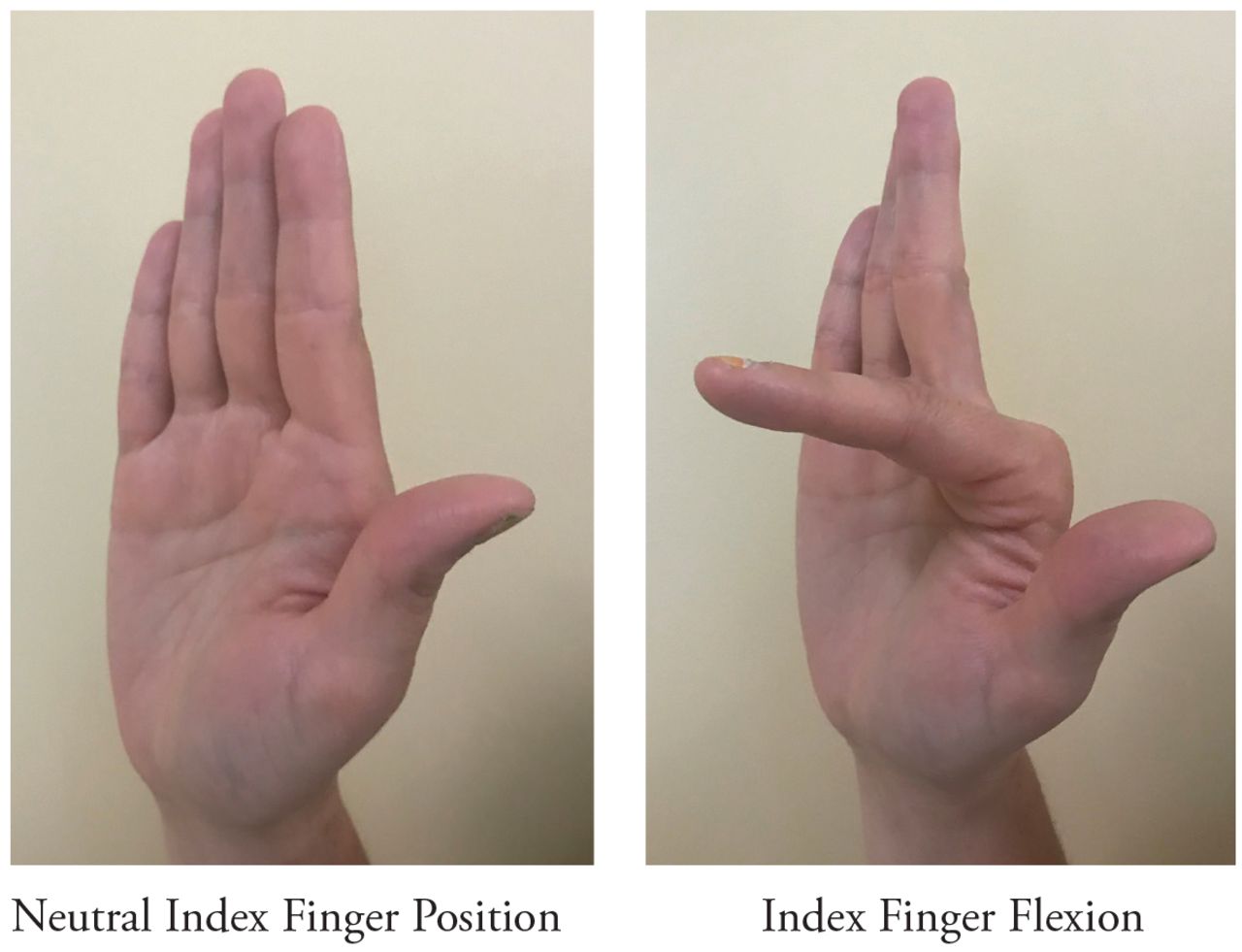
After completing the modified CUQ, participants performed a series of tests that measuring force production of muscles identified as being associated with cell phone use as well as dental hygiene practice (Table I, Figures 1, 2, 3 and 4). A MicroFET 2 hand-held dynamometer (Hoggan Industries, Inc., UT, USA), a valid instrument for measuring muscular force production, was used to test each muscle group. Following an explanation and demonstration of the measurement process, each participant was asked to push against the dynamometer as possible for a total of three seconds (Figure 5). Each muscle of the dominant (right) hand was tested individually three times with a minute of rest between each trial. The average amount of force produced for the individual muscles was used to determine differences between the experimental (dental hygienist) and the control group. Data on self-reported cell phone use collected with the modified CUQ was also used to identify differences in muscle strength between the identified low, moderate, and high cell phone users in both groups, as well as among dental hygienists individually. The effects in muscle force production based on years in dental hygiene practice was also evaluated.
Data analysis
Independent samples t-tests were used to assess differences in force between the experimental and control groups for each individual muscle. One-way ANOVA was utilized to compare mean muscle force generation for the experimental and control groups, based on three levels of cell phone use: low, moderate, and high. If the results were significant, a Bonferroni post hoc test was used to evaluate the differences between the six groups. To address the effect of years in practice for dental hygienists and cell phone use on muscular force generation, a one-way ANOVA test was used. If the results were significant, a Bonferroni post hoc test was used to evaluate the differences between years in practice. Statistical analyses were performed using SPSS statistical software, version 24 (IBM, Armonk, NY) with the significance level set to p<0.05.
Muscles evaluated for force generation with the force transducer*


Results
A total of 16 licensed dental hygienists and 16 participants with no history of using tools/devices repetitively for work, comprised the experimental and control groups, respectively. Equal numbers of males (n=3) and females (n=13) participated in each group. This distribution was intentional in order to ensure accurate averaging of force measurement results. The majority of participants were female (81.25%, both groups) and between the ages of 18-44 (81.25%, experimental group and 87.5%, control group). Participants in the experimental group had varying levels of experience in clinical practice with the majority practicing for ten years or less. Participant demographics are shown in Table II.

A total of three measurements were taken per participant for each individual muscle group, resulting in a total of 288 readings per group and 576 readings overall. Muscle strengths were compared between the experimental and control groups to determine differences between in muscle forces between the experimental and control groups. Independent samples t-test revealed statistically significant differences between the experimental and control group for the abductor pollicis longus (p=0.045), indicating the mean muscle force generated was greater for the control group. The average muscle force generation for each muscle tested is shown in Table III.

Handheld dynamometer for measuring muscle force production
Participant demographics
The experimental group and control groups were broken up into low, moderate, and high cell phone user groups. To identify the effects of cell phone use and dental hygiene practice on overall finger muscle force, one-way ANOVA was used to determine statistically significant differences between the groups. Means and standard deviations for the amount of force generated for each of the muscles were determined for each group of cell phone users are shown in Table IV. Significant differences were found when comparing low cell phone users in both the experimental and control groups for the following muscles: flexor pollicis brevis (p=0.031), abductor pollicis longus (p=0.031), and flexor digitorum (p=0.006). For these muscles, the control group had higher muscle force generation when compared to the experimental group. For moderate and high cell phone users, while the control group generated more muscle force, the results were not significant.
Descriptive statistics for muscle force generation
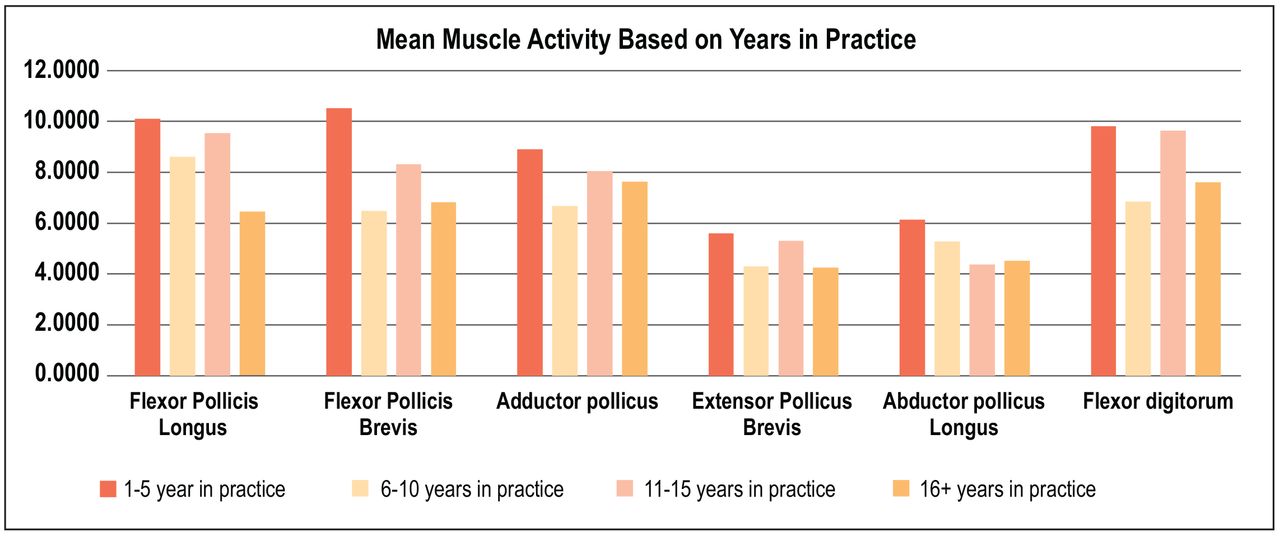
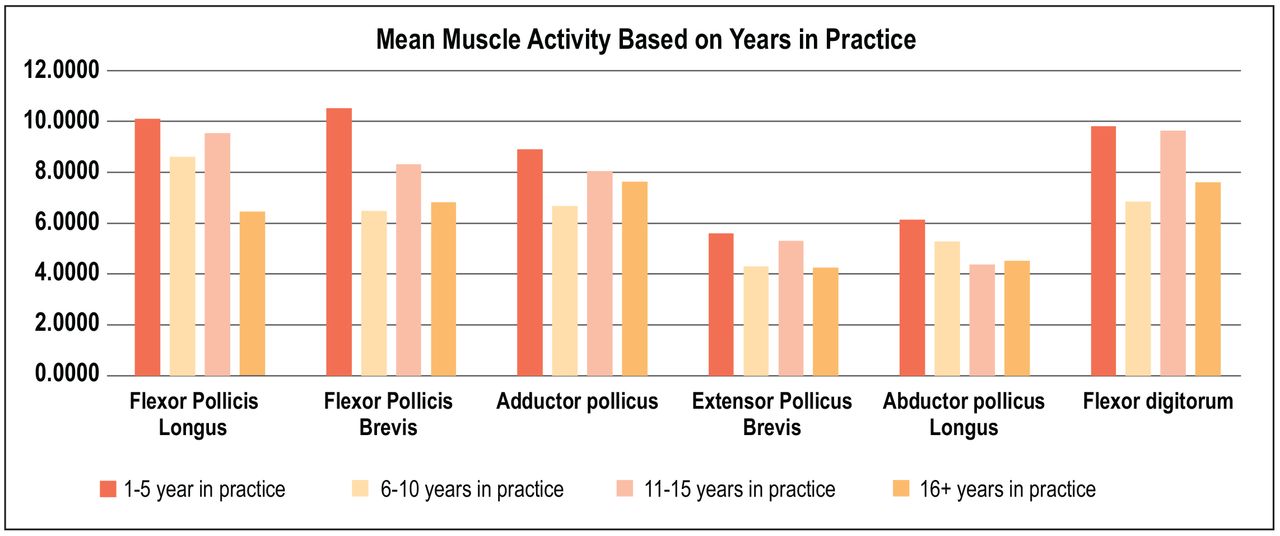
Muscle force generation and cell phone use was compared for each individual muscle based on years in clinical practice in the experimental group (Figure 6). The results of the one-way ANOVA test indicated a significant effect related to years in practice for the flexor pollicis brevis (F=3.645, df=3, p=0.020) and flexor digitorum (F=3.560, df=3, p=0.022) muscles; with with subjects who had practiced the longest producing the least amount of muscle force. Post hoc tests showed that participants practicing 1-5 years produced significantly higher muscle force for the flexor pollicis brevis as compared to those practicing 6-10 years (x=10.53 and x=6.48, respectively; p=0.028). Additionally, post hoc tests indicated participants practicing 1-5 years produced significantly higher muscle force for the flexor digitorum as compared to participants practicing 6-10 years (x=9.82 and x=6.85, respectively; p=0.026). No other statistically significant differences were identified in muscle force generation based on years in practice for the individual muscles examined.
Mean and standard deviations for muscular force generation
Means for muscular force generation and years in clinical practice
Discussion
Cumulative trauma disorders are common injuries found among dental hygienists as well as among individuals identified as high cell phone users.1-12, 20-29 Quantifying the additive effects of cell phone use and dental hygiene practice on force production may aid dental hygienists in identifying risk factors associated with CTDs. This pilot study aimed to compare dental hygienists with a comparable control group to determine the effects of cell phone use on muscle force generation for several muscles used in dental hygiene practice for instrumentation. This study also compared the additive effects of cell phone use and dental hygiene practice on the strength of these muscles, in addition to the effects based on years of clinical practice.
The results indicate that dental hygiene practice had a significant effect on muscle force generation as compared to the control group. The control group had significantly higher mean muscle force at the abductor pollicis longus, which aids the thumb in side-to-side movement, indicating that dental hygienists have reduced abductor pollicis longus strength as compared to individuals who do not use tools/devices repetitively for work. The use of dental instruments has been demonstrated to increase muscle activity in the forearm and wrist.9,14-16,20-21 It is possible that the repetitive motions specifically at the abductor pollicis longus in clinical practice has a negative effect on the force produced on this muscle. Future research should determine whether there are preventative measures aimed at reducing the impact of dental hygienist work factors contributing to this reduced strength. The average dental hygienist in clinical practice, spends roughly 22 hours a week performing repetitive tasks with instruments and devices (i.e. scaling and polishing), and a high prevalence of CTDs amongst this population is not surpising.8
Results of this pilot study reveal dental hygienists who are categorized as low cell phone users produced significantly less muscle force than low cell phone users in the control group. However, no other statistically significant differences were found between the experimental and control group as cell phone use increased to moderate and high levels. These results indicate there may not be any additive effects of cell phone use on specific muscle strength, rather clinical dental hygiene practice (i.e. scaling and polishing) effects muscle strength. Low cell phone users are not using their devices repetitively for the long durations as seen with moderate and high cell phone users, indicating that the differences noted may be due to dental hygiene practice rather than cell phone use.
Results from this pilot study also suggest years in clinical practice for dental hygienists may also negatively impact the muscular force generated in the thumb and index finger. There is a natural degeneration of overall musculoskeletal strength with over time.32-34 Age, in combination with the muscular stress placed on clinicians over years of practice, may play a large role in comorbidities related to the dental hygiene profession. Clinicians in practice for five years or less generated higher muscular forces for each of the muscles tested and significantly more for the flexor pollicis brevis and flexor digitorum when compared to clinicians practicing for 6-10 years, indicating years in clinical practice requiring repetitive motions may reduce the muscular force generated for muscles. Dental hygienists who have been practicing longer periods of time may need to be cautious of additional repetitive behaviors and activities of longer duration of the fingers, hands and wrists, such as cell phone use.
Previous studies have indicated that the repetitive motions of dental hygiene practice impact the wrist and hand muscles and risk for developing CTDs.1-20 Additional studies outside of dentistry have indicated that the repetitive motions of cell phone use can also lead to disorders in the fingers, hands, wrists, and forearms.20-28 However, there is a gap in the literature regarding the additive effects of these two repetitive practices and how they may be quantified in muscle force produced by individual muscles. Findings from this study indicate that cell phone use does not have an additive effect on muscle strength production for dental hygienists. However, these findings reinforce the need for awareness of the repetitive motions of dental hygiene practice and how they may impact the risk for developing CTDs and career longevity. This is especially noteworthy given that average muscle force generation was reduced in participants after five years in clinical practice. Further research should be conducted with larger samples to better quantify the effects of repetitive cell phone use and dental hygiene practice, by further examining muscle activity production in regards to specific tasks associated with cell phone use with the addition of the muscles in the wrist and forearm used for clinical dental hygiene. Studies should also examine other repetitive practices that may have additive effects on muscles (e.g. playing the piano and e-gaming) and risk for CTDs. Results from this pilot study could impact dental hygienists by increasing awareness among dental hygiene educators, future and current clinicians of the risk factors associated with all types of repetitive practices and CTDs.
This pilot study had several limitations. The small, convenience sample may have impacted the results and limited the generalizability of findings. Cell phone use was determined by self-reporting questionnaires and may inaccurately represented the amount of time participants actually used cell phones for repetitive tasks and the exact duration of cell phone use per day was not determined for each participant. Additionally, information on other extracurricular activities that may impact muscular strength produced by the muscle groups studied was not collected and may have impacted the muscle force generation measurements. The type and size of the cell phone used may have impacted the effects on muscular strength produced as well. Future studies are needed to look at the type and size of cell phones used, the exact daily duration of use, and ways to reduce the risk of the additive effects on development of musculoskeletal disorders. Additionally, future research should evaluate muscle activity generation with the use of surface electromyography to determine the additive effects of cell phone use and dental hygiene practice on the forearm and wrist muscles that are used for both activities. Muscles in the wrist and forearm have been identified for repetitive motions in dental hygiene practice and may also be used for cell phone activities as well.13-15, 20-21
Conclusion
Results from this pilot study indicate there are no significant additive effects of cell phone use and dental hygiene practice on finger muscles used for instrumentation. However, results indicate that dental hygiene practice had significant effects on muscular strength as compared to individuals who do not use tools/devices repetitively for work. These results suggest dental hygiene practice impacts muscular force generation and risk for developing CTDs. Future research should be conducted to examine these effects and ways to reduce overall risk for CTDs in larger samples of dental hygienists, as well as the additive effects of prolonged, repetitive tasks performed outside the workplace.
Footnotes
Jessica R. Suedbeck, RDH, MSDH is an assistant professor in the School of Dental Hygiene, Old Dominion University, Norfolk, VA; Cortney N. Armitano-Lago, PhD, LAT, ATC is a postdoctoral research associate in the Department of Exercise and Sport Science, the University of North Carolina, Chapel Hill, NC; Emily A. Ludwig, RDH, MSDH is a visiting lecturer in the School of Dental Hygiene, Old Dominion University, Norfolk, VA.
This manuscript supports the NDHRA priority area, Professional development: Occupational health (determination and assessment of risks).
- Received April 19, 2019.
- Accepted September 29, 2019.
- Copyright © 2020 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}