



Abstract
Purpose: Frail elders and nursing home residents are vulnerable to poor oral health and frequently lack access to dental care. The purpose of this study was to determine why residents in Arkansas skilled nursing facilities have limited access to oral health care.
Methods: This study utilized qualitative research methodology. Data was collected from oral health care personnel through open-ended responses in a written survey (n=23) and through telephone interviews (n=21). The investigators applied the constant comparative method to analyze and unitize the data and ultimately reach consensus.
Results: Data analysis resulted in consensus on 2 emergent themes: policy and access.
Conclusion: This qualitative case study suggests access to oral health care for residents living in both long-term care (LTC) and assisted living I and II facilities in Arkansas is affected by public and facility policies and access to oral health care as a function of the patient's health status and availability of oral health care providers. Access for residents residing in assisted living I and II facilities is also limited by the residents' inability to assume responsibility for accessing oral health care. The outcomes from this study may serve to inform policymakers and advocates for access to oral health care as they develop new policies to address this growing need.
Introduction
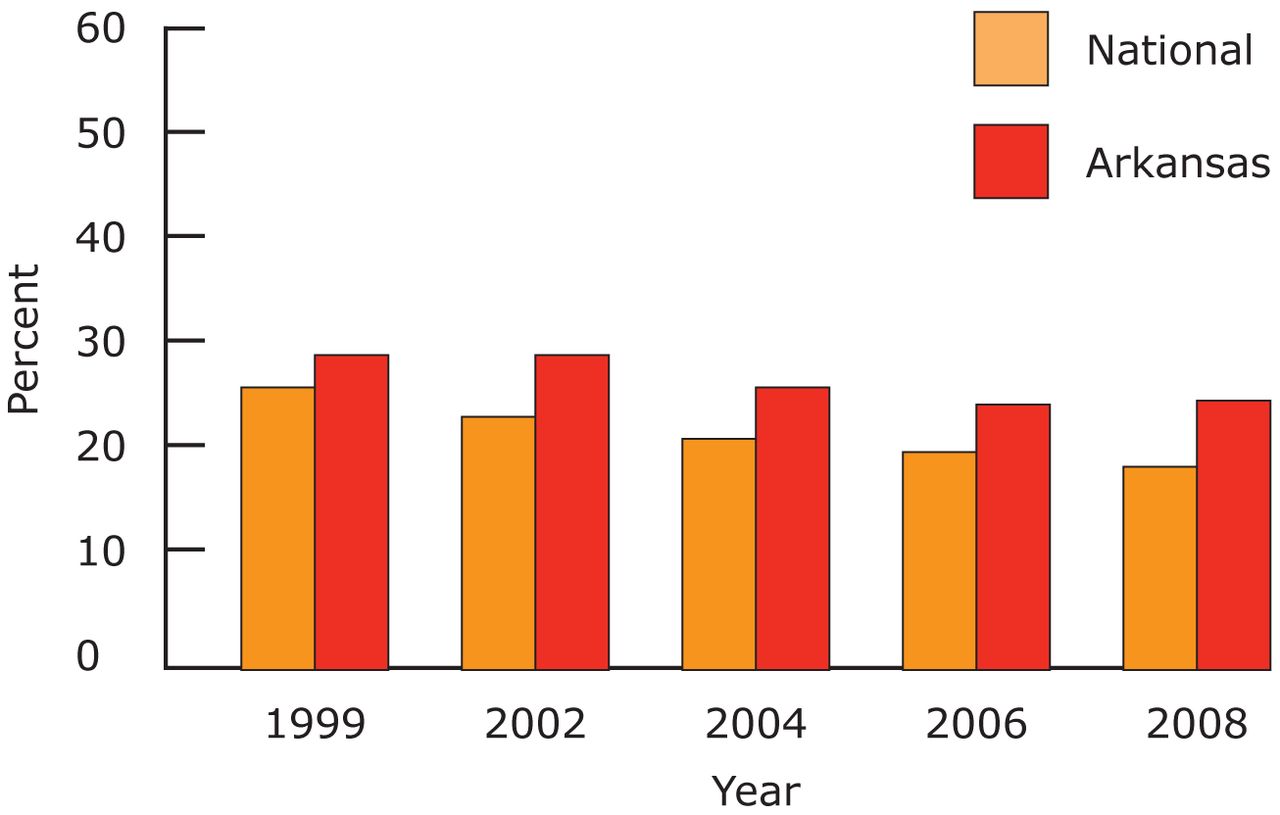
Older adults are the fastest growing population segment in the U.S. according to the 2010 U.S. census.1 Data from the Center for Disease Control (CDC) National Health and Nutrition Examination Survey (NHANES) indicate older adults in the U.S. are living longer and experiencing a significant decline in edentulism resulting in more teeth being exposed to dental disease.2 National and Arkansas statistics related to declining tooth loss are illustrated in Figure 1.3
Retention of teeth throughout the lifespan is desirable; however, dental care and maintenance become more complex and present additional challenges in long-term care (LTC) and assisted living facilities.4,5 Nursing facilities are defined by the level of care they provide. The highest level of care is provided through skilled nursing facilities referred to as LTC. Assisted Living facilities encompass any facility that provides personal care services to three or more adult residents and include Levels I and II. Residents of Level I facilities do not have serious medical conditions while Level II facilities accept residents that meet the lowest level of care and must have a nurse on contract.6
The Surgeon General's Report identified frail elders and nursing home residents among the populations most vulnerable to poor dental care.7 Aging populations have fewer financial resources and often do not retain dental insurance upon retirement.8 Elderly individuals are faced with a variety of age related functional disabilities directly and indirectly affecting their oral health.9-16 A primary concern is the association between poor oral health and aspiration pneumonia. Aspiration pneumonia accounts for the majority of admissions to hospitals from nursing homes and is the leading cause of death in nursing home populations.15,16 Inadequate oral health and disability status are further related to poor oral health related quality of life, thus increasing the need for access to oral health care.15,17-21 Research clearly documents the inadequacy of oral care provided in LTC facilities.12-14,22-29
Improving oral health for older adults by reducing the incidence of untreated decay and periodontitis is among the health objectives outlined in Healthy People 2020.29 Arkansans are typically behind in oral health care status as evidenced by earning a grade of “F” on the Oral Health America Report Card.22 Screenings of residents in LTC facilities in Arkansas revealed that virtually all residents (99.9%) had a history of dental caries or periodontal disease.30
The state of Arkansas, through its 2011 Oral Health Plan, addressed this disparity by setting goals for increasing access to oral care and passing Senate Bill 42, creating a collaborative care permit program for dental hygienists.31 The main purpose of the legislative change was to alleviate oral health care disparities by expanding the scope of dental hygiene practice. Similar workforce models have been implemented in other states.32 The Arkansas collaborative care permit program can aid in helping to preserve the natural dentition of the elderly population and decrease dental morbidity of vulnerable elders living in LTC and assisted living facilities. Three key components of this population's oral health needs include: regular oral assessment, preventive oral hygiene care and provision of dental treatment.23
It is important to assess dental needs of residents in nursing facilities in an effort to better provide oral health care. The purpose of this study was to determine why residents in Arkansas skilled nursing facilities have limited access to oral health care.
Methods and Materials
Institutional review board research protocol was approved by the University of Missouri-Kansas City. This study used a qualitative research design with descriptive statistics. The study was initially designed to capture quantitative and qualitative data using a validated survey instrument that identified current issues in meeting oral health needs of nursing facility residents.28 A question delineating the type of facility (LTC or assisted living) and open ended questions about dental hygienists providing oral care were added to the survey. Paper copies of the survey and follow up postcards were mailed to oral health care personnel in Arkansas nursing facilities (n=311). The oral health care personnel were defined as the staff member most involved with oral health care in Arkansas nursing facilities and included Directors of Nursing, registered nurses, certified nursing assistants (CNA) and health and wellness coordinators. Administrators who received the initial survey and cover letter made this determination. The survey was also distributed electronically to all registered Arkansas Health Care Association members (n=306) in a weekly members' newsletter.
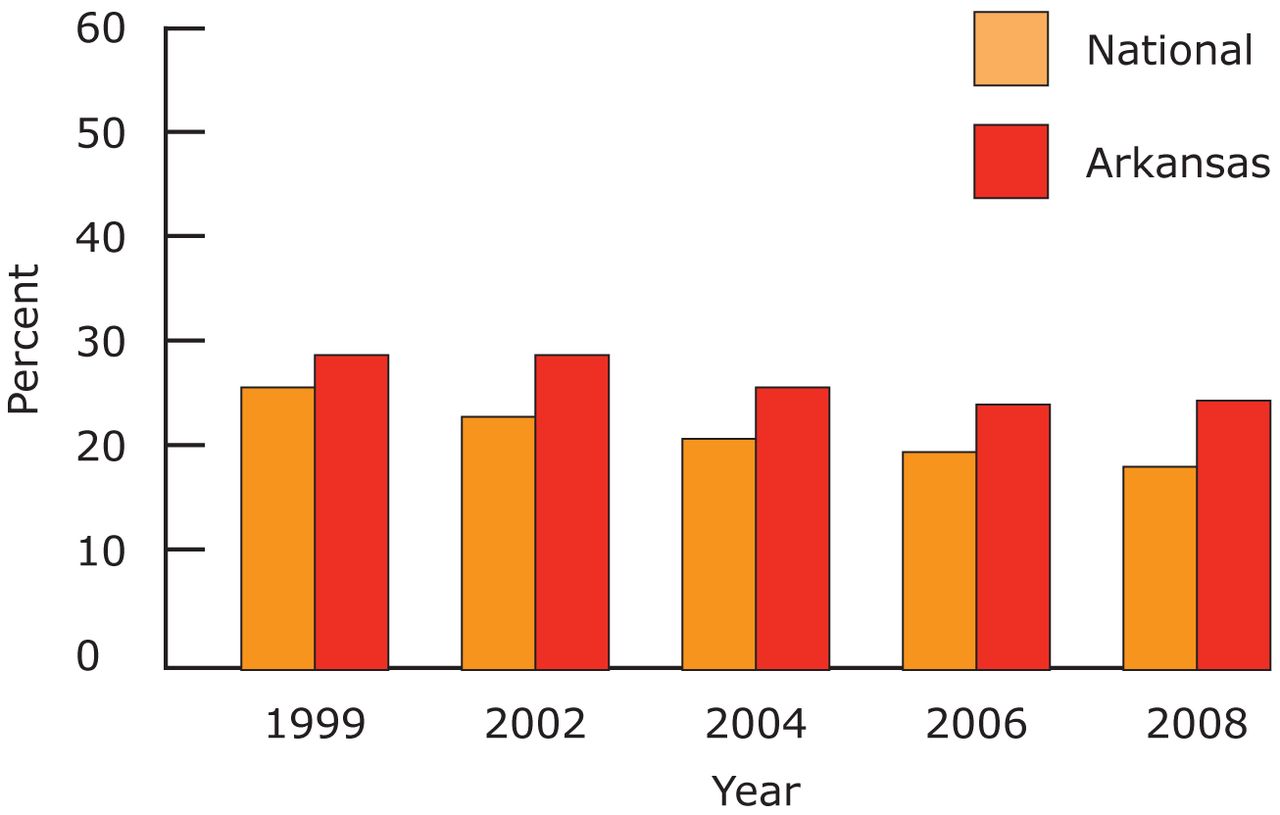
National/Arkansas Complete Tooth Loss, Adults Age 65 or Older Who Have Lost All Their Natural Teeth
Collectively, 23 surveys representing 14 counties were returned. The response rate was low (7.4%), so a quantitative analysis, as originally planned, was not implemented. Four researchers separately analyzed the open ended responses using the constant comparative methods described by Lincoln et al.33 Data was unitized by deconstructing the open responses and identifying key themes. Table I lists the descriptive and interpretive codes that were used. As themes emerged, the unitized data were reviewed and compared to reflect and describe specific themes.
In order to increase the response rate the primary investigator conducted telephone interviews with oral health care personnel working in facilities located in zip codes where the mailed surveys were not returned. A purposeful sampling strategy was used to target facilities (15 LTCs, 3 assisted living I and 3 assisted living II) for a combined total of 21 interviews. Facilities were located in 13 counties equally distributed across the state.
Unstructured, open-ended questions were asked to investigate why residents in Arkansas nursing facilities have limited access to oral health care. The primary investigator began each interview asking: “From your perspective, what are the greatest needs and barriers to providing oral care for residents of your facility?” Questions were asked until no new information emerged. The primary investigator took detailed notes to capture the essence of each conversation.33 Four investigators separately analyzed interview notes and reached consensus identifying key themes. Descriptive numerical frequencies were tracked and totaled within categories and calculated as an overall total percentage.
Several approaches were employed to establish validity and reliability of the findings as suggested and described by Creswell.34 Triangulation was achieved by collecting and analyzing data from 2 separate sources and by comparing the present findings with published literature. Between the 2 sources of information, 23 of Arkansas' 75 counties were represented. Using descriptions to convey findings providing a sense of shared experiences was accomplished by including original quotes in the results. Peer debriefing was used within the qualitative study for describing results for other care providers, government officials or families reviewing results to enhance accuracy.
Results
Table II summarizes the key themes that emerged from the survey's open-ended questions and interview responses. Collectively, 133 units of data were analyzed. The emergent themes included policy (77%) and access (23%). Policy was defined as the rules and regulations in place that direct the provision of health care in LTC and assisted living facilities. Access was defined as making oral health care available for both LTC and assisted living facilities.
Within the theme of policy, 4 representative interpretive codes emerged. The areas of particular interest include regulations (12%), education (12%), infrastructure (44%) and personnel (8%). A majority of oral health care personnel's expressed not having appropriate infrastructure (44%) for the provision of oral health care within their facilities. Oral health care personnel's discussed a lack of dental equipment, providers, money and time, all of which impacted the delivery of care.
The majority of facility oral health care personnel's reported not having space dedicated to oral health care. One oral health care personnel expressed: “Residents staying in a familiar environment might increase cooperation making it easier to provide care.” Another oral health care personnel commented about the lack of dental personnel (8%): “We need dentists who are willing to come do assessments on residents at the facility.” Additional comments included: “It would help if a familiar CNA or family member was involved during care.”
Emergent Category and Representative Interpretive and Descriptive Codes for Interview Analysis
Summary of Emergent Themes with Representative Interpretive Codes for Long Term Care and Assisted Living Facilities for Survey Open End Responses and Interview Responses
Residents within these facilities may be insured, uninsured or underinsured; thus all residents living in the same facility do not have the same financial resources. This variability requires the oral health care personnel to understand multiple plans and know how to navigate each system. Respondents stated: “Our mobile dental services cannot provide emergency care and only people on the ‘offset plan’ usually get services,” “Families cannot afford dental care” and “This is a rural area with lots of people with no money.” Thematically, these statements support issues associated with infrastructure (44%) and regulation (12%) practices.
An oral health care personnel with extensive experience described a demanding work environment: “There is a prevalence of OHCP (oral health care personnel) burnout especially in the for-profit setting. OHCP staff frequently work 14 hour days. Oral care is often sacrificed as it is not visible, providing OHCPs a shortcut to surviving the day.” The oral health care personnel further discusses current attempts by nursing homes to implement a culture change when she described: “This change is to focus not just on the elder, but on the elder caregiver; to promote relationships between elders and staff by promoting consistent assignments in which the CNA would work with the same person or group of elders.” This finding described the theme of lack of personnel (8%) and the importance of staff providing quality care for residents being served.
Throughout the interviews oral health care personnel's at assisted living facilities discussed the need for better oral health education among personnel: “Educating staff about oral care is not required as nursing staff is primarily responsible for taking medication to the resident and reminding them to take it,” and: “Oral care is not regulated but we do provide some in-service education related to oral care.” The amount of oral health education provided to staff ranged from none to occasional and was inconsistent between facilities. Thematically, issues associated with staff education (12%) and personnel (8%) have significant impacts on care provision.
Lack of finances was a commonly cited barrier for accessing care services. One oral health care personnel recalled a resident having to choose between accessing dental care and purchasing medication. The oral health care personnel reported: “He ‘chose his medicine.’” These statements supported the considerations thematically associated with infrastructure (44%).
Concerns regarding lack of regulations were significantly higher for assisted living facilities (31%) than for LTC facilities (4%). Survey responses and interviews with oral health care personnel in LTC facilities revealed concerns that facilities have too many regulations and too much red tape hindering provision of oral health care. Conversely, survey responses and interviews with oral health care personnel in assisted living facilities expressed difficulties because of the lack of regulations. Assisted living facilities are not regulated and therefore are not required to provide oral care assessments or treatment. “We do not have dental assessments. The resident is responsible for making dental appointments.” These statements support concerns thematically associated with regulations (31%).
Within the theme of access, 3 representative interpretive codes emerged: patient health status (8%), provision of care (11%) and residential responsibility (4%). The oral health care personnel at LTC facilities expressed access being impacted by patient health status (11%). This did not appear to be a concern for assisted living facilities (3%).
A number of oral health care personnel expressed challenges when working with patients who have dementia resulting in the following quotes: “They are uncooperative and don't understand what you are trying to do and may even think that the toothbrush feels funny.” Additional concerns were related to residents being unable to articulate their own needs due to cognitive impairment: “They are often uncooperative, without it being their own fault-they don't understand what you are trying to do for them.” Another described concern that an underlying dental problem could cause behavioral problems stating: “They cannot tell you where it hurts.” These comments address concerns thematically associated with patient health status (8%) and provision of care (11%).
Repeated concerns were expressed about weight loss as a result of the lack of access to oral health care: “Many of the residents have ill-fitting dentures that discourage proper eating and cause weight loss,” and: “It is important to improve oral care in order to avoid losing weight.” Another stated: “They (residents) just don't care about taking care of their teeth.” These comments support concerns thematically related to patient health status (8%) and provision of care (11%).
The oral health care personnel at assisted living facilities expressed access being impacted by residential responsibility (13%). This was not a concern for LTC facilities (0%). The following quote provides a rich description of this matter: “Either the family member or legal guardians make all decisions about their oral care and are responsible for making dental appointments.”
Both types of facilities expressed that access is influenced by the provision of care (LTC 13%, assisted living 8%). When asked whether or not the oral health care personnel would be receptive to having a dental hygienist serve as the primary oral care provider, oral health care personnel were generally supportive of this oral health care provider model. The following quote represents responses related to the provision of care and openness to dental hygienists having direct access to patients without direct supervision: “I see more residents than in the past with their natural teeth and could see the benefit of having a dental hygienist provide oral care.”
Discussion
Limitations
Limitations are inherent in qualitative research. The investigator in qualitative research is considered to be the survey instrument.35 Potential bias exists as the investigator's personal opinions and experiences are involved in the process. Researchers conferred that there could be overlapping codes within established categories. Limited sample size and possible geographic bias are acknowledged to be limitations of this study. Further, the variety of oral health care personnel could have provided inconsistencies. The opinion of a caretaker who has only worked in the environment for 2 weeks is not comparable to a registered nurse with 30 years of experience. The investigators of the present study attempted to control for these limitations by using well established qualitative research methods; nevertheless, findings cannot be generalized.34
Reaching the target population of this study was problematic. Similar experiences have historically been reported in other studies involving nursing facilities.28,36,37 Interviews with industry experts acknowledged that the nursing home staff population is hard to reach, citing a demanding work environment, lack of email access and high turnover rate. A report from an Arkansas researcher showed difficulty acquiring informed consent and difficulty accessing the Arkansas nursing home population in a recent study.38
Financial Needs and Barriers
Residents of LTC and assisted living facilities have a variety of public and private dental insurance plans. Oral health care personnel in the present study voiced difficulties leveraging the nuances of these plans. Often oral health care personnel do not have the knowledge and time to assist residents in using the resources that are available. It is unlikely that this will change in the near future. Dental care coverage prior to and following the implementation of the Affordable Care Act (ACA) is provided primarily for children. Provisions of the ACA exclude mandatory dental coverage for adults deferring provisions to states.39,40 In Arkansas, older adults covered by both Medicare and Medicaid are selectively provided dental care under “life threatening conditions” only (Office of Oral Health, personal communication, 2014).
As in similar studies, financial concerns of the resident or family were considered to be an important barrier for both LTC and assisted living facilities. Those depending upon Medicaid and Medicare assistance are limited and encounter a significant amount of paperwork to attain needed assistance, adding to the demands of nursing staff and families. This burden results in treatment delays, prolonged pain and suffering and overall reduced quality of life.15,19,20
Educational Needs and Barriers
The present study revealed oral health care personnel felt more oral health education would be beneficial. This finding mirrors conclusions made by the Institute of Medicine in the 2011 report “Improving Access to Oral Health Care for Vulnerable and Underserved Populations.”41 The literature is replete with studies detailing the low priority of oral health by non-dental health care professionals.41-45 In response to these shortcomings, the Committee on Oral Health Access to Services developed a core set of oral health competencies and curricula for non-dental health care professionals to improve their ability to promote oral health and disease prevention.41 A national initiative known as the Oral Health Nursing Education and Practice was established to address this concern.46,47 An important aim of this initiative is to use inter-professional teams across the health care system to improve oral care provisions. Nurses are on the front line with regard to providing oral health care. With adequate education and training in oral health care, the nursing workforce has the potential to improve access and quality of oral health care. Education and training about activities of daily living could incorporate oral health care practices along with bathing, toileting and dressing. Oral health outcomes could be improved using an interdisciplinary approach to care.
Earlier Intervention
Assisted Living facilities are the fastest growing segment of the nursing care continuum,48 with the typical assisted living resident being much like the nursing facility patient of the past with a high burden of functional impairment and related illness.49 Research concerning oral care provision centers on highly regulated LTC facilities. Limited attention is given to unregulated assisted living facilities. A comprehensive report funded by the State of Florida Health Care Administration revealed a general lack of oral care during the period after retirement and before entering a nursing facility.50 Results from the current study indicate assisted living residents are less likely to have a dental exam than LTC residents. Residents of assisted living did not receive assistance with oral hygiene and a dental plan was not required. Downstream medical costs could be reduced by increasing access to oral care at this critical juncture by preventing disease and its associated comorbidity.
Policy
The Institute of Medicine's longitudinal landmark study cited numerous recommendations for policy reform including the establishment of a unified set of items and definitions for assessing all residents in nursing facilities in the nation.51 Concerns about poor quality of care and the rights of residents within the nursing home led to a government mandate known as the 1987 Omnibus Budget Reconciliation Act (OBRA) which provides a set of standards for nursing homes known as the minimum data set.52,53 Regulations, such as minimum data set, are in place today in an attempt to improve and monitor the quality of care provided in LTC,53 yet many LTC residents have inadequate access to oral care.11,18 The inadequacy of the minimum data set has been reported by a study of Iowa nursing homes in which it was determined that the use of the oral, nutritional and dental sections of the minimum data set are often not useful and not used as intended in the identification of dental needs.25 These regulations need to be updated to reflect the changing needs of older adults, who are living longer and retaining their teeth, so they have improved oral care.
In addition to OBRA regulations, Arkansas, as in most states, require that facilities establish a written cooperative agreement with an advising dentist or dental service which includes a provision to participate annually in a staff oral hygiene policies and practices development program.54 Conclusions from studies of both LTC and assisted living facilities indicate that oral health policies and practices vary, and that dental involvement in policy creation and in providing consultation and service is limited.28,36 The current study supports these findings as evidenced by LTCs reporting annual policy development programs with inconsistent amounts of in-service education. Oral health care personnel in assisted living seemed receptive but stated they were not required to provide any dental care other than transporting the resident to a dentist if necessary. Lack of time and funding, as well as an overall low priority seems to prevail.
Lack of on-site dental equipment and unwillingness of specialty and general dentists to provide care at nursing facilities were two of the primary barriers that emerged during this study. Further, time constraints of nursing staff presented a significant barrier making oral preventive care a low priority in this study and previous studies.28,36,55 The oral health care personnel in the present study expressed a need to provide more dental services within the familiar environment of the nursing home and with the assistance of a consistent caregiver or family member. This change would address identified concerns such as inability to communicate, lack of cooperation, dementia and weight loss. Multiple studies report similar needs and barriers.15,56,57
Interestingly, the Arkansas state penitentiary employs a dental hygienist in an on-site dental clinic raising questions about the parity of policies and infrastructure in place for providing oral care within the state. This inequality is further illustrated in the 2011 Arkansas report card published by the PEW Center on the States where children's' oral health improved from a “F” in 2010 to a “C” in 2012.58 Infrastructure in Arkansas has been modified to provide access to oral health care for many different populations; however, older adults are being overlooked. A recent survey of the burden of oral disease in Arkansas has found demographic inequities in older adults especially with regard to education, race and gender.59 Updating regulations and policies to require individualized care plans developed by a dental professional should be in place and available for all individuals.
The Role of the Dental Hygienist
The use of non-dental professionals to conduct assessments is needed to improve access. An interdisciplinary team approach, that includes dental professionals is necessary to more accurately identify oral health care needs and therefore facilitate the development and implementation of effective oral health care plans and educational programs. Implementation using an interdisciplinary model will be challenging. The present study underscores this disconnect in response to reports of frequent turnover of facility employees and a variety of providers with an inconsistent degree of oral health knowledge. One oral health care personnel stated that many of the caregivers do not have good oral care themselves and often do not feel it is a priority for residents. Educating staff members to value their own oral care as well as residents is important to increase the overall awareness of quality oral care. Dental hygienists could aid in increasing the confidence of the caregiver in providing oral care and reduce some of the stress associated with caring for uncooperative residents. Based on insight from oral health care personnel, dental hygienists could be used to increase retention by alleviating some of the demanding workload of the oral health care personnel. Results from a recent pilot study conducted in Arkansas demonstrates how hands on support from a dental health champion working in collaboration with oral health care personnel can have a positive impact on the oral health of residents in LTC settings.60
The present study suggests that oral health care personnel are overall receptive to the use of dental hygienists in providing care in their facilities; however, no current involvement exists. This circumstance is a problem in Arkansas because of limitations preventing dental hygienists from providing oral care and the small number of dentists treating residents within the facilities despite the apparent need. In 2011 the dental practice act in Arkansas was modified to allow them an opportunity to attain a Collaborative Care Permit enabling dental hygienists to provide needed oral care to populations that lack access. The permit, which mirrors other states' workforce models, is just beginning to be implemented in Arkansas. The possibility of increasing access to care in Arkansas through direct access to dental hygiene preventive services as outlined by the Collaborative Practice Permit promises to alleviate some of the disparities in oral health care and is a response to the state's efforts to increase access to care based on needs found in oral health care reports.30 This model of care has demonstrated success in Louisiana. Testimony from Folse describes his geriatric model of care which uses hygienists to complete facility minimum data set items and provide treatment.61 He states:
“Without general supervision which fully enables a hygienist's abilities, I would not have a viable prevention model or the ability to provide my patients access to comprehensive care. Working with hygienists has increased the entry points of my patients into the dental delivery system. This is a winning model for my patients.”61
Future Research
Replication of this study in other states would be beneficial to improve generalizability. In order to achieve an acceptable survey response, future research with this target population should explore ways to connect with oral health care personnel “in person” in settings such as professional meetings. In person contact was suggested by oral health care personnel due to lack of time, and lack of access to electronic or regular mail within their workplace. Investigators may want to offer incentives for survey participation. A mixed methods approach incorporating before and after focus interviews along with a survey could also strengthen and enrich this study type. Additional suggestions for future research are to assess the perceptions of oral health care personnel as to their own oral care practices and beliefs and to investigate dentists and dental hygienists in Arkansas to determine their interest in, or experiences with providing care through the use of a Collaborative Care Permit.
Conclusion
This qualitative case study suggests access to oral health care for residents living in both LTC and assisted living I and II facilities in Arkansas is affected by public and facility policies and access to oral health care as a function of the patient's health status and availability of oral health care providers. Access for residents residing in assisted living I and II facilities is also limited by the residents' ability to assume responsibility for accessing oral health care. The outcomes from this study may serve to inform policymakers and advocates for access to oral health care as they develop new approaches to address this growing need.
Acknowledgments
We are grateful for research support from The University of Missouri Kansas City Research Support Committee. The authors also thank Dr. Edward Gbur at the University of Arkansas Fayetteville for his help with statistical analysis, the Arkansas Health Care Association for their assistance with the electronic survey and Barbara Smith for use of the survey instrument.
Footnotes
-
Virginia M. Hardgraves, RDH, MS, is an Instructor of Dental Hygiene at the University of Arkansas-Fort Smith. Tanya Villalpando Mitchell, RDH, MS, is an Associate Professor and Director, Graduate Studies; Carrie-Carter Hanson, RDH, EdD, is an Assistant Clinical Professor; Melanie Simmer-Beck RDH, PhD, is an Associate Professor. All are at the University of Missouri-Kansas City.
-
This study supports the NDHRA priority area, Health Services Research: Identify how public policies impact the delivery, utilization, and access to oral health care services.
- Copyright © 2014 The American Dental Hygienists’ Association





{kind=link}