



Abstract
Purpose: Autism Spectrum Disorder (ASD) can greatly inhibit a child's communication and social interaction skills, impacting their comfort during dental hygiene treatment and services. Children with ASD may exhibit sensory sensitivities, fear of the unfamiliar and lack of socio-cognitive understanding, leading to anxiety and corresponding behavioral deficits. Since the prevalence rates for ASD have risen significantly in the past decade, increased emphasis has been placed on educational and behavior guidance techniques, which can be helpful for children with ASD because of their increased capabilities in visual-processing. The purpose of this literature review is to summarize the interventions available to reduce dental anxiety in children with ASD, and to determine which strategies are best suited for implementation by the dental hygienist. Advancements in technology and socio-behavioral interventions were assessed for appropriate use, efficacy and engagement in the target population. Interventions were categorized into the following groups: picture cards, video technologies and mobile applications.
Introduction
Autism spectrum disorder (ASD) is the diagnostic term for a complex, heterogeneous, neurodevelopmental disorder, which manifests most commonly as difficulty with social communication and in the occurrence of behaviors that are atypical in appearance, frequency and/or magnitude.1 A diagnosis of ASD is typically made before age 3, when caregivers begin to notice unusual behaviors or delayed development in the areas of social communication and social interaction. For example, the child may not respond to the caregivers' presence, voice or touch, seem disinterested in social interactions with peer groups, exhibit delays in speech and communication, and engage in repetitive body movements or avoidance behavior.2,3
According to the Autism and Developmental Disabilities Monitoring Network, the prevalence of ASD in 8 year old children has risen from approximately 1 in 150 in the year 2000, to 1 in 68 in the year 2010.2,4 A prevalence rate of 2.00% (1 in 50) was calculated for children ages 6 to 17 in the years 2011 to 2012, as compared to 1.16% (1 in 86) from the year 2007.5 For unknown reasons, the disorder is almost 5 times more likely to occur in males than females; however, no link can be found between prevalence rates and factors such as race, ethnicity or socioeconomic status.5
Symptoms of the disorder vary considerably in each individual. Although a child diagnosed with ASD will have deficits in social communication and behaviors, those with mild ASD may have strong cognitive abilities that foster the learning of appropriate replacement skills in these deficit areas. As a result, children with mild ASD may only demonstrate impairments in social skills and interpersonal relationships. Conversely, a child with a more severe form of ASD may demonstrate significant speech impediment, unusual or repetitive behaviors, perceived in-difference toward others, emotional outbursts, and hypersensitivity to new stimuli.6 The range in symptoms makes it difficult to predict how each child will be affected; therefore, individualized educational and/or behavioral interventions are often necessary to help the child function effectively and comfortably with others, especially in novel settings.7
A dental hygiene appointment can be especially difficult for children with ASD since the child is in an unfamiliar environment, surrounded by new people and things. Approximately 40% of children diagnosed with ASD receive a comorbid diagnosis of anxiety disorders, which can exacerbate deficits in communication and socialization while increasing in-appropriate behaviors such as self-stimulation, self-injury and tantruming.8 Furthermore, anxiety may be increased by the inability of the child to effectively communicate fears and/or reservations experienced at the thought of undergoing dental treatment. There are foreign sights, smells and sounds that a child must absorb and process during a short period of time, such as hand pieces, suction, bright lights and personal touch, all of which are stimuli that can exaggerate sensitivities and make the child feel uncomfortable. During this process, a child with ASD can easily become overwhelmed on all sensory levels: visual, auditory, tactile, olfactory and gustatory.9,10 Sensory overload is associated with negative reactions in children with ASD and can lead to aggression, self-injurious behavior, emotional out-bursts, attempts to block the stimuli, or physical and social withdrawal.7,9,11,12 This behavior makes conducting dental hygiene treatment extremely difficult, prompting some dental professionals to consider sedation, physical restraint or referral to a pediatric specialist who may also employ these techniques. Though sometimes necessary, neither sedation nor restraint are absolutely safe and effective. Pharmacological sedation is considered highly controversial due to high cost and associated health risks, while medical restraint can cause psychological and physical trauma in people with intellectual disabilities (Table I).12-17
There are options for reducing dental anxiety, such as social and communication training, which do not carry the same medical risks as sedation and restraint. Advancements in special education and behavioral guidance have allowed children with ASD to achieve comfort and relaxation, resulting in more cooperative behaviors during situations known to induce anxiety or stress.7,18 A thorough understanding of associated symptoms, hypersensitivity reactions, behavioral response, treatment options and intervention strategies could allow dental hygienists to interact more effectively with children with ASD.
The primary focus question for this literature review was: what interventions are available to reduce dental anxiety in children with ASD? A secondary focus question was: which are the best interventions for use by the dental hygienist to help children with ASD receiving dental hygiene services? There were 38 scholarly journal articles collected that were applicable for this review. The inclusion criteria consisted of the following: published between January 2000 and April 2014, published in peer-reviewed journals, primary sources (including intervention studies, case reports, randomized controlled trials and surveys), publications of a medical or government organization (such as Centers for Disease Control and Prevention (CDC) or National Institutes of Health (NIH)), written in English, full text available, related to topic, and applicable to focus questions.
Picture Cards
By far, the most studied intervention for children with ASD is use of the Picture Exchange Communication System (PECS). PECS uses cards featuring a simple picture paired with its associated word, phrase or sentence and includes 6 phases of training: how to communicate, distance and persistence, picture discrimination, sentence structure, answering questions, and commenting.19 Children are taught to choose the appropriate card to express their wants, needs or feelings and present the card to a “communicative partner” as an alternative form of expression. The ASD population is ideal for training with PECS due to the disorder's characteristic developmental delays in language and social skills, including lack of eye gaze. Children with ASD may begin speaking much later than their typically-developing peers, may use a vocabulary of fewer or more simple words, or may be completely nonverbal. Not only does PECS allow the child to learn a larger and more complex vocabulary while associating those words with pictures and ideas, it requires the child to physically present the card to others, thereby initiating social interaction between the child and the communicative partner.19

Example of a Social Cue Card Series for a Student Who Frequently Throws Tantrums When Asked To Get Off the Computer18
Studies using picture cards, such as PECS, as the sole intervention demonstrated increases in verbal speech, spontaneous communication and social-communicative behaviors, and a decrease in problem behaviors.20-23 The study by Gordon et al is of particular importance because it utilized 84 participants from 15 schools in a randomized controlled trial of PECS, which is rare when conducting research on children with ASD.23 Due to varying degrees of symptom severity, diverse presentation of deficits, difficulty matching controls and the heterogeneous nature of the population, limited sample sizes are common. Similarly, 2 studies utilized social cue cards to resolve unfavorable conduct, practice acceptable verbal and physical communication, and maintain targeted social skills in children with ASD.20,24 The social cue cards show a simple picture paired with an age-appropriate social story, which are attached together in sequence and read to the child in a step-by-step fashion (Figure 1). The use of social stories in general is a popular behavioral intervention for children with ASD.25 Social stories are read prior to a specific social situation, and are not used to elicit a specific change in behavior, but to facilitate the understanding of social situations and the perspectives of other individuals in the setting.26 When utilized together, social stories and social cue cards help to mediate problem behavior by ensuring the student is aware of appropriate responses expected during a given situation.
Another method for decreasing inappropriate behaviors in children with ASD is to teach the child to appropriately express anxiety. The use of functional communication training, where a child is taught a communication skill to replace a behavior (e.g. raise hand to ask for a break instead of hitting), is one of the most effective methods for decreasing inappropriate behaviors.27 Studies which implemented functional communication training with picture cards demonstrated that the presence of the cards during social situations improved the subject's ability to interact effectively with others, and the use of functional communication training facilitated the learning of picture card systems.28,29 In Danov et al, the primary targeted behavior was self-injury, and results revealed a significant decrease in self-injurious behavior (SIB) after intervention with functional communication training and picture cards.28 The child began utilizing the cards to communicate a want or need for desired objects instead of SIB. Similarly, in Hines et al, the subject displayed more of the desirable “appropriately engaged” behaviors and less disruptive behaviors after intervention with functional communication training and picture cards.29 When the picture cards were unavailable, the child reverted to problematic behaviors such as disruptive vocalizations, refusal to participate and lying on the floor, which demonstrates the importance of having the cards present and accessible once they are learned (Table II).29
Video Technology
The literature suggests electronic screen media is an ideal educational tool for children with ASD because this population tends to favor visual stimulation.30,31 A survey of caregivers indicated children with ASD show more interest in watching television and video than using the computer, and a predilection for animated programming versus non-animated.31 Additionally, children with ASD most often engaged in verbal and physical imitation while viewing electronic screen media.31 Given the preference for animation, children with ASD may be more attentive to video modeling techniques featuring an animated character whose actions can be easily followed and imitated.31
Studies incorporating a component for both picture cards and video technology support the use of video technology for children with ASD.18,32 In one such study, instructional video clips were created and implemented to teach the selection and retrieval of picture cards to express requests.32 Video technology was utilized in this case because children with ASD often do not attend to their surroundings, including people, and therefore do not readily obtain new skills through observation of their environment or behavioral models.33 Video technology is known to attract the attention of children with ASD and can be easily adapted to present the desired content. However, the study found the ability to pay attention to the screen for approximately 10 to 26 seconds (full length of the video clips) was a necessary prerequisite to successful intervention.32 If the child lacked the ability to fully attend to the presented message, he or she was unlikely to learn content through video modeling.32 Orellana et al used both pictures and videos in a training program to achieve a complete dental examination in children with ASD.18 The video showed a model patient executing the “10 steps” of an oral assessment, which included entering the room, lying back in the chair and pressing the teeth together in occlusion. The majority of children (81.6%) participating in the program successfully accomplished cooperative behavior (e.g. remain sitting still, legs stretched out, mouth open) during an intraoral examination with mirror and probe, showing great potential for similar exercises conducted by dental hygienists.18
Summary of the Current Literature on Picture Card Interventions for Children with ASD
Summary of the Current Literature on Video Technology Interventions for Children with ASD
Advancements in virtual reality technology over the past decade have contributed to exploration of educational virtual reality interventions for children with ASD. Two separate studies using virtual reality simulations to teach safety skills found students learned the material more quickly when immersed in virtual reality.34,35 Students aged 6 to 12 learned proper fire drill behavior during a simulated building tour, and were able to generalize this training in a real-life fire drill in the school setting.34 The research noted that children with ASD were able to effectively implement their virtual reality safety training in similar real-life scenarios at a rate of over 50%.35 While these results appear promising, it is unclear if virtual reality could be effective for use by the dental hygienist due to the slower-paced and less physically involved nature of dental hygiene treatment. More research on virtual reality training in the dental hygiene setting is needed to confirm efficacy for children with ASD.
When considering the overall engagement of virtual reality technologies, there may be a potential for anxiety reduction through mere distraction. A study comparing video technology (animated versus self-immersed) and virtual reality simulations (familiar person versus self-immersed) found all 4 strategies were able to hold the attention of 6 to 18-year-olds with ASD.36 While the self-immersed video and self-immersed virtual reality conditions achieved the longest gaze durations, virtual reality simulations in general garnered more vocalizations than traditional video viewing.36 Thus virtual reality programs, which can be utilized for distraction and relaxation during dental hygiene services, are a suitable intervention for children with ASD (Table III).
Mobile Applications
The popularity of mobile devices with high-speed internet connectivity has contributed to increased use of standard and downloadable applications. One advantage of mobile devices is convenience of use - the portability of handheld technology allows the user access to his or her applications almost anywhere and anytime. This is particularly valuable when educating children with ASD, who benefit from repetition of content when learning new skills and information. For example, if socio-communicative interventions learned in the classroom are encouraged outside of the school setting, they are more likely to be retained for later use in social situations.37,38
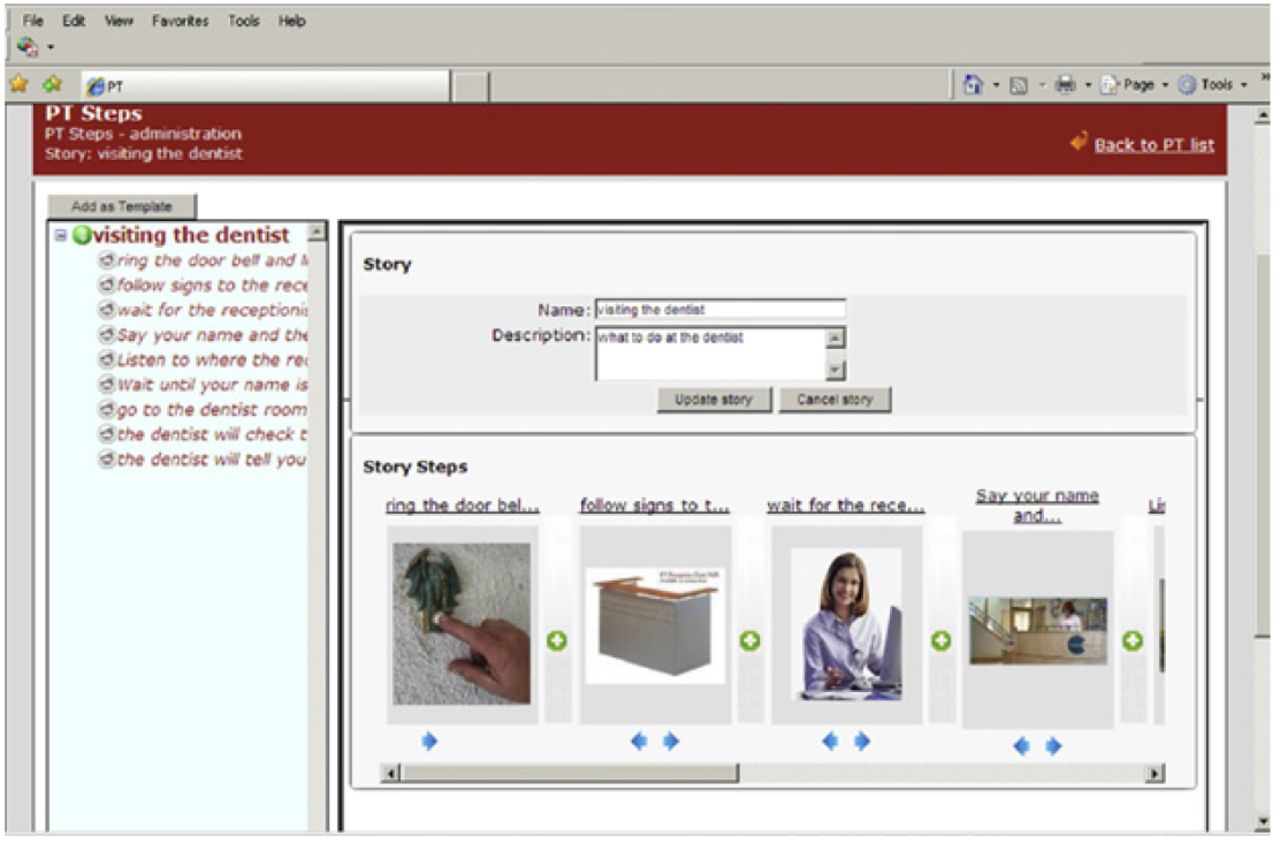
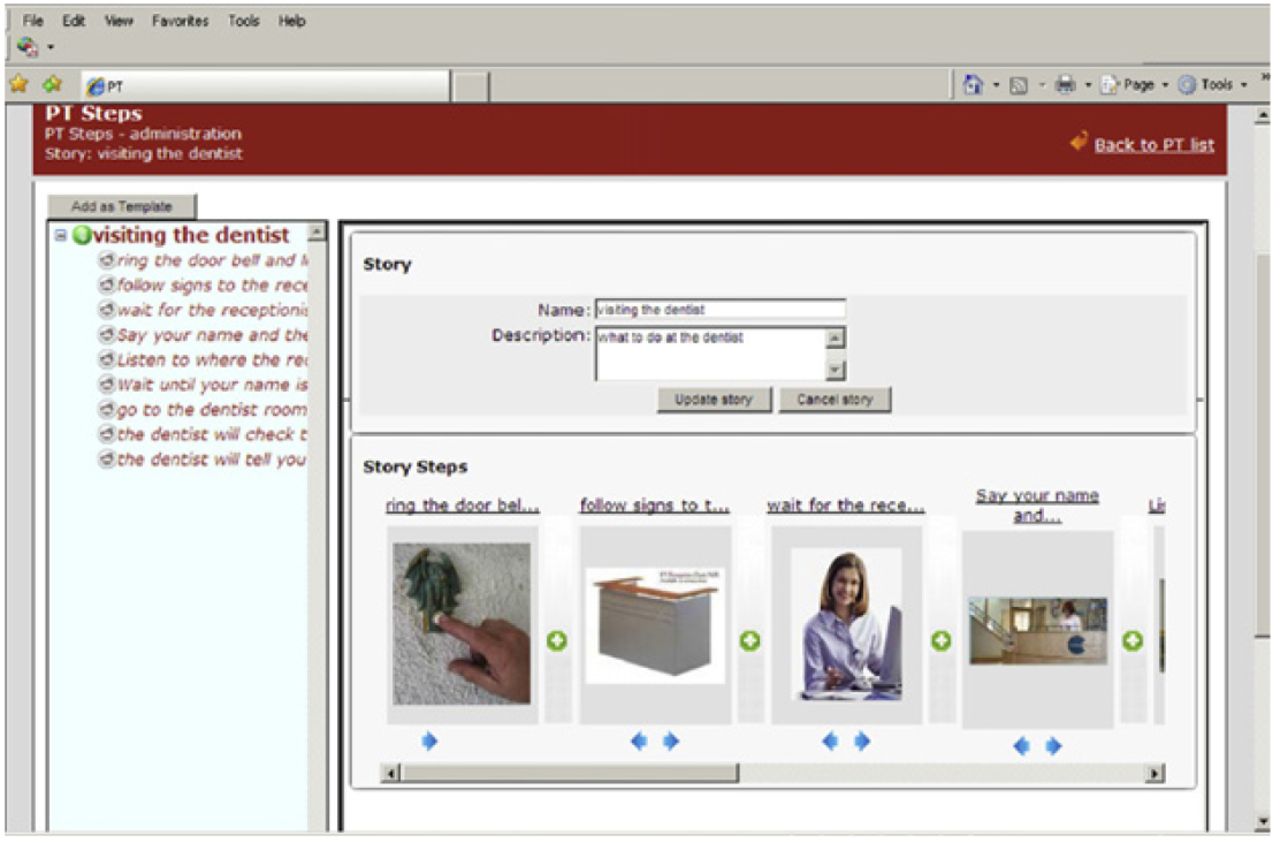
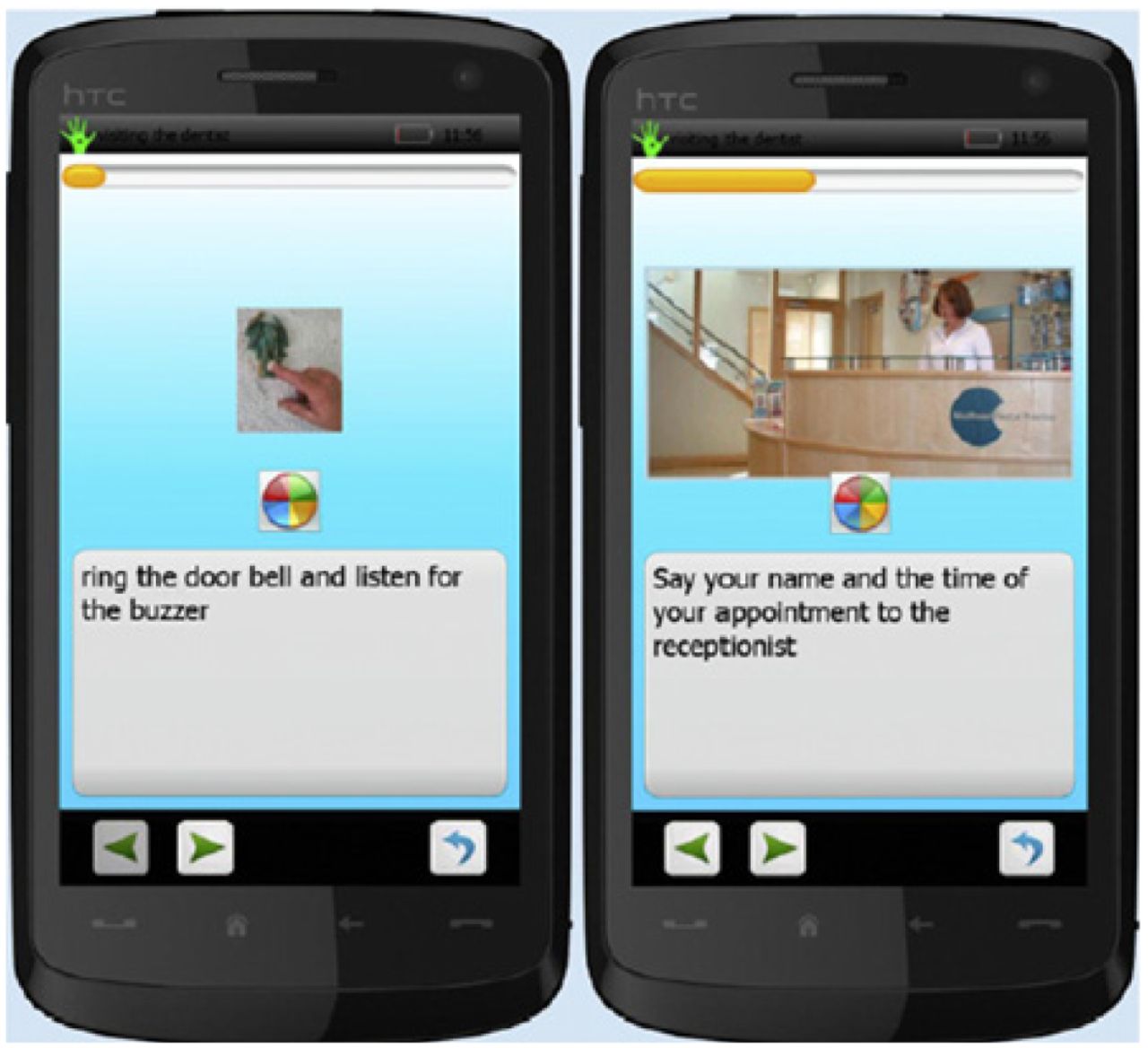
Mintz et al developed an application for smartphones to support social skills and life skills via a flexible software design.37 Key benefits of the software include using the teacher's or caregiver's picture and voice with instructions, use of a rewarding video with the appropriate action or response, and the ability to track logged time and achievements.37 The program is designed to enhance social skills by encouraging calm, rational behavior in situations likely to induce high levels of anxiety, and by prompting consideration of others' perspectives during everyday discussion and interaction. Mixed reviews prompted critical evaluation of the application's components. Consequently, a second prototype was created using the same foundations of the original application with a redesigned graphical user interface.38 The technical adjustments allowed the program to have a more stable internet connection and user-friendly interface, providing further support for case-specific intervention via smartphone application (Figures 2, 3).38
Picaa is a mobile learning platform created for elementary school children with ASD, and is based on the iPad and iPod touch devices.39 The program provides flexibility of content, exchange of content between professionals, mobility between multiple devices, and a built-in accelerometer that responds to rotations or movements of the device.39 The capability for personalization and adaptation of the educational content is necessary to focus the intervention for a specific learning deficit. The Picaa application provides templates that educators can use to create individualized lesson plans and learning exercises for each student.39 The researchers observed a significant increase in scores for all 5 skill categories: language, math, environmental awareness, autonomy and social skills.39 The significant difference in scores confirms Picaa platform's potential as a tool for developing educational skills in children with special needs.
Additionally, studies utilizing computer and smartphone applications demonstrated improvement in literacy skills, engagement, on-task behavior and the ability to maintain a set schedule in children with ASD.40,41 For example, a case study describing the use of Microsoft PowerPoint as an educational intervention was used to train a child with ASD how to research favorite topics and create non-fiction texts. The project helped the child enhance his literacy skills by increasing interest, engagement and attitude regarding reading.41 Overall, the customizable and multifaceted nature of mobile applications makes them appropriate and convenient for use in most situations and settings; therefore, they are a viable option for helping children with ASD cope with receiving dental hygiene care (Table IV).
Discussion
Research testing the effects of picture cards, video technology and mobile applications has shown great potential for helping children with ASD access dental hygiene treatment.18,37,38 However, due to the heterogeneous nature of this community, it is very difficult to find a “one-size-fits all” intervention to decrease stress and anxiety, and increase comfort, cooperation and learning. Dental hygienists treating children with ASD should be knowledgeable in the above mentioned interventions and work with caregivers well in advance of the first physical visit to become acclimated with the child's behaviors, sensitivities and symptom severity. Many resources are available to prepare for children with ASD undergoing dental hygiene treatment to include continuing education courses, online resources and local autism support groups or special education professionals.

It is helpful to inquire which learning tools are already used at the child's home or school to coincide with the child's learning preferences. For example, mobile applications can provide an appropriate and fun tool for children with a mild form of ASD, who may be high-functioning with an exceptional ability to navigate various forms of technology.37-41 Mobile applications are convenient for use in the waiting area or treatment rooms, especially for children who already use a tablet or mobile phone.
Summary of the Current Literature on Mobile Application Interventions for Children with ASD
To increase verbal or non-verbal communication, the dental hygienist can incorporate a picture card or video prompting system.20-24,28,29,32,33 Picture cards and video prompting are often the best option for children with a more severe form of ASD, who may be dependent on caregivers for activities requiring fine motor skills. Additionally, video and virtual reality technology can be used to familiarize children with the dental hygiene process and as a distraction technique during the appointment.30-36
Video modeling can be beneficial prior to and during dental hygiene treatment if the child watches a video and imitates the on-screen actions, such as an animated character that demonstrates how to “lay back in the chair,” “put your feet out straight and hands on your stomach,” and “open your mouth to show your teeth,” thereby teaching the child ideal patient positioning. Both picture cards and video technology offer a do-it-yourself option, as the cards, social stories and short video clips can be made at home or in office. Other interventions, such as mobile applications and virtual reality systems, may be more costly with fewer options available on the consumer market. More interventions utilizing electronic screen media technology need to be developed and made available to help dental professionals provide treatment for children with ASD.
Conclusion
A lack of social awareness, fear of the unknown, and sensory sensitivities can make dental hygiene treatment very difficult for children with ASD. While sedation and restraint techniques have been used in the past, socio-communicative and behavioral training are the preferred methods for reducing dental anxiety. Incorporating educational and behavior guidance techniques prior to and during the dental hygiene appointment can help providers achieve a more successful outcome of care. Early familiarization may prevent the child from feeling so overwhelmed in an environment with multiple forms of new stimuli. When children with ASD have gained initial trust in the dental hygiene environment, subsequent appointments will most likely be less traumatic. Improving oral care experiences and opportunities for this unique population directly translates into increased access to care and oral health-related quality of life.
Footnotes
Jessica L. Elmore, BSDH, MS, is a registered dental hygienist in private practice and is an Adjunct Assistant Professor at the Gene W. Hirschfeld School of Dental Hygiene, Old Dominion University. Ann M. Bruhn, BSDH, MS is an Assistant Professor at the Gene W. Hirschfeld School of Dental Hygiene, Old Dominion University. Jonna L. Bobzien, PhD is an Assistant Professor in the Department of Communication Disorders and Special Education, Darden College of Education, Old Dominion University.
This study supports the NDHRA priority area, Health Promotion/Disease Prevention: Identify, describe and explain mechanisms that promote access to oral health care, e.g., financial, physical, transportation.
- Copyright © 2016 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}