



Abstract
Purpose: Oral complications are common in children undergoing head and neck radiation and chemotherapy. The purpose of this study is to examine the knowledge, perceived ability and practice behaviors of pediatric oncology and hematology nurses in assisting with the various oral health care needs of pediatric oncology patients and to identify pediatric oncology nurses' previous training/education, practice types and other demographic characteristics that are related to their oral health competencies.
Methods: A survey of a convenience sample of Pediatric Oncology and Hematology Nurses was conducted during the Association of Pediatric Oncology and Hematology Nurses' (APHON) 36th Annual Conference and Exhibit. Descriptive analysis and the exploratory factor analyses were performed using SAS version 9.2 (SAS Institute, Inc., Cary, NC).
Results: Among the 300 surveys that were distributed, 235 surveys were completed (78% response rate) by pediatric oncology or hematology nurses who provide direct patient care in the U.S. Approximately 75% reported receiving less than 3 hours of oral health related education/training. Sixty percent did not have a clinical requirement regarding the assessment of the teeth and gums during their nursing school education. Bivariate analyses indicated that nurses who had clinical requirements regarding oral health assessment during nursing education/training presented greater overall oral health competencies including having greater confidence in examining oral complications than those who did not.
Conclusion: Pediatric oncology nurses' knowledge, perceived ability and practice in assisting patient's oral hygiene care, preventing and managing oral complications vary by topic and might reflect their educational preparedness. This study may provide valuable information pertaining to the need and opportunity for interprofessional oral health care education and collaboration with nursing and dental professionals, in order to increase access to comprehensive oral care for pediatric cancer patients.
Introduction
Information gathered from the National Cancer Data Base (NCDB) and the Surveillance, Epidemiology, and End Results (SEER) registries, both of which collect data relating to the diagnosis and treatment of individuals with cancer, reveal that there were an estimated 13.7 million Americans with a history of cancer alive on January 1, 2012. The population of cancer survivors is projected to increase to nearly 18 million by January 1, 2022.1 Although childhood cancers, from birth to age 14, are considered rare, affecting less than 1% of all new cancer diagnoses, nearly 59,000 Americans are survivors of childhood cancers.1 Improved survival rates are largely due to newly implemented aggressive treatment strategies.2 It is predicted that nearly 80% of children diagnosed with cancer in 1990 will survive into adulthood due to these treatment modifications.2-4 But, these new cures may be associated with long-term effects that have adverse effects on the quality of life of survivors.2
Oral complications, such as mucositis, herpes simplex virus (HSV) infections, erythematous or pseudomembranous candidiasis, xerostomia, dental caries, and dental anomalies are common in children undergoing head and neck radiation and chemotherapy due to compromised immune systems, damage to salivary glands and/or developing dentition.2,5-8 As oral complications persist with chemotherapy or radiation therapy and worsen with prolonged treatment, patients may experience debilitating pain when performing simple tasks, such as eating, drinking and/or talking.5,9 Secondary to this debilitating pain in the mouth and compromised nutrition, patients may also experience delayed wound healing, decreased treatment effects and diminished quality of life.5,10,11
It is widely accepted throughout the literature that basic oral hygiene practices, such as brushing, flossing and using mouth rinses help in reducing the oral microbial flora in the mouth and preventing oral complications associated with the treatment of cancer.12,13 Furthermore, early and radical professional dental intervention reduces the frequency of problems, minimizing the risk for oral and associated systemic complications.14-18 Therefore, it is recommended that all newly diagnosed pediatric oncology patients seek early dental consultation to allow adequate time for necessary dental care to be completed prior to initiating cancer therapy and continue to place emphasis on preventive interventions.14
Nurses are often frontline clinicians who triage outpatient's conditions and needs and spend more time with inpatients and their families than do physicians. In the pediatric oncology unit, nurses may firsthand see the incidence of oral complications that may affect patients' quality of life and treatment success.10 Baseline surveys from 2 demonstration projects, whose purpose was to eventually develop an oral care protocol for use in cancer care units in the U.S., indicated that nurses were capable of identifying simple oral complications, such as mucositis and oral candidiasis, but were not able to diagnose more severe oral complications, such as xerostomia.19,20 These studies also found that the nurses lacked current knowledge on oral care recommendations for pediatric oncology patients and were not performing oral assessments and referrals on a regular basis.
It is important to determine the need and opportunity for interprofessional oral health care education and collaboration in order to increase access to comprehensive oral care for pediatric cancer patients. Therefore, the purpose of this study was to examine the knowledge, perceived ability and practice behaviors of pediatric oncology and hematology nurses in assisting with the various oral health care needs of pediatric oncology patients and to identify their training/education, practice types and other demographic characteristics that are related to their oral health competencies.
Methods and Materials
This cross-sectional survey research study was approved by the Biomedical Institutional Review Board of the University of North Carolina at Chapel Hill (UNC-CH). The survey instrument was developed with input from questionnaires used in 2 previous studies,19,20 input from 3 committee members (1 pediatric dentist, 1 general dentist and 1 dental hygienist), a survey methodology consultant from the H.W. Odum Institute for Research in Social Science at UNC-CH, and the recommendations set forth by the American Academy of Pediatric Dentistry (AAPD).21 The survey included 21 questions that solicited demographic and practice information; knowledge, practice behaviors, and their reported confidence to assist with the oral health care needs of pediatric oncology patients, which were intended to measure the nurses' oral health competencies. The survey instrument was pilot tested by 2 pediatric oncology nurses and their suggestions were incorporated in the final survey. A scannable TeleForm questionnaire was developed by the UNC School of Dentistry Data Coordinating and Statistical Consulting Unit to reduce potential entry errors.
Three hundred surveys were distributed to a convenience sample of nurses at a booth in the exhibit hall during the Association of Pediatric Hematology and Oncology Nurses' (APHON) 36th Annual Conference and Exhibit on October 4 to 6, 2012 in Pittsburgh, Pennsylvania. The APHON is a professional organization for pediatric hematology/oncology nurses and allied health care professionals, and it currently has approximately 3,381 active members. By the last day of the conference, 272 surveys were returned.
Data Analysis
The data were analyzed using SAS version 9.2 (SAS Institute, Inc., Cary, NC). Frequencies were computed to summarize demographics and practice characteristics as well as knowledge, confidence and practice behaviors of pediatric oncology nurses with regard to oral health. Exploratory factor analysis was used to identify the factor pattern and domain of question items measuring the nurses' oral health competencies. Chronbach's alpha ranged from 0.7 to 0.95 for the 6 domains identified for nurses' perceived ability and practice behaviors. Among 5 oral health related knowledge questions shown in Figure 1, the knowledge items listed as “daily inspection of mouth by caregivers,” “use of fluoridated toothpaste” and “referrals to a dentist prior to cancer therapy” appeared to form a domain, thus included in the further analysis. Bivariate analyses were conducted with the Mantel-Haenszel test to identify the pediatric oncology nurses' previous training/education, practice types and other demographic characteristics that were associated with the 7 domains of oral health competencies, with statistical significance set at p<0.05.
Results
Of the 272 surveys that were returned, 235 surveys were completed by those who are currently employed as a pediatric oncology, pediatric oncology or hematology nurse, giving a response rate of 78%. The demographic and professional characteristics of the survey respondents are summarized in Table I. The majority of the respondents were women (97%) and reportedly work 36 hours or more a week (70%). Slightly more than half of respondents work as certified pediatric oncology/hematology nurses and have been employed as a pediatric oncology nurse for 10 or more years (54% and 53%, respectively). Approximately 75% of the respondents reported receiving 3 hours or less of education and/or training related to oral health care in nursing school, and about 60% did not have a clinical requirement regarding the assessment of the teeth and gums during their nursing school education. While 91% of survey respondents expressed a desire to take continuing education (CE) courses relating the oral health care for pediatric oncology patients in the future, only 25% had taken such a CE course in the last 5 years.
Knowledge
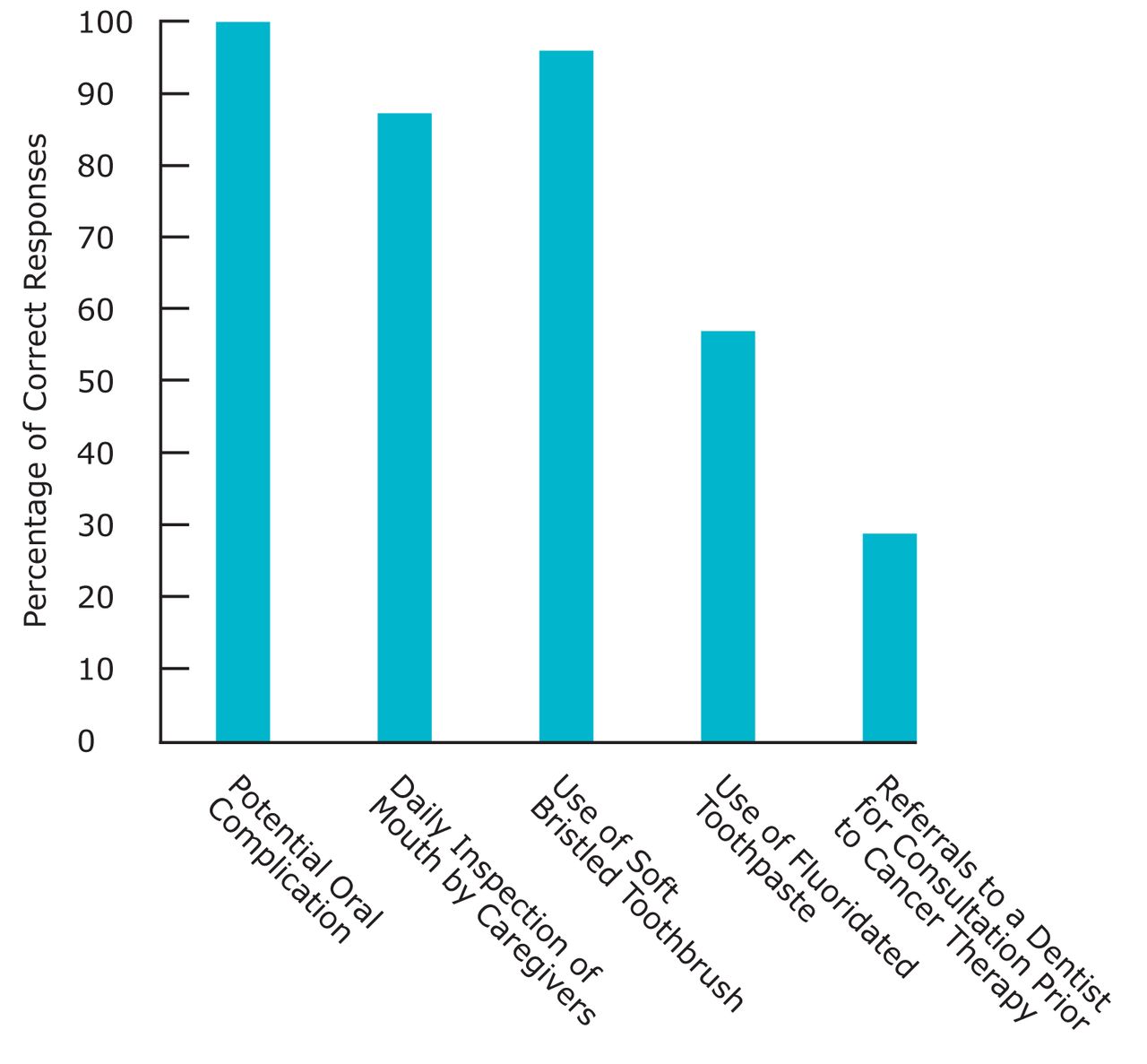
The majority of respondents were aware of potential oral complications related to cancer treatment (100%) and professional oral health care recommendations for pediatric oncology patients such as the use of a soft bristled toothbrush (97%) and daily inspection of the child's mouth by his/her caregivers to determine the presence or absence of oral complications (87%) (Figure 1). However, the use of fluoridated toothpaste and referrals to a dentist for consultation prior to cancer treatment received lower rates of correct responses (57% and 29%, respectively). Overall, only 14% of survey participants responded correctly to all informative questions that assessed their knowledge of oral health care recommendations for pediatric oncology patients undergoing cancer treatment.
Perceived Ability
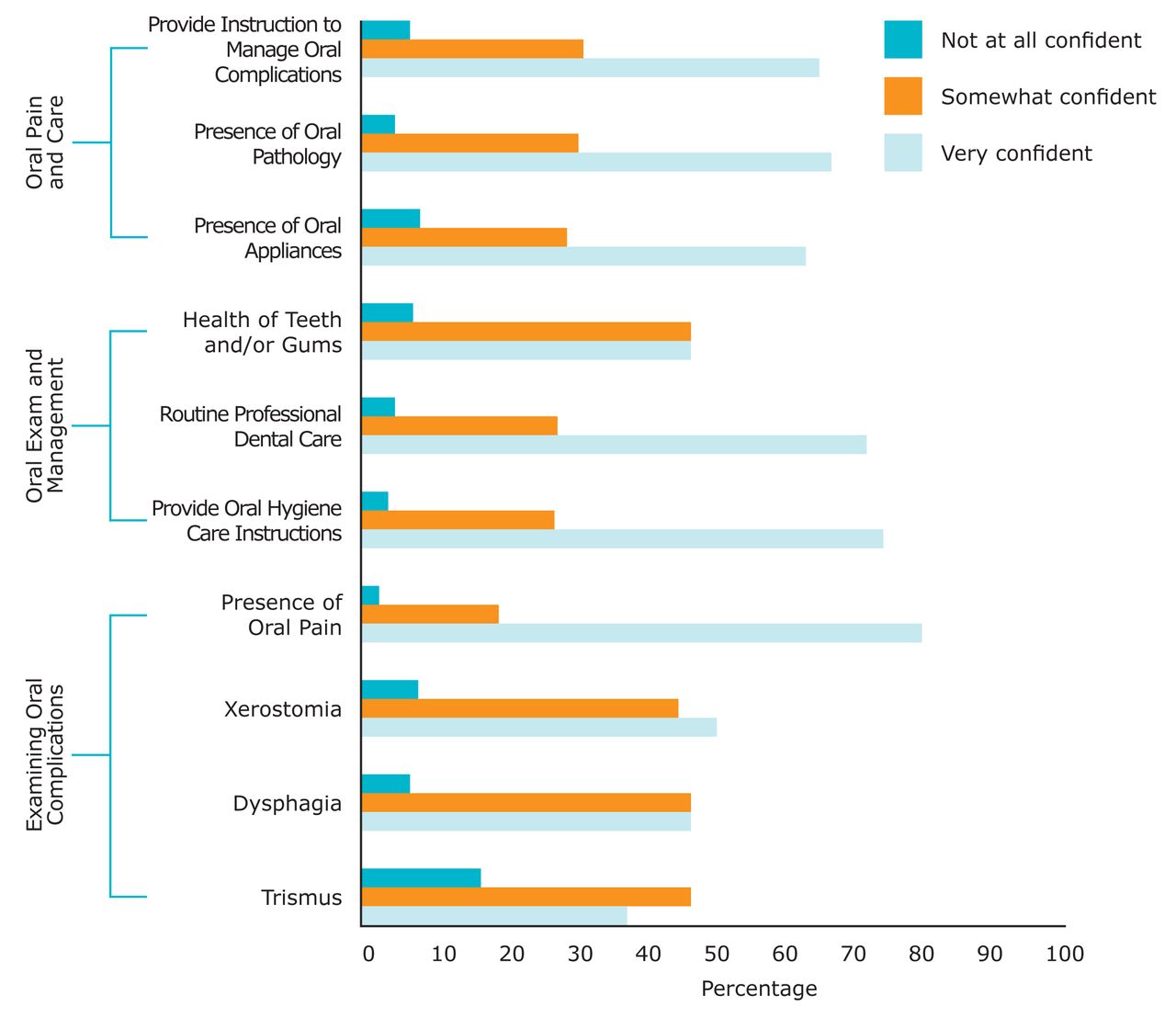
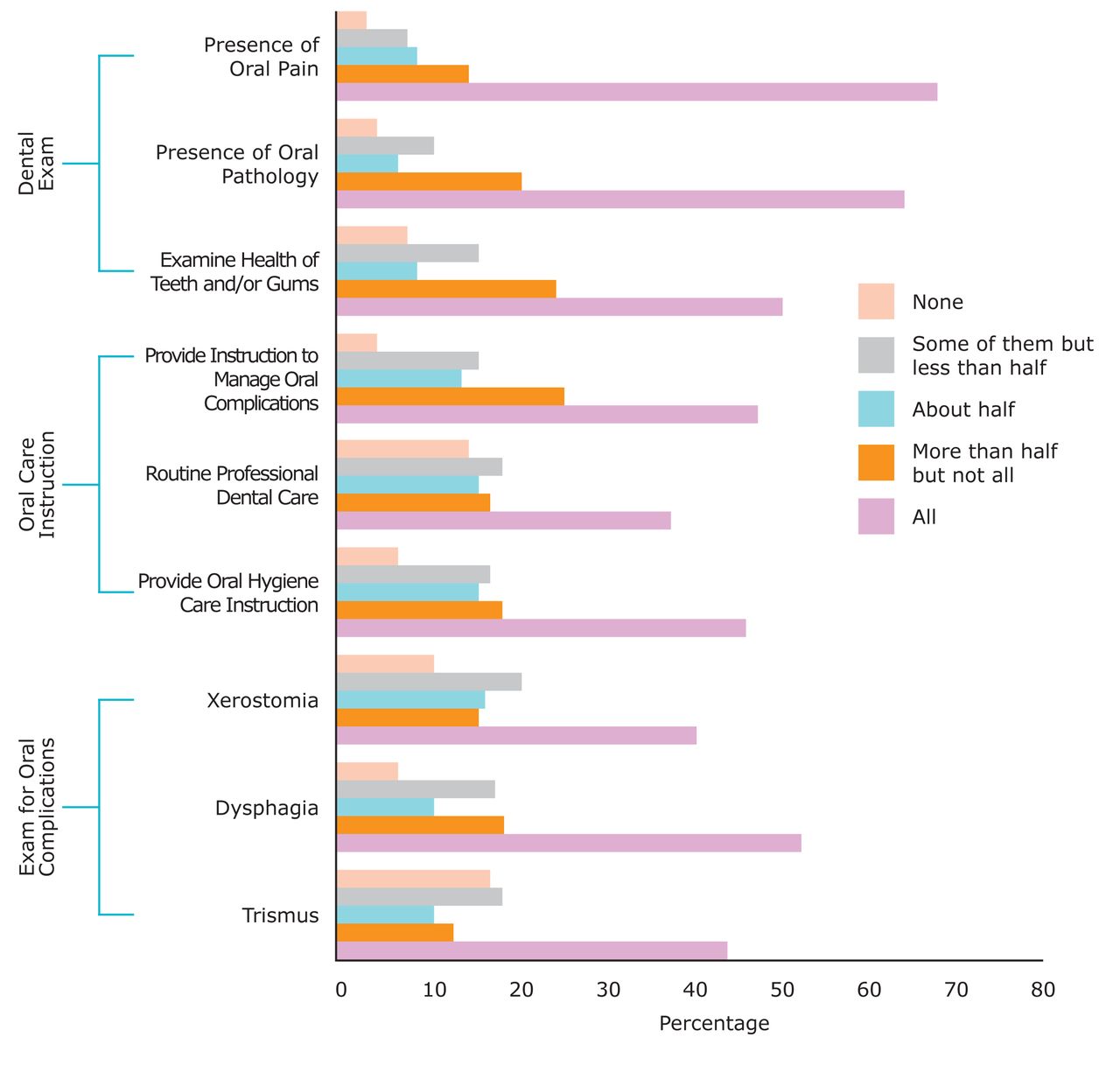
The majority of the respondents reported that they are comfortable performing oral procedures on patients (77%), and are adequately trained to provide oral health care instructions/education to patients (72%) and to perform oral care procedures (84%). When asked about their level of confidence in performing various oral health related tasks for pediatric oncology patients, more than 70% of survey respondents were reportedly very confident in examining for the presence of oral pain, providing oral hygiene instructions, and discussing the importance of seeking routine professional dental care (Figure 2). However, less than half of respondents reported that they were very confident in their ability to examine the health of teeth and gums for complications of trismus, dysphagia, and xerostomia.
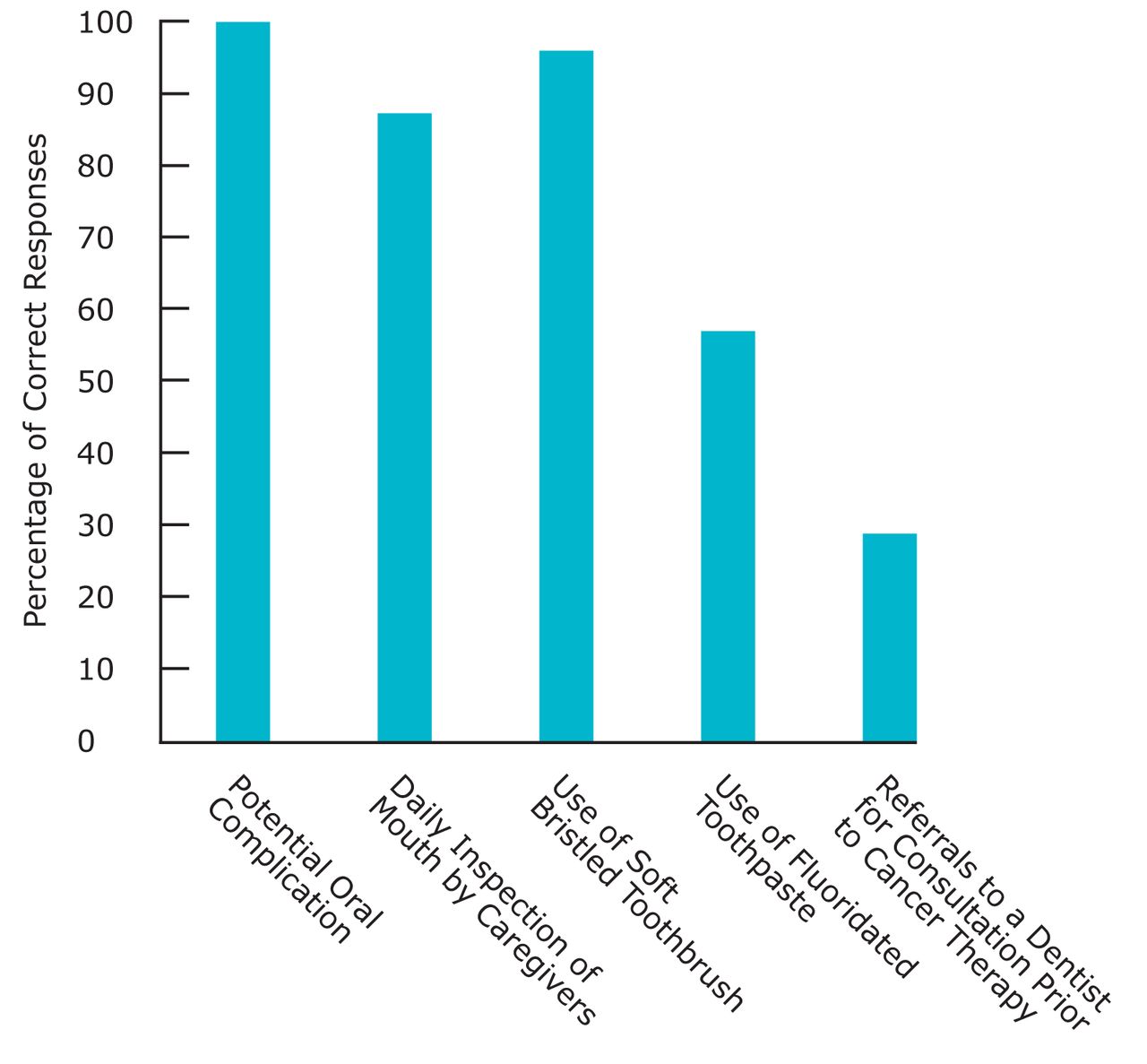
Knowledge of Oral Health Care Recommendations for Pediatric Oncology Patients among Survey Respondents (n=235)
Practice Behaviors
While more than 60% of respondents reported examining all of their patients for the presence of oral pathology or oral pain (63% and 69%, respectively), about half of survey participants examine all of their pediatric oncology patients' teeth and/or gums, detect dysphasia, and provide instructions for oral hygiene care and management of oral complications (Figure 3). Only about 40% or less of respondents reported examining all patients for the presence of xerostomia, trismus, and discussing the importance of seeking routine professional dental care.
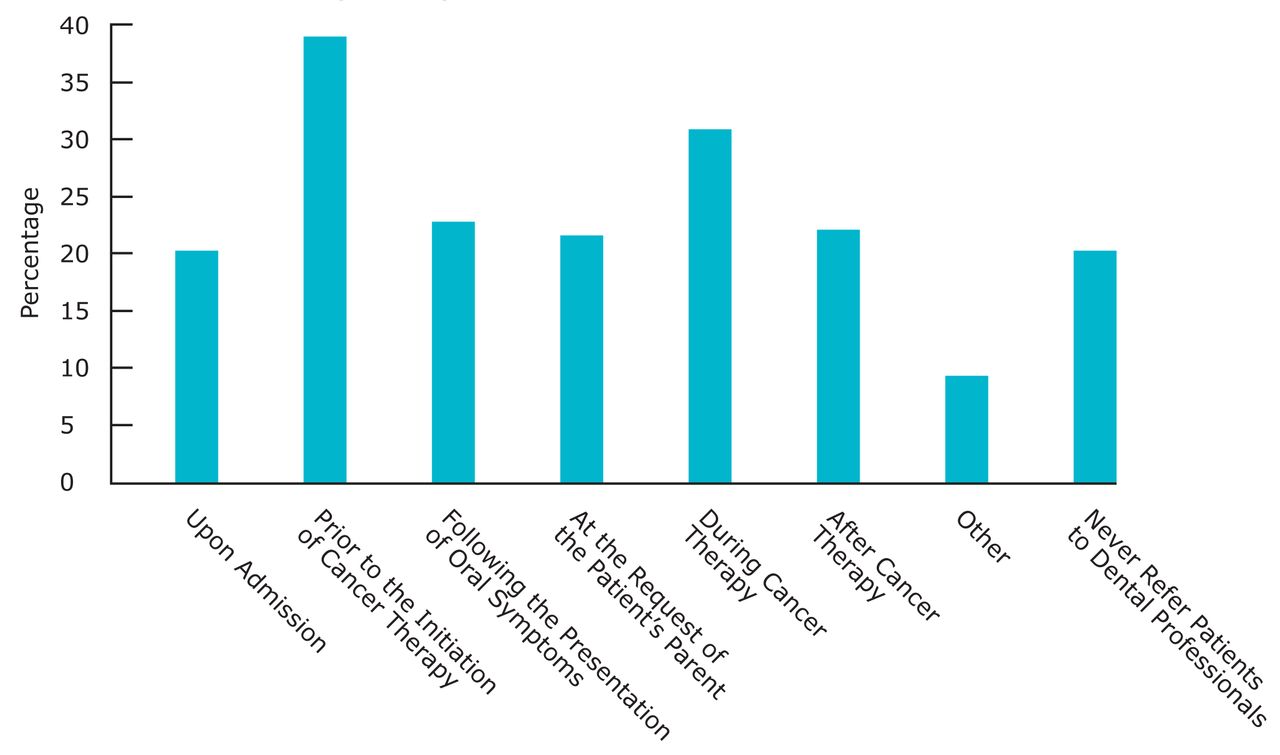
Figure 4 shows survey respondents' practice of patient referrals to dental professionals. More than one-third of survey respondents reported referring patients to dental professionals prior to the initiation of cancer treatment and/or during cancer treatment (39% and 31%, respectively). Twenty percent of survey respondents reported never referring patients to dental professionals.
Oncology Nurses' Demographic Characteristics and Oral Health Competencies
Extracted outcomes of bivariate analyses are shown in Tables II, III and IV. Overall, nurses' characteristics such as having had a clinical requirement regarding oral health assessment during nursing education/training, having taken oral health related CE courses in the past 5 years, and number of years worked as a pediatric oncology nurse were associated with domains of oral health competencies. Survey respondents who had a clinical requirement regarding oral health assessment during nursing education presented greater oral health related knowledge and confidence in examining patient's mouth, detecting oral complications and providing oral care management while they were also likely to provide oral care instructions and examine the patient's mouth more often than those who did not (p<0.02). History of having taken an oral health related CE course in the past 5 years was associated with all domains of oral health competencies except for the domains of practice of and confidence in examining for oral complications (p<0.007). The level of oral health related knowledge, confidence and practice were greater among survey respondents who worked as a pediatric oncology nurse for a longer time than those with a shorter history of specialty practice (p<0.05). However, no difference was observed in the confidence in and practice of examining for oral complications such as xerostomia, dysphagia and trismus with the length of professional work experience as a pediatric oncology nurse (p>0.1). More nurses who work full-time in direct patient care and have a source for dental referrals responded to oral health knowledge questions correctly than those who don't work full-time in direct patient care. Job title, such as whether they were a certified oncology nurse or not, as well as hours spent in oral health education/training during nursing school were not associated with oral health competencies.
Discussion
This study identified gaps in pediatric oncology nurses' knowledge, confidence and practice in assisting with the oral health care needs of their patients, depending on the area of oral health topic assessed and the survey respondents' educational background. In conjunction with the findings from previous studies, the data implied that pediatric oncology nurses are learning in the field about oral health and oral complications among pediatric oncology patients as opposed to having been formally trained in this health knowledge area in nursing school. Most of the survey respondents reported having received less than 3 hours of formal training and/or education relating oral health care, nor did they have a clinical requirement regarding the assessment of the teeth and/or gums, while in nursing school. This study revealed that overall oral competencies were greater among individuals who had worked longer as an oncology nurse.
Demographic and Professional Characteristics of the Survey Participants (n=235)*
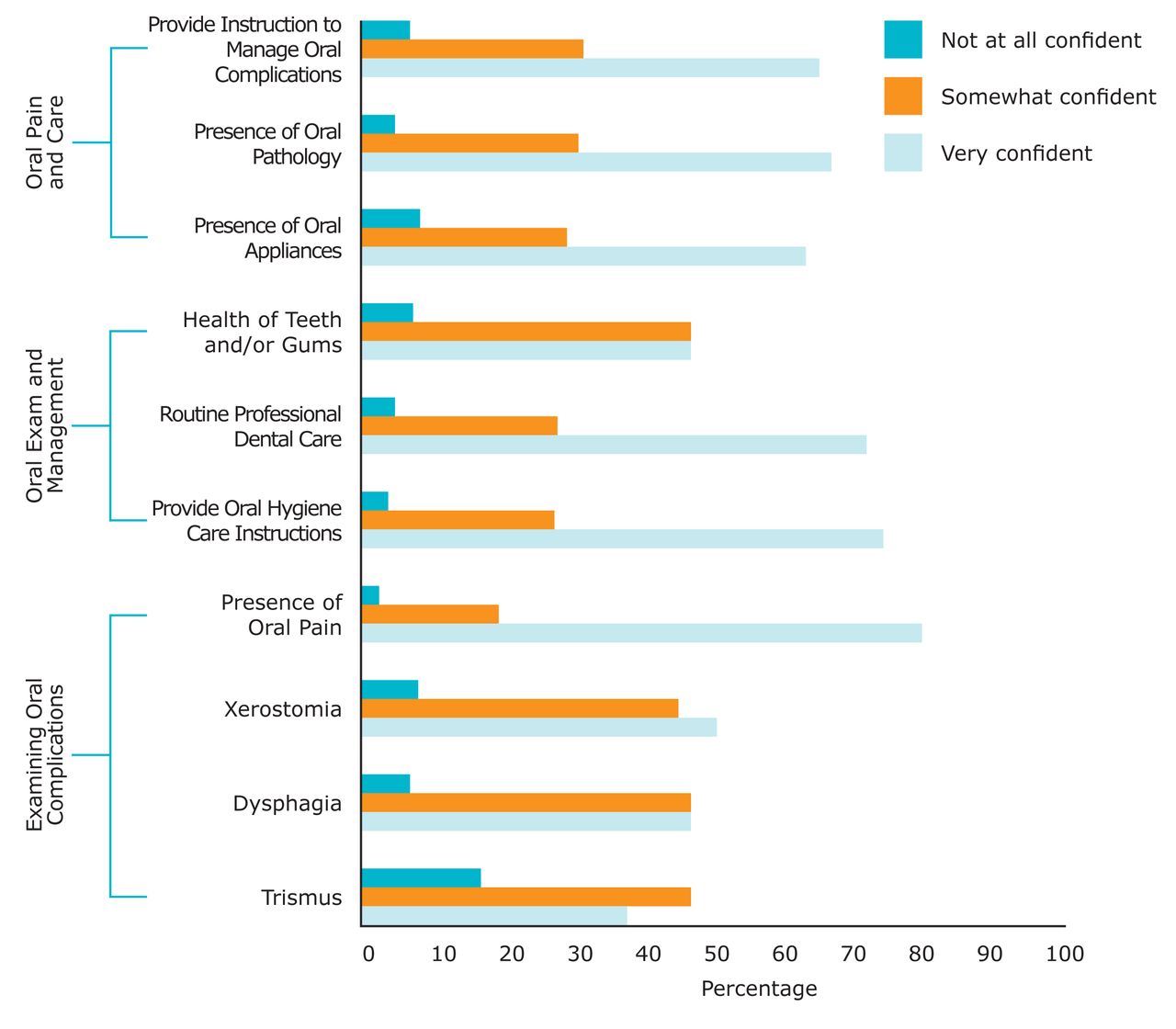
Perceived Ability in Performing Oral Health Related Tasks on Pediatric Oncology Patients among Survey Respondents (n=235)
Response rate of 78% (235/300)
Previous studies have surveyed internists and endocrinologists, nurse practitioners and nurse midwives, and diabetes educators to determine their knowledge, opinions and behaviors regarding periodontal disease and adverse health outcomes.22-24 Owens et al found that internists and endocrinologists knowledge about periodontal disease was high, but they lacked training and education relating to periodontal disease and oral health care.22 Wooten et al found that nurse practitioners and certified nurse midwives had limited knowledge about periodontal disease and oral health care.23 Lopes et al found that the majority of diabetes educators had no formal education and/or training related to oral health care, nor did they have any continuing education once they began their careers.24 All 3 studies suggested that a collaborative effort between health care providers and dental professionals would positively benefit patients in various areas of the healthcare system.22-24
While on-the-job training or taking CE courses may improve oncology nurses' confidence and practice behavior of providing oral exams and oral care instructions over time, the data suggests that these factors may not sufficiently improve confidence and practice related to oral complications among nurses. Confidence and practice behaviors related to examination for oral complications (i.e. xerostomia, dysphagia, trismus) were greater among survey respondents who had oral health related clinical requirements during nursing school than those who did not. Previous studies also found that while nurses could readily identify simple oral complications, they could not diagnose or treat more severe oral complications prior to the implementation of a structured oral health protocol and receiving additional training in children's hospitals.19 These findings thus indicate the importance of incorporating oral health education and/or training into nursing schools' curricula and finding innovative ways to motivate nurses to adhere to evidence-based oral health care recommendations for pediatric patients who undergo cancer treatment. Although only less than 25% of survey respondents reported having taken a CE course relating to oral health care in the last 5 years, it is encouraging that almost all survey participants (91%) desire to take a CE course relating to oral health care in the future.

Frequency of Performing Oral Health Related Tasks on Pediatric Oncology Patients among Survey Respondents (n=235)
Response rate of 78% (235/300)

Stage in Which Survey Respondents Usually Refer Pediatric Oncology Patients to a Dental Professional (n=235)
Response rate of 78% (235/300)
Percentages do not add up to 100% because multiple choices were given
The Institute of Medicine (IOM) report in 2011, Advancing Oral Health in America, states that “Nurses, physicians, and other health care professionals have generally not been trained in providing oral health services or screenings. In addition, dental professionals are generally educated and trained separately from other health care professionals, which reinforces the separation of care as well as lack of training in appropriate referrals between professionals.”25 As the complexity of health care continues to increase, it has been recommended that health care providers learn to work more collaboratively in order to provide quality care.26 It has been shown that interprofessional collaboration, with nursing and dental professionals, positively affects quality of care, patient satisfaction, effectiveness of health care services, health care costs and communication among health care professionals.26-28 In order to improve compliance with evidence-based recommendations, perceived abilities and practice behaviors of pediatric oncology nurses as related to oral health care, an interprofessional approach with emphasis placed on implementing an oral health care protocol and continuous staff education and training at each pediatric oncology unit might be important.
Strengths of this study include the broader geographic representation of pediatric oncology and hematology nurses. While 2 similar previous studies surveyed pediatric oncology nurses in local institutions, the current study was able to capture nurses from various geographic regions, which was identified by the mailing addresses respondents placed on the raffle tickets. Respondents also included those with various certifications and differing educational backgrounds and training. The limitation of this study includes missing data found in various sections of the survey which made performing multivariable analysis infeasible. Furthermore, the attendees of the professional meeting may be more involved in educational activities than those who do not attend. Therefore, the findings of this study may not be representative of all U.S. pediatric hematology and oncology nurses nor all the member of the APHON professional organization. Lastly, although the study identified several domains related to oral health knowledge, perceived ability and practice behaviors in assisting pediatric oncology patients, there was no validated tool available to measure oral health competencies of oncology nurses when we conducted this study. Despite this, we provided initial evidence of the domains of oral health competencies among pediatric oncology nurses and gained insight into the type of demographic characteristics of nurses that may influence their knowledge, confidence and practice behaviors in assisting child patients' oral health needs.
Quantile for Domain of Oral Health Related Knowledge by Survey Respondents' Background Characteristics (n=235)
Quantile for Domains of Confidence in Performing Oral Health Related Tasks by Survey Respondents' Background Characteristics (n=235)
Quantile for Domains of Performing Oral Health Related Tasks by Survey Respondents' Background Characteristics (n=235)
Conclusion
Pediatric oncology nurses' knowledge, perceived ability, and practice behaviors in assisting patient's oral hygiene care and preventing and managing oral complications vary by topic and might reflect their educational preparedness. Interprofessional collaboration between dental and nursing schools in provider training as well as institutional efforts in implementation of evidence-based oral health practices might be needed in order to improve pediatric cancer patients' and survivors' oral health.
Footnotes
Antiana Perry, BSDH, MS, completed this project in partial fulfillment of the Master of Science degree in Dental Hygiene Education at the University of North Carolina Chapel Hill School of Dentistry. Hiroko Iida, DDS, MPH, is currently a director of the New York State Oral Health Center of Excellence and was an assistant professor at UNC Department of Pediatric Dentistry when this study was conducted. Lauren Patton, DDS, is a Professor and Department Chairperson of the Dental Ecology Department. Rebecca S. Wilder, RDH, MS, is a Professor and Director of Graduate Dental Hygiene Education and also Director of Faculty Development at the University of North Carolina Chapel Hill School of Dentistry.
This study supports the NDHRA priority area, Health Promotion/Disease Prevention: Validate and test assessment instruments/strategies/mechanisms that increase health promotion and disease prevention among diverse populations.
- Copyright © 2015 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}
{kind=link}