



Introduction
Tobacco is the only legal consumer product that kills at least 1 out of 2 of its regular users when used as intended by the manufacturer.1 There are approximately 1.1 billion smokers world-wide, and it is predicted that the use of tobacco could kill 1 billion people during the 21st century. Cigarettes contain tobacco, and tobacco contains nicotine, delivered rapidly to the brain when smoking tobacco. Nicotine is a single psychoactive substance that affects the brain and the central nervous system, among others. The disease of tobacco addiction (Nicotine Dependence, Tobacco Use Disorder) is recognized as a chronic disease by most authorities including the USDHHS, Health Canada, the many countries' Medical Associations, and the World Health Organization; it is classified as such in major disease classification systems.2,3 However, not every person who uses tobacco is addicted to nicotine.
Addiction is a Pediatric Disease
Tobacco addiction is a treatable disease and not simply a lifestyle choice. Addiction is a primary, chronic, neurobiological disease with genetic, psychosocial, and environmental factors influencing its development and manifestations. It is characterized by behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving.3 This condition is typically induced by repeated exposure to nicotine from tobacco, producing changes in the brain's motivational system as a consequence of which a reward-seeking behavior has become out of control.4,5 Decision-making and behavior are subsequently influenced by the underlying pathophysiological changes in the brain. Ninety percent of the population will try tobacco at least once in their lifetime, and about 90% of persons who become addicted will do so before the age of 18.
Global Approaches to Tobacco Control
Although much progress has been made in many countries, our current country-specific prevalence rates cannot be seen as the endpoint for success. Increasing adult cessation is considered a major determinant for reducing smoking-related death and disease over the next few decades.6 The first international public health treaty—the Framework Convention on Tobacco Control (FCTC)7 — represents a milestone for public health. Article 14 of the FCTC addresses cessation. In its MPOWER initiative, the WHO describes the six key policy strategies that have been demonstrated to denormalize and reduce tobacco use:1
M: Monitor tobacco use and prevention policies
P: Protect people from tobacco smoke
O: Offer help to quit tobacco use
W: Warn about the dangers of tobacco
E: Enforce bans on tobacco advertising, promotion and sponsorship
R: Raise taxes on tobacco
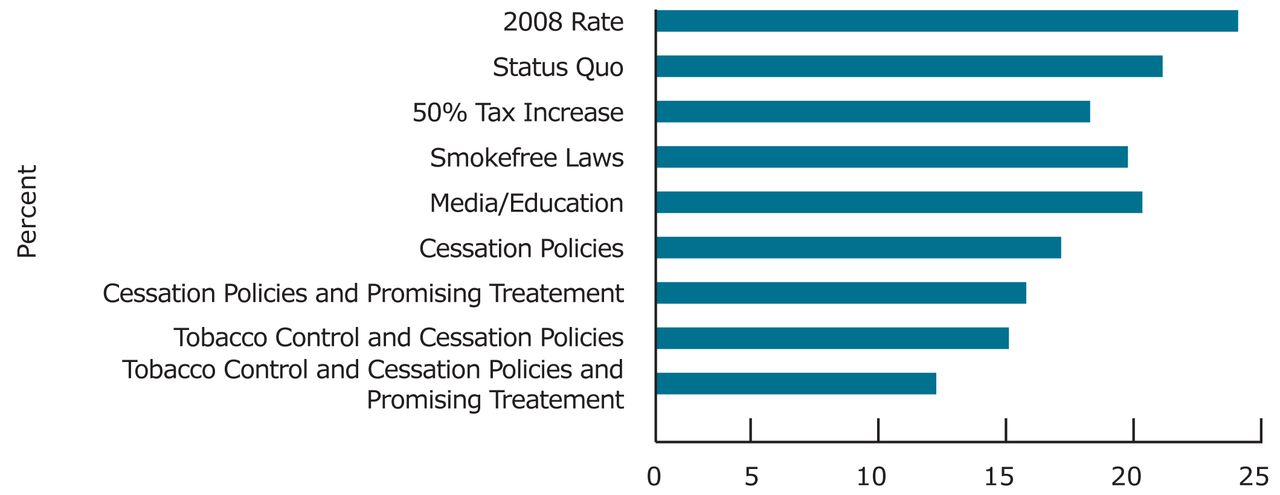
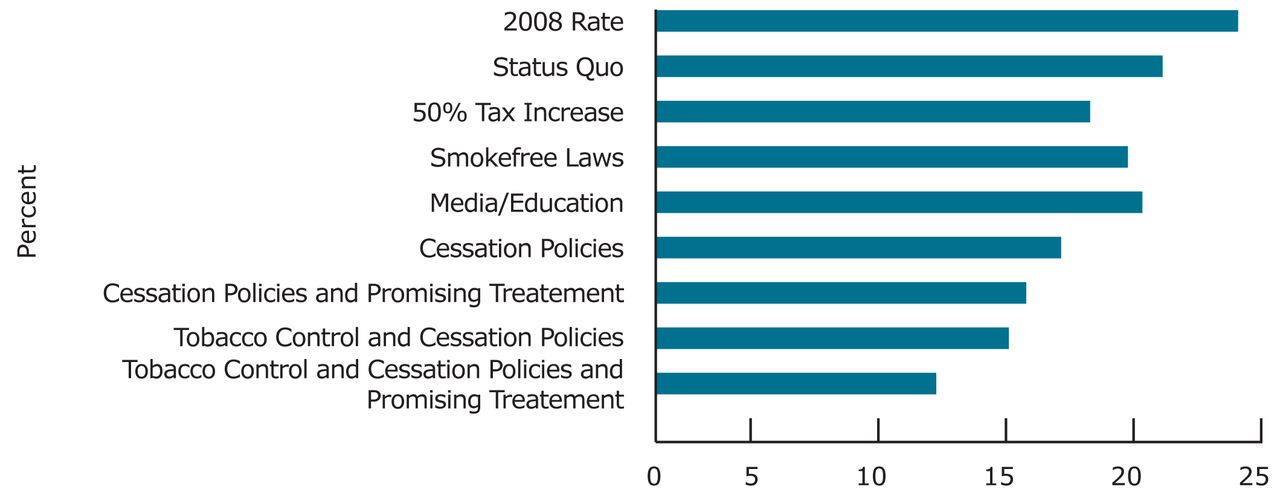
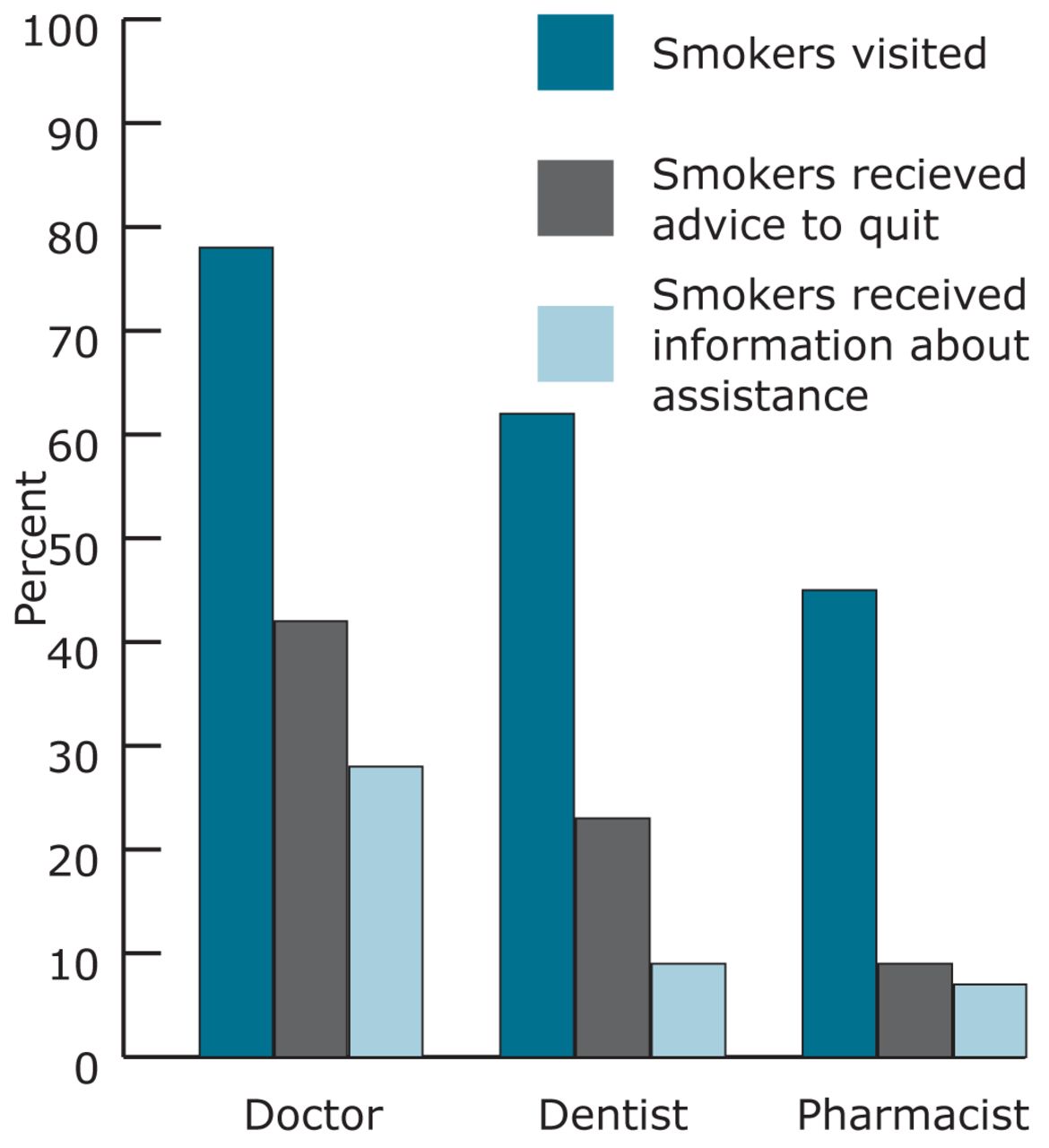
Simulation models8 examine the overall effect of tobacco control policies and other interventions on estimated population quit rates. Graph 1 demonstrates some of the lost opportunities for cessation interventions on primary care for different disciplines.
Despite the devastating health effects and the associated costs to society, and the availability of safe and effective measures to treat tobacco addiction, there appears to have emerged a plateau in tobacco control's impact. There are numerous plausible explanations for this, including lost opportunities for safe and effective interventions by health professionals. The reality is that, despite the proven beneficial impact on remedying the tobacco epidemic, treatment of tobacco use and addiction continue to be vastly neglected.9
Treatment Approaches
There is a robust body of evidence guiding effective tobacco cessation, and there exists a wide array of internationally recognized guidelines and opportunities for intervention with tobacco use and addiction. The US Public Health Service-sponsored Clinical Practice Guideline update identifies the ‘5-A’ model for treating tobacco use and dependence.9 This includes asking about tobacco use with every patient at every visit, advising tobacco users to quit, assessing willingness to make a quit attempt, assisting those willing to attempt quitting by offering counseling and medication, by motivating future quit attempts in those unwilling, and arranging for follow-up contacts.
USDHHS Guideline Key Recommendations for Tobacco Use and Dependence9
The overarching goal of these recommendations is that clinicians strongly recommend the use of effective tobacco dependence counseling and medication treatments to their patients who use tobacco, and that health systems, insurers, and purchasers assist clinicians in making such effective treatments available.
Tobacco dependence is a chronic disease that often requires repeated intervention and multiple attempts to quit. Effective treatments exist, however, that can significantly increase rates of long-term abstinence.
It is essential that clinicians and healthcare delivery systems consistently identify and document tobacco use status and treat every tobacco user seen in a healthcare setting.
Tobacco dependence treatments are effective across a broad range of populations. Clinicians should encourage every patient willing to make a quit attempt to use the counseling treatments and medications recommended in the Guideline.
Brief tobacco dependence treatment is effective. Clinicians should offer every patient who uses tobacco at least the brief treatments shown to be effective in the Guideline.
Individual, group, and telephone counseling are effective, and their effectiveness increases with treatment intensity. Two components of counseling are especially effective, and clinicians should use these when counseling patients making a quit attempt:
Practical counseling (problem-solving/skills training)
Social support delivered as a part of treatment
Numerous effective medications are available for tobacco dependence, and clinicians should encourage their use by all patients attempting to quit smoking—except when medically contraindicated or with specific populations for which there is insufficient evidence of effectiveness (i.e. pregnant women, smokeless tobacco users, light smokers, and adolescents).
Seven first-line medications (5 nicotine and 2 non-nicotine) reliably increase long-term smoking abstinence rates:
bupropion (Sustained Release [SR])
nicotine gum
nicotine inhaler
nicotine lozenge
nicotine spray
nicotine patch
varenicline
Clinicians should consider the use of certain combinations of medications identified as effective in the Guideline.
Counseling and medication are effective when used by themselves for treating tobacco dependence. The combination of counseling and medication, however, is more effective than either alone. Thus, clinicians should encourage all individuals making a quit attempt to use both counseling and medication.
Telephone quitline counseling is effective with diverse populations and has broad reach. Therefore, both clinicians and healthcare delivery systems should ensure patient access to quitlines and promote quitline use.
If a tobacco user currently is unwilling to make a quit attempt, clinicians should use the motivational treatments shown in the Guideline to be effective in increasing future quit attempts.
Tobacco dependence treatments are both clinically effective and highly cost-effective relative to interventions for other clinical disorders. Providing coverage for these treatments increases quit rates. Insurers and purchasers should ensure that all insurance plans include the counseling and medication identified as effective in the Guideline as covered benefits.
Consistent with the FCTC Article 14,7 Canada released its first federally funded set of Clinical Practice Guidelines through the Canadian Action Network for the Advancement, Dissemination and Adoption of Practice-informed Tobacco Treatment (CAN-ADAPTT).11 Given the high level of co-occurrence of mood symptoms in persons who use tobacco and/or stop its use, the basic algorithm included in CAN-ADAPTT allows integrated and brief screening of mood in the treatment of tobacco use and addiction.
Among those who currently smoke tobacco, approximately 70% would like to stop and about half of these will try to quit at least once this year.10 The use of short-term, acute care models to manage chronic, non-communicable diseases is theoretically inconsistent. Hypertension, hypercholesterolemia, obesity, diabetes, depression, chronic obstructive lung diseases and addiction are some diseases that often require repeated interventions. Following a short-term approach for tobacco-addicted individuals is equally illogical and compromises the chances of long-term cessation success. Evidence-based smoking cessation is both safe and effective and appears to be one of the most robust and clinically meaningful interventions healthcare professionals could offer.

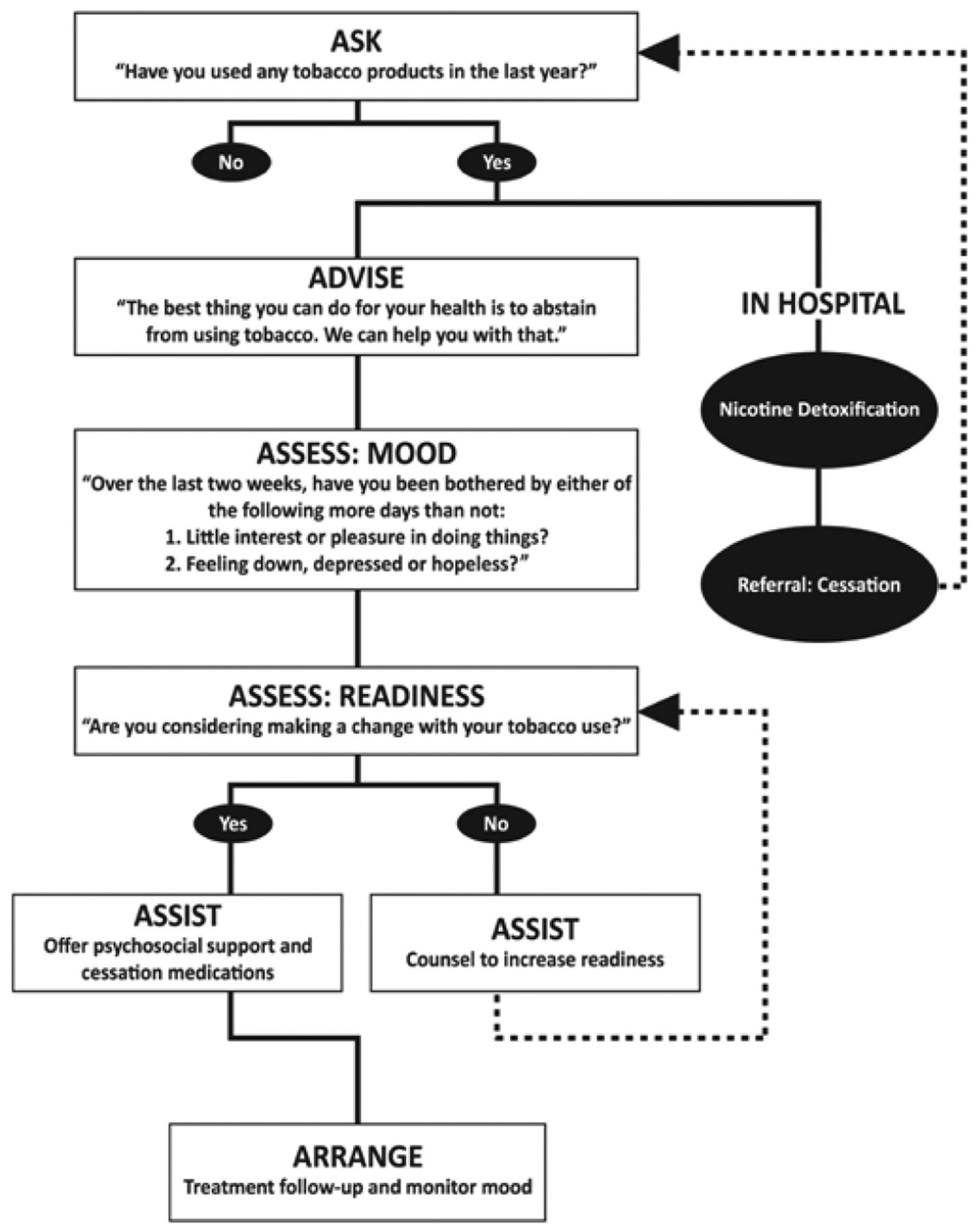
Safety Sensitive Algorithm
Conclusion
Tobacco use remains the leading preventable cause of death and disease worldwide and, having taken into consideration impressive progress over decades, existing smoking rates (as an endpoint) cannot be regarded as a success. Yet the problem of tobacco does not have to be an intractable one. It has been estimated that some of the greatest declines in smoking-related death over the next few decades will come from increasing adult cessation. Tobacco (nicotine) addiction is a chronic disease amenable to treatment. Health professionals are ideally placed to make a substantial difference, utilizing Clinical Practice Guidelines.12 Despite the highly significant health threat of tobacco, the existence of robust interventions, and the desire of most individuals to quit, opportunities continue to be neglected. Evidence tells a vivid and chilling story of the dire and urgent need to support cessation.12
- Copyright © 2015 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}