



Abstract
Purpose: There has been an increase in awareness of the link between oral health and systemic health in recent years. While questions exist about the relationship of oral disease to cardiovascular conditions, no published study to date has addressed cardiologists' knowledge and opinions about this area of science. This study examined North Carolina cardiologists' knowledge, opinions and practice behaviors regarding periodontal disease and cardiovascular disease.
Methods: A survey was developed, revised, pilot tested and mailed to 625 licensed, practicing cardiologists' in North Carolina. A total of 3 mailings were conducted. Data were analyzed using descriptive statistics.
Results: The response rate was 19% (n=119). Respondents were mostly males (86%) and working in private group practice (48%) or academia (32%). Sixty three percent correctly identified the first sign of periodontal disease; however, only 18% choose the correct etiology of periodontal disease. Sixty percent of respondents stated that medical students and dental students should be trained to work collaboratively. Half of cardiologists' surveyed were unsure that treatment of periodontal disease can decrease a patient's risk for cardiovascular disease. The majority were interested in learning more about the relationship between cardiovascular disease and periodontitis.
Conclusion: The majority of cardiologists surveyed were unclear about the etiology of periodontal disease and would like to have more information about the potential oral-systemic link regarding cardiovascular disease. It is important for educators and administrators in higher education to examine the need for interprofessional education and collaboration between medicine and dentistry. This study may provide valuable information about ways to implement more effective interprofessional education and collaboration between dental and dental hygiene professionals and cardiologists to improve oral health.
Introduction
Oral systemic health has been a topic that is gaining more attention in the U.S. The Institute of Medicine (IOM) 2011 report on Advancing Oral Health in America concluded that in order to enhance the delivery of oral health care across the U.S., a collaborative effort across multidisciplinary health related fields is necessary.1
The U.S. Surgeon General's report noted that there is an association between chronic oral infection and diseases such as diabetes, heart disease and pre-term low birth weight babies.2 The IOM report along with the report from the U.S. Surgeon General regarding oral health in America discusses the association between oral health and other systemic conditions. The report also states that there is a lack of knowledge or training of non-dental health care providers in the area of oral health care. The IOM committee concluded that non-dental health care providers could have an increased role in oral health care. It also stated that interprofessional, team-based care could provide the best care to patients.1
Periodontal disease is a common oral disease that affects approximately 47.2% of the adult population in the U.S. In adults aged 65 and older the prevalence increases to 70%.3 Periodontitis is a bacterial induced, chronic inflammatory disease that destroys the supporting tissues surrounding teeth. A general dentist or periodontist clinically diagnoses periodontal disease using variables such as tooth loss, recession, clinical attachment loss, periodontal pocket probing, tooth mobility and radiographic bone loss.4-10 Factors such as smoking, type 1 and 2 diabetes mellitus, cardiovascular disease, and obesity have also been linked to the risk associated with developing periodontal disease.6,10-17
Cardiovascular disease is the leading cause of mortality in the U.S., with approximately 11.5 % of Americans having been diagnosed. High blood pressure, low-density lipoproteins and smoking are all risk factors associated with cardiovascular disease.18 The Center for Disease Control and Prevention (CDC) estimates that coronary heart disease costs the U.S. $108.9 billon dollars each year.19 Several studies have reported that periodontal disease pathogens and inflammatory markers are common between cardiovascular disease and periodontal disease.6-9,20,21
Cardiovascular Disease and Periodontal Disease
Cardiovascular disease and periodontal disease have many of the same contributing risk factors such as smoking, diabetes and age. It has been suggested that periodontal disease is a direct pathway by which the 2 diseases could be associated. Mucci et al hypothesized that inflammatory mediators that react in response to periodontal pathogens could have a possible effect on the systemic inflammatory response to the development of atherosclerotic plaque.16 Periodontal infections could be a casual pathway to cardiovascular disease though bacteremia or inflammatory mediators provoked in response to the pathogen. Therefore, this systemic inflammatory response may induce the development of atherosclerotic plaque.16
Blaizot et al conducted a meta-analysis of observational studies using a methodological process of reviewing 215 epidemiological studies.5 The meta-analysis examined the association between exposure to periodontitis and cardiovascular disease. Of the 215 studies, 22 case-control and cross sectional studies along with 7 cohort studies were selected to use in the analysis. The results supported an association between persons with periodontal disease and cardiovascular disease. This analysis provided evidence that many of the risk factors associated with cardiovascular disease and periodontal disease are independent of each other. It concluded that further research is needed to examine the pathophysiological process between the two.
Poor oral hygiene is the major cause of periodontal disease. This chronic oral infection is related to a systemic inflammatory response. Periodontal disease has been reported to cause an increase in the C-reactive protein levels in patients. Systemic inflammation could signify the mechanism that links periodontal disease and cardiovascular disease. de Oliveira et al conducted a survey to measure if self-reported tooth brushing and oral hygiene was associated with an increase in cardiovascular disease.21 The results indicated that persons with reported poor oral hygiene had a higher risk of cardiovascular disease and low-grade inflammation but the causal nature was yet to be determined.
Another meta-analysis focused on prospective cohort studies conducted among the general population. The purpose of this meta-analysis was to determine the relationship between periodontal disease and coronary heart disease. This analysis also reported that biological markers such as C-reactive protein serve as an indicator for additional coronary heart disease. It reported that periodontal disease results in approximately a 24 to 35% increased risk for coronary heart disease.8
With the potential effect for periodontal disease to increase risk for cardiovascular disease, it is important for the dental and medical professions to work together to help reduce the risk for adverse outcomes for patients. In 2009, a set of clinical recommendations for patients with periodontal disease and/or cardiovascular disease was published.22 These recommendations were established to provide guidance to both cardiologists and periodontists regarding the link between cardiovascular disease and periodontitis and a potential approach to reducing the risk for cardiovascular disease in patients who have periodontitis. The recommendations were important because they represented the first of its kind between cardiologists and periodontists.
In 2012, the American Heart Association (AHA) issued a scientific statement regarding the association between cardiovascular disease and periodontal disease. Health care professionals from dentistry, infectious diseases, cardiology and epidemiology formed a group to assess and measure the scope of evidence for an association or causality between the 2 diseases. A total of 282 peer-reviewed publications were selected for a literature review.23 The AHA statement suggests that there are significant gaps in the scientific understanding of the interaction of oral health and cardiovascular disease. Therefore, it is stated that while there is an association between cardiovascular disease and periodontal disease, there is not a causal relationship.23
Health Care Practitioners' Knowledge and Practices Regarding Oral Systemic Diseases
The area of oral systemic health is continuing to grow in the U.S. It is important to assess the current knowledge and practices of health care practitioners' regarding oral systemic diseases. It is also imperative to examine the roles of both medical providers and oral health care providers in assessing the practice behaviors regarding patient care.
Lewis et al assessed pediatricians' knowledge, attitudes and professional experience regarding oral health and to determine pediatricians willingness to incorporate fluoride varnish into their practices.24 They conducted a survey of 1,600 randomly selected pediatricians using the American Medical Association list of pediatricians. The survey assessed the knowledge, current practice and opinions on their role as a pediatrician to promote oral health. The response rate was 62% with 1,386 eligible survey recipients. Two-thirds of respondents observed caries in their school-aged patients. While the majority of respondents referred patients to a dental office or clinic, 55% reported difficulty in achieving referral for uninsured patients, and 90% agreed that they played an important role in promoting and educating patients on the importance of oral health.
Owens et al surveyed 1,000 internists and 115 endocrinologists to determine their knowledge, opinions and practice behaviors regarding periodontitis and diabetes.25 The survey received a 34% response rate. Knowledge about periodontal disease was high and the respondents agreed that physicians should be taught about periodontal disease and be trained to do screenings for periodontal disease. The majority of respondents indicated that there is a link between periodontal disease and diabetes; however, the majority were not familiar with studies regarding the relationship between the 2 diseases.
Wooten et al surveyed 404 nurse practitioners' and certified nurse midwives' to determine their knowledge, opinions and practice behaviors regarding periodontal disease and adverse pregnancy outcomes.26 The results indicated that nurse practitioners and certified nurse midwives had limited knowledge about oral health. Both the Owens and Wooten surveys concluded that collaborative efforts between healthcare providers and oral health care providers would benefit patients in various areas of health care.25,26
Oral Health Care Practitioners' Knowledge and Practices Regarding Oral Systemic Diseases
Collaborative efforts made by the dental team and cardiologists could help to identify and reduce oral/systemic diseases. The dental hygienist is an essential component to the dental team. Dental hygienists receive extensive training on medical histories and systemic diseases, as well as oral diseases such as periodontal disease. The dental hygiene process of care is multifaceted to include assessment, implementation and evaluation of outcomes.27 Bell et al stated that it “is the responsibility of the dental hygienist to make assessments based on patients' systemic health to promote a healthy lifestyle in addition to providing safe and effective dental hygiene care.”28 The Bell et al study also reported on practice behaviors of dental hygienists incorporating oral systemic evidence into patient care. In this study, a survey was conducted to assess whether dental hygienists updated medical histories at every appointment, assessed blood pressure and obtained blood sugar readings. During the assessment phase of care, 84% of the respondents reported that it is the dental hygienist who performs a periodontal exam on new patients. The survey also indicated that 64% of the respondents performed periodontal examinations at every visit for periodontal maintenance patients. Sixty-eight percent of respondents reported that medical histories were updated at every visit, and 92.9% discussed medications and medical diagnoses with all patients. However, very few record blood sugar levels. The results from this survey exhibited that respondents are incorporating some aspects of oral systemic evidence into patient care.29
Although there is some evidence that there is an association between periodontal disease and cardiovascular disease, little is known about medical providers' knowledge about the link. The purpose of this study was to examine the knowledge, opinions, and practice behaviors of North Carolina cardiologists' regarding the association between cardiovascular disease and periodontal disease.
Methods and Materials
A cross- sectional survey was designed to assess North Carolina cardiologists' knowledge, opinions and practice behaviors regarding the relationship between cardiovascular disease and periodontal disease. The survey was adapted from a questionnaire developed at the University of North Carolina that focused on a similar topic regarding oral and systemic health. The survey was modified to address the current research questions. Thirty four questions were included and divided into 6 sections that included the following topics:
Practice setting
Oral examinations
Oral and systemic health
Opinions about periodontal disease
Education
Demographics
A list of cardiologists was obtained from the North Carolina Medical Board. Although the list contained the names of 1,160 registered cardiologists in the state of North Carolina, only 625 were actively practicing cardiology, so surveys were mailed to 625 cardiologists. The selection criteria included cardiologists practicing full time or part time in a public, private or government practice in North Carolina. Retired cardiologists, pediatric cardiologists or cardiologists practicing outside of the state were excluded from the study.
The survey was reviewed and approved by the Institutional Review Board. Following the approval, the survey was pilot tested with 5 practicing cardiologists. After minor changes, the survey was produced using Teleform, a scannable format that simplifies data entry. The survey, along with a cover letter explaining its purpose and business reply envelope was mailed using the Salent and Dillman method.30 There were 2 mailings in the fall of 2012 and a final mailing in January 2013. To maintain confidentiality, there were no identifiers on the surveys and random identification numbers were assigned to each subject. All data was stored in a password-protected database that was only accessible to the research team and statistician. The data were analyzed using SAS version 9.1 (SAS Institute Inc., North Carolina) using descriptive statistics.
Demographics of North Carolina Cardiologists (Respondents)
Results
A total of 119 surveys were completed as requested and were useable for data analysis, resulting in a 19% response rate. Demographic data is reported in Table I. Seven percent of respondents have been providing patient care for less than 5 years, and 40% reported providing more than 20 years of care to patients with cardiovascular disease. Eighty-six percent were male and 78% were 60 years old or younger. Eighty-five percent reported receiving dental care within the last year, and 90% reported their oral health as “good” or “excellent.” Eighteen percent had been told that they have periodontal disease. (Table II)
Practice Behaviors and Oral Examinations
Forty-one percent of cardiologists refer patients to a dental facility when they express concerns about their mouth, and 31% refer if they see something that should be further examined. However, 22% never refer patients to a dental clinic or facility. In the past year, 46% of respondents reported referring between 1 to 5 patients to a dental facility due to periodontal disease, and 13% referred more than 6 patients within the last year. Respondents' answers were similar for referring a patient for tooth decay, with 43% referring between 1 and 5 patients to a dental facility for tooth decay, whereas 12% referred 6 or more patients (Table III).
North Carolina Cardiologists' Oral Health Status
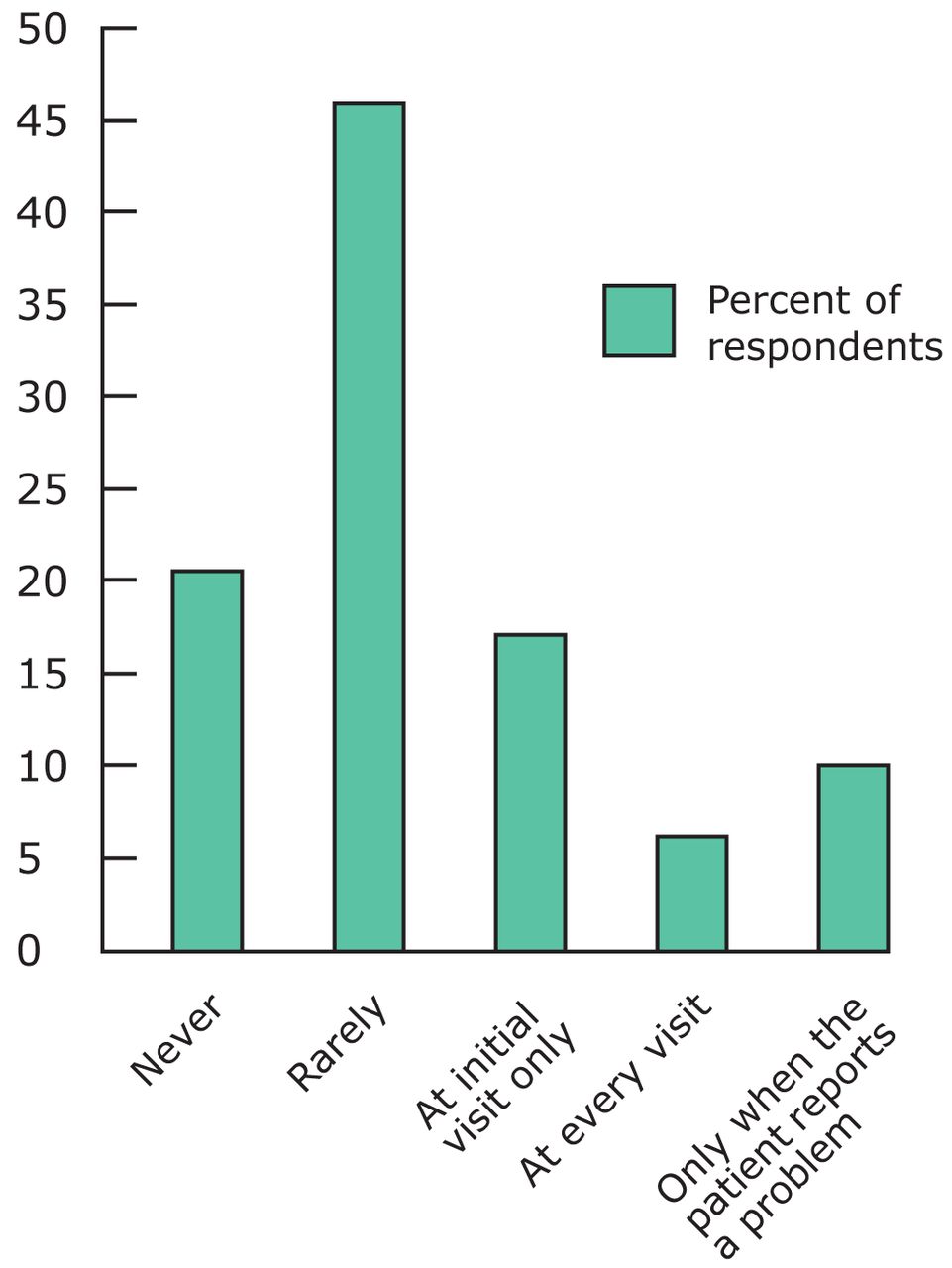
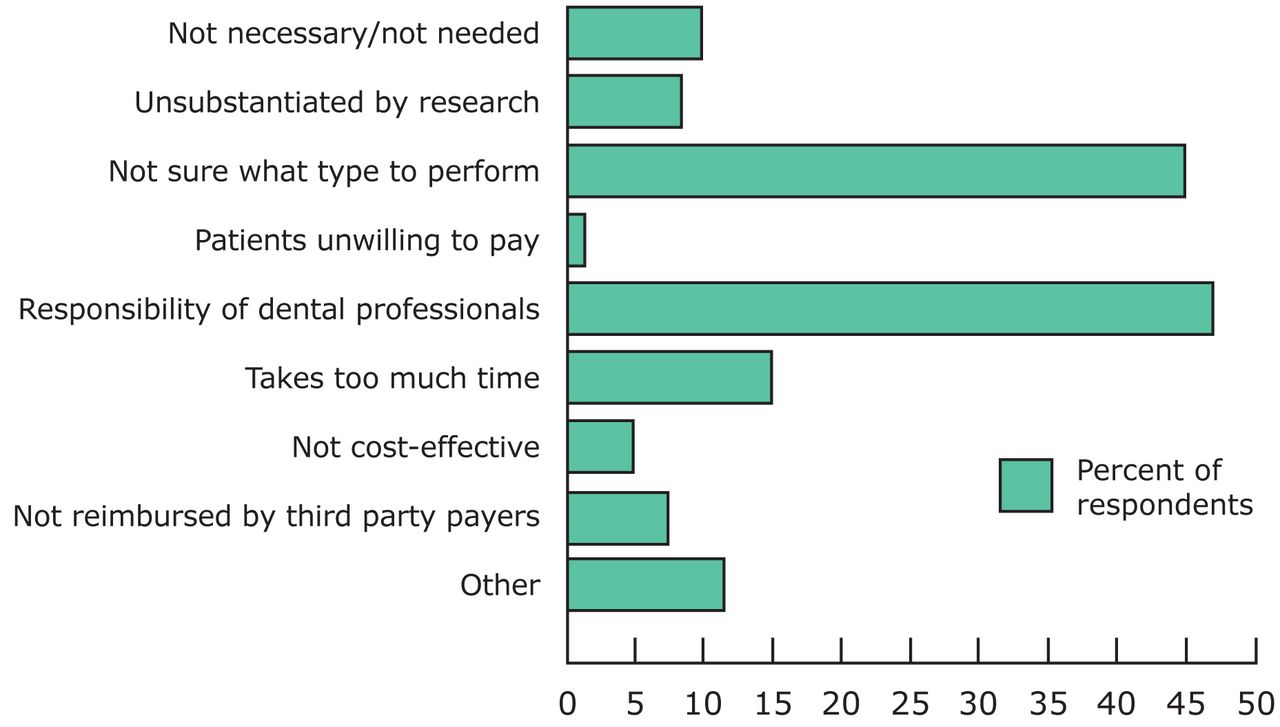
Physicians were asked how often they perform oral examinations on their patients, and 18% responded that they perform an oral exam at the initial visit, while 21% never perform oral examinations on their patients (Figure 1). When asked the reasons for not doing so, 46% responded that it is the responsibility of the dental professional and 45% were not sure what type of exam to perform (Figure 2)
Knowledge and Opinions about Periodontal Disease and Systemic Health
Cardiologists' knowledge about periodontal disease was moderate, with 70% reporting that bone loss describes periodontal disease. Sixty-three percent of respondents answered correctly about the first sign of periodontal disease as being bleeding gums, and 50% were aware that periodontal disease is an infection in the gums. Conversely, 18% described tooth decay as a sign of periodontitis, and 31% recognized reversible redness/inflammation as a clinical indication of periodontitis.
Survey Respondents' Patients with Cardiovascular Disease Referred to Dental Facility within the Past Year
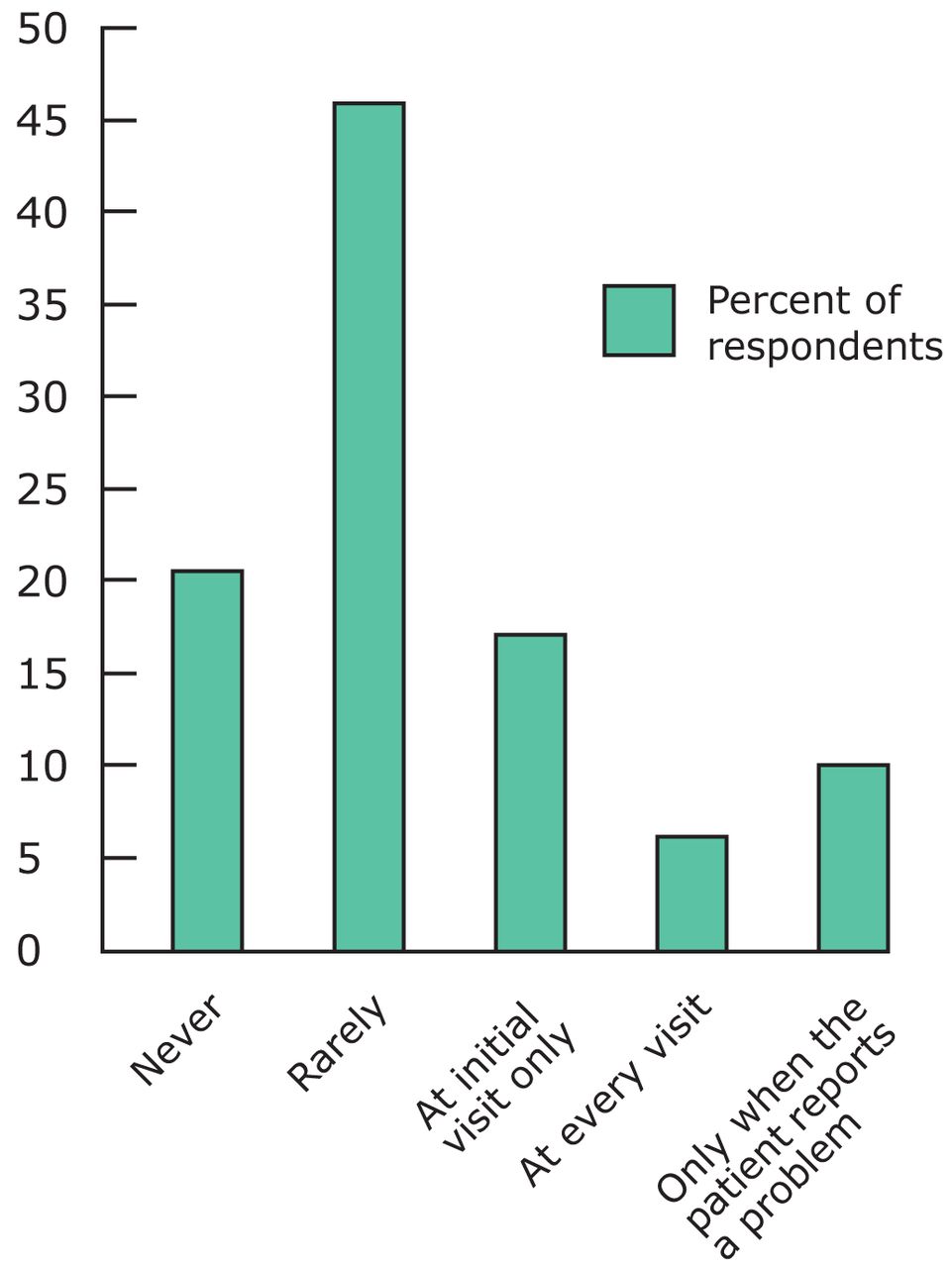
Frequency Survey Respondents Perform Oral Health Exams on Patients with Cardiovascular Disease

Survey Respondents' Reasons for Not Performing Oral Exams
The majority (92%) of cardiologists agreed or strongly agree that inflammation is a key component between periodontal disease and cardiovascular disease, and 66% agree that controlling infection and inflammation is important for managing cardiovascular disease. When asked about their knowledge about the studies regarding an association between cardiovascular disease and periodontal disease, 50% agreed and 50% were unsure or disagreed. When asked if patients with periodontal disease were more likely to have increased atherosclerosis and risk for myocardial infarction and stroke, 72% agreed (Table IV).
Only 39% agreed that treatment of periodontal disease could decrease a patient's risk for cardiovascular disease. However, 72% were interested in learning more about the relationship between cardiovascular disease and periodontal disease. The majority of physicians (71%) agreed it is important for cardiologists' and periodontists to work together to educate their patients about oral systemic disease risks (Table IV).
Cardiologists were asked if they were familiar with the 2009 clinical recommendations regarding the relationship between cardiovascular disease and periodontal disease.17 Sixteen percent were slightly familiar while 78% were not familiar. When asked if these recommendations changed the way they treat their patients, 76% indicated they had not changed procedures. Twenty-two percent of respondents were familiar with the recent 2012 statement from the AHA and 86% said that the statement has not changed their opinion about the importance of oral health to overall health.23
Physicians' Education
Physicians reported that 20% of their professional education included oral health content. However, 80% reported not receiving any education on oral health care. For the majority of physicians who did receive oral health education, 90% received less than 3 hours. Twelve percent reported having clinical requirements regarding assessments of the teeth or gums, while only 5% reported observing a dentist or dental hygienist. When asked to rate the quality of their oral health education, 69% reported it as poor. Sixty percent of cardiologists believe that medical and dental students should be trained to work collaboratively, and 39% responded that “maybe” they should be trained to do so (Table V).
Opinions About Periodontal Disease and Systemic Health
Discussion
This study was the first of its kind to question cardiologists about their knowledge and behaviors regarding periodontal disease and the potential association with cardiovascular diseases. While studies have been conducted with other health care providers, cardiologists have not been investigated.25,26,31,32 It has been determined that individuals who have cardiovascular disease and periodontal disease share many of the same risk factors such, as smoking, diabetes, obesity and age.6,10-17 But how this evidence is translated into the clinical practice of cardiologists has not been studied until this investigation.
There is evidence that periodontal bacteria and the byproducts of the bacteria have a detrimental effect on distant sites.21,22 Although the specific mechanism has yet to be confirmed, scientists agree that there is an association between periodontitis and cardiovascular diseases.23 When other health care providers have been questioned about their knowledge regarding the etiology of periodontal disease, most have some knowledge of the bacteria and their detrimental effects. For example, a recent study of internists and endocrinologists found physicians knew that bacteria was related to the etiology of periodontal disease (86%) and bone loss around teeth is a description of periodontal disease (77%).25 Sixty-six percent knew that bleeding gums were a first sign of periodontitis. But the physicians also thought that tooth decay was a sign of gum disease (30%). The current study found similar results, with 63% of cardiologists reporting bleeding gums as a first sign of disease, and 70% knowing that bone loss is congruent with periodontal disease. Sixty-six percent reported the first sign of periodontitis as bleeding gums, and 18% also thought that tooth decay was a sign of periodontitis. While their knowledge is high in some areas, they are confused in other oral health topics. Most studies of other health care providers have reported that they view their oral health education in professional school as being poor and they are interested in learning more about oral disease.25,26,32
The research team for this study anticipated that more than 16% would be familiar with the guidelines. The most recent statement from the AHA regarding the association of periodontal disease to atherosclerotic vascular disease has gained much attention since it was published in May, 2012; however, the cardiologists in this study did not seem aware of the statement and indicated it had not changed the way they view the importance of oral health. While a cause and effect has not been established between periodontal disease and cardiovascular disease, the statement does support an association between the 2 conditions.23 Clearly more work needs to be done to educate cardiologists about periodontal disease and the potential detrimental effects to systemic health.
The relationship between oral health care providers and medical providers is an area that needs improvement. Wooten et al reported that 62% of nurse practitioners and certified nurse midwives conduct an oral exam as part of routine care at initial visits.26 The current study concluded that only 18% of North Carolina cardiologists' conduct an oral exam at the initial visit. Practitioners stated that it is the responsibility of the dentist to perform the exam. Another reason for not doing an exam is that they simply do not know what it entails. This is an area that could be incorporated into medical school education through interprofessional education.
With an increase in oral systemic disease, it is important to examine the need for interprofessional education. Wilder et al recommended that faculty development, curricular changes and interprofessional education initiatives be incorporated into dental education. Dental schools should seek relationships with local clinics and private practice dentists and other health professionals.33 The paper reinforces the Commission on Dental Accreditation recommendation that states students should be encouraged and participate in service learning (Haden, personal communication, December 2007). Lopes et al reported that only 21% of diabetes educators received formal education on oral health.31 The current study reported similar findings and concluded that while the majority of respondents did not receive oral health education, they believe it is an important area for students to work collaboratively. An interprofessional education curriculum would provide the atmosphere for collaboration to occur.
Physicians' Education Regarding Oral Health
Interprofessional practice can be improved by providing options for continuing education in the area of oral systemic health. Higher education administrators and leaders should begin examining these areas and incorporating them into health professions curricula. In 1989, Rutgers School of Biomedical and Health Sciences began implementing oral health modules into the second, third and fourth years of medical school. Modules in head/neck examination and oral cancer screenings were incorporated into the curriculum along with rotations throughout the dental school to learn more about oral conditions.34 This study, along with other studies, concluded that oral health is an important part of overall health.25,26,31-34 To provide the best care and practices for patients, multidisciplinary fields need to collaborate.
Limitations of this survey include a low response rate. Cartwright investigated response rates of physicians from 19 professional groups. The response rate varied from 56 to 99%.35 Factors affecting response rates included length of questionnaire and the available time to complete it. While the method used for the conduct of the survey was a recommended procedure for survey research,30 it is also recognized that busy physicians may not take the time to complete a longer questionnaire or the physicians may not actually see the survey if they do not review the mail. In addition, this sample of North Carolina cardiologists may not be representative of all cardiologists, thus limiting the external validity. However, the study does provide a view of how oral health is incorporated (or not incorporated) into the clinical practices of cardiologists.
Future studies should investigate how oral health content can be incorporated into the curricula of medical providers. Other studies might evaluate scenarios where oral health care (dentists and dental hygienists) and medical providers work collaboratively in providing patient care.
Conclusion
This study found that North Carolina cardiologists' have some knowledge about periodontal disease but are unclear in other areas. Half of cardiologists' surveyed were unsure that treatment of periodontal disease can decrease a patient's risk for cardiovascular disease. Approximately half of respondents referred 1 to 5 patients to a dental facility for either tooth decay or periodontal disease. Further education in oral diseases will help physicians refer patients to the appropriate oral health care provider. Though North Carolina cardiologists' were not implementing the published clinical recommendations into practice, the majority were interested in learning more about the association between the 2 diseases. Respondents agreed that it is important for health care providers to work together to educate patients on systemic diseases.
Acknowledgments
This project was supported by a grant from the ADHA Institute for Oral Health and the Colgate Palmolive CO.
Footnotes
Megan Mosley, BSDH, MS, graduated in 2013 from the University of North Caroline at Chapel Hill with a Masters in Dental Hygiene Education, and currently works in private practice in Raleigh, NC. Steven Offenbacher, DDS, MS, PhD, is a member of the department of periodontology at UNC School of Dentistry, and is the director of the Center for Oral and Systemic Diseases. Ceib Phillips, MPH, PhD, is a Professor in the Department of Orthodontics at the University Of North Carolina School Of Dentistry. Christopher Granger, MD, is a cardiologist at Duke University. Rebecca Wilder, BSDH, MS, is a Professor and Director of Faculty Development for the University of North Carolina at Chapel Hill School of Dentistry, and also serves as Director of the Master of Science Degree Program in Dental Hygiene Education.
This study supports the NDHRA priority area, Health Promotion/Disease Prevention: Assess strategies for effective communication between the dental hygienist and client.
The Journal of Dental Hygiene Best Paper Award was created to recognize the most outstanding research paper published from the previous year (2014). All original research papers published in 2014 were evaluated by a panel of judges, using specific criteria, to make the final selection. This manuscript first appeared in Volume 88, Issue Number 5 of the October 2014 issue of the Journal of Dental Hygiene.
- Copyright © 2015 The American Dental Hygienists’ Association





{kind=link}
{kind=link}