



Abstract
Purpose: The purpose of this article is to discuss the impact of the training program for predoctoral dental and hygiene students at Loma Linda University School of Dentistry (LLUSD) with regard to issues related to treating patients with a high risk of having HIV/AIDS.
Methods: LLUSD offers a training program for fourth-year dental hygiene and predoctoral dental students that addresses the oral health care needs of persons with HIV disease. The training occurs in small groups 2 days per week at a community clinic serving HIV-positive individuals. Three academic quarters are required to train all fourth-year students each year. Evaluation of program effectiveness is conducted by means of pre- and post-session surveys. Dental hygiene and dental students completed the pre-survey during the spring quarter of their third year in public health dentistry courses. The same students completed the post-session survey at the end of their weekly training sessions during the fourth year.
Results: The overall change in all areas related to the students' comfort level in treating patients in the 3 defined categories is in a positive direction (p-value<0.0001). The change was much higher among dental hygiene students compared with predoctoral dental students.
Conclusion: A comparison of pre- and post-session surveys reveals a significant improvement in students' perception of and comfort level with treating patients who are homosexual/bisexual or intravenous drug users, or who have a history of blood transfusion in both student groups upon completion of the HIV and the Dentist training program at LLUSD.
Introduction
Dentists and dental hygienists see many medically compromised patients in need of care with conditions and personal histories that pose management challenges and that could potentially expose health care professionals, office staff and other patients to risks associated with infectious diseases. Such patients must be given oral health care that addresses their needs and personal conditions, while simultaneously minimizing risk in the office environment. Such management was greatly simplified with the adoption of the approach of treating all patients as potentially infectious. The Center for Disease Control and Prevention (CDC) first issued guidelines for isolation precautions (termed Universal Precautions) to be used with patients known to have or suspected of having an infectious disease in 1983.1 In 1987, the guidelines for preventing HIV transmission in health-care settings were expanded, requiring blood and body fluid precautions to be used with all patients, regardless of their bloodborne infection status.2 These guidelines were updated and expanded in 1996 and 2007, and are now referred to as Standard Precautions.3
Due to the surgical nature of most dental treatment, the potential for exposure to bloodborne pathogens due to percutaneous injuries and mucosal splash is considerable. Of particular concern in the dental clinic are patients with HIV/AIDS. A higher risk of HIV transmission is associated with homosexual/bisexual individuals, intravenous drug users and persons with a history of blood transfusion; however, there are no patients who can be identified to have no risk of transmission. The Standard Precautions addresses this issue with the mandate that everyone be treated as a potential source of infection.4,5
The CDC reports that from 2005 to 2008, HIV incidence in the U.S. has grown slowly and steadily from 37,000 to 42,000.6 The annual number of deaths attributable to HIV/AIDS amounts to approximately 15,500.7 Effective antiretroviral medications and disease management are allowing more people with HIV disease to live longer with what can now be managed by many as a chronic condition.8
The issue of health care professionals' comfort with and willingness to treat HIV patients is not confined to the U.S. alone - it is a global concern. According to Marcus et al, 20% of HIV patients in the U.S. were unable to obtain dental treatment in the past 6 months due to socio-economic status in addition to their medical condition.9 In a more recent study, Myers et al report of a survey indicating that nearly 9% of students were unwilling to perform dental procedures on patients with HIV.10 A survey study conducted in Canada reports that 16% of dentists would refuse to treat HIV patients because they lack a belief in ethical responsibility and fear cross-infection.11 A report was published in Thailand on a survey distributed to patients with HIV who needed dental treatment; 40.9% of patients reported that they failed to disclose that they had HIV in order to obtain the requisite dental care.12 Meanwhile, in a study conducted by Giuliani et al, general dentists in Italy stated that dentists discriminate against patients with HIV.13 Moreover, the literature indicates that many dentists tend to avoid treating patients with HIV.14,15
Several studies found that students lacked knowledge regarding infection control when treating HIV patients; this lack of knowledge was clearly needed to be addressed by means of educational programs.16-18 The Loma Linda University School of Dentistry (LLUSD) recognized the need for providing dental hygiene and predoctoral dental students with additional training related to treating patients with HIV disease. The HIV and the Dentist program was instituted in 2003 to provide all fourth-year students with training in a community dental clinic with a large HIV-positive clientele. This training includes the epidemiology and pathology of the disease, as well as dental treatment considerations and sociological and behavioral aspects. A considerable effort is made to present technical health care management information along with an appreciation of the basic humanity of HIV-positive individuals. The intent of the program is to teach students how to manage patients with this disease, reduce the risk of transmission of the infection to others in the dental office and decrease the stigma associated with treating such individuals among health care providers.
The aim of the present study is to evaluate the effectiveness of the LLUSD program in reducing students' concerns related to treating patients identified with a high risk of having HIV/AIDS.
Methods and Materials
LLUSD developed the HIV and the dentist program to help students manage the oral health care needs of persons with HIV disease. The program components have been published elsewhere.19,20 The training occurs in small groups of 5 to 7 over a 2 half-day sessions. The student in each group spends a total of 8 hours during 1-week periods in the HIV training program at the community clinic. Three academic quarters are needed to train all fourth-year students each year. Evaluation of program effectiveness is conducted by means of pre- and post-session surveys, which were identical for the dental hygiene and the dental students. The survey questions were developed with the assistance of staff of the Behavioral Health Program at the Social Action Community Health System (SACHS). Dental hygiene and dental students completed the pre-survey at the beginning of the training program during the spring quarter of their third year in public health dentistry courses. The same students completed the post-session survey at the end of their weekly training sessions during the fourth year. Both surveys were collected by the secretary of the Department of Dental Education Services. The surveys contained 5 statements regarding:
HIV general knowledge
Attitudes towards the HIV-positive clientele
Comfort with treating this group
Confidence in the effectiveness of universal precautions and post-exposure prophylaxis following bloodborne exposures
A self-assessment of an understanding of the issues involved
Students' comfort level with treating the HIV group is addressed by the following 3 questions:
How do you feel about treating homosexual/bisexual individuals
How do you feel about treating intravenous drug users
How do you feel about treating patients with a history of blood transfusion
Participants scored questions on a 5-point Likert scale as follows: 1=very uncomfortable, 2=uncomfortable, 3=Neutral, 4=comfortable and 5=very comfortable.
Six years of pre- and post-session survey results (composed of 5 overlapping 2-year cycles) are reported in this article. The surveys were distributed to 414 dental students and 197 dental hygiene students from 2003 to 2009. All the students completed the pre-test survey. However, 337 dental students and 172 dental hygiene students (a total of 549 students, or 89.85% of students) completed the post-session survey. A statistical analysis was conducted on the completed pre-post questionnaire for the same participants. Slight modifications were made to the surveys, but the general content remained the same. We did not include questions related to demographics in the early cycles, but we did include these later on. Those dental/hygiene students who did not complete post-training questionnaires were excluded from the analysis. Descriptive statistics were generated, including means. The normality distributions were depicted in histograms and assessed by means of Kolmogorov-Smirnov normality tests. Given the nature of the data, the non-parametric Wilcoxon signed-rank test analyzed was performed on data recorded in pre-session and post session surveys. A p-value<0.05 was considered statistically significant.
Percentages of the Comfort Levels of Predoctoral Dental Students Regarding Treatment of Different Categories of High-Risk Patients
Percentages of the Comfort Levels of Dental Hygiene Students Regarding Treatment of Different Categories of High-Risk Patients
The data were analyzed with a proportional odds model. This model is used for cases in which an ordered categorical dependent variable is present; in this particular case, students' comfort level with each high-risk group at the end of the program can be identified as the ordered categorical dependent variable. The explanatory variables were baseline comfort level, student level (DDS, dental hygiene), and cohort (2003 to 2005, 2004 to 2006, 2005 to 2007, 2006 to 2008, 2007 to 2009). We collapsed categories of combined “very uncomfortable” and “ uncomfortable” into one due to low count in “very uncomfortable.” In addition, a 5-point scale did not show a difference when compared with a 4-point scale; hence, the 5-point scale was changed to a 4-point scale for the analysis purpose. The interaction term between student level and cohort was statistically significant. The evidence suggests that student level (DDS and dental hygiene combined) affects the comfort level differently in the cohort (5 cycles). A separate proportional odds model for each student level was conducted (one for the DDS and the other for dental hygiene). The model's goodness of fit was also examined. All statistical analysis was conducted using SAS 9.3.
Results
In reviewing the post-session survey data after participation in the HIV and the dentist training program, the Wilcoxon signed-rank test showed changes in all categories that were highly statistically significant at a p-value<0.0001 (Tables I and II).
Association between Baseline Comfort Level with Regards to Treating Homosexual/Bisexual Individuals and Comfort Level at the End of the Program as an Outcome
Association between Baseline Comfort Level with Regards to Treating IV Drug Users and Comfort Level at the End of the Program as an Outcome
In a proportional odds model with comfort level with treating HIV patients as the outcome variable, baseline comfort was found to have a significant positive association with the outcome (odd ratio (OR) 37.17, 95% confidence interval (CI) 22.82 to 60.55), and dental hygienists were more likely to be comfortable with treating HIV patients compared with pre-doctoral students (OR 2.50, 95% CI 1.61 to 3.89) (Table III). The results did not differ when each student level was examined separately. For both student groups, the baseline had a significant positive association with the students' comfort level at the end of the program. In other words, students who felt comfortable with treating HIV patients initially were more likely to feel more comfortable with and more confident about treating the same group of patients after completing the program.
Association between Baseline Comfort Level with Regards to Treating Patient with Histories of Blood Transfusion and Comfort Level at the End of the Program as an Outcome
The results were similar for IV drug users and patients with a history of blood transfusion (Tables IV and V). In both, a significant positive association with the comfort level was found (OR 20.48, 95% CI 14.04 to 29.90 for IV drug users, and OR 239.91, 95% CI 83.23 to 691.53 for patients with a history of blood transfusion). Dental hygienists were also more likely to be comfortable with treating these patients.
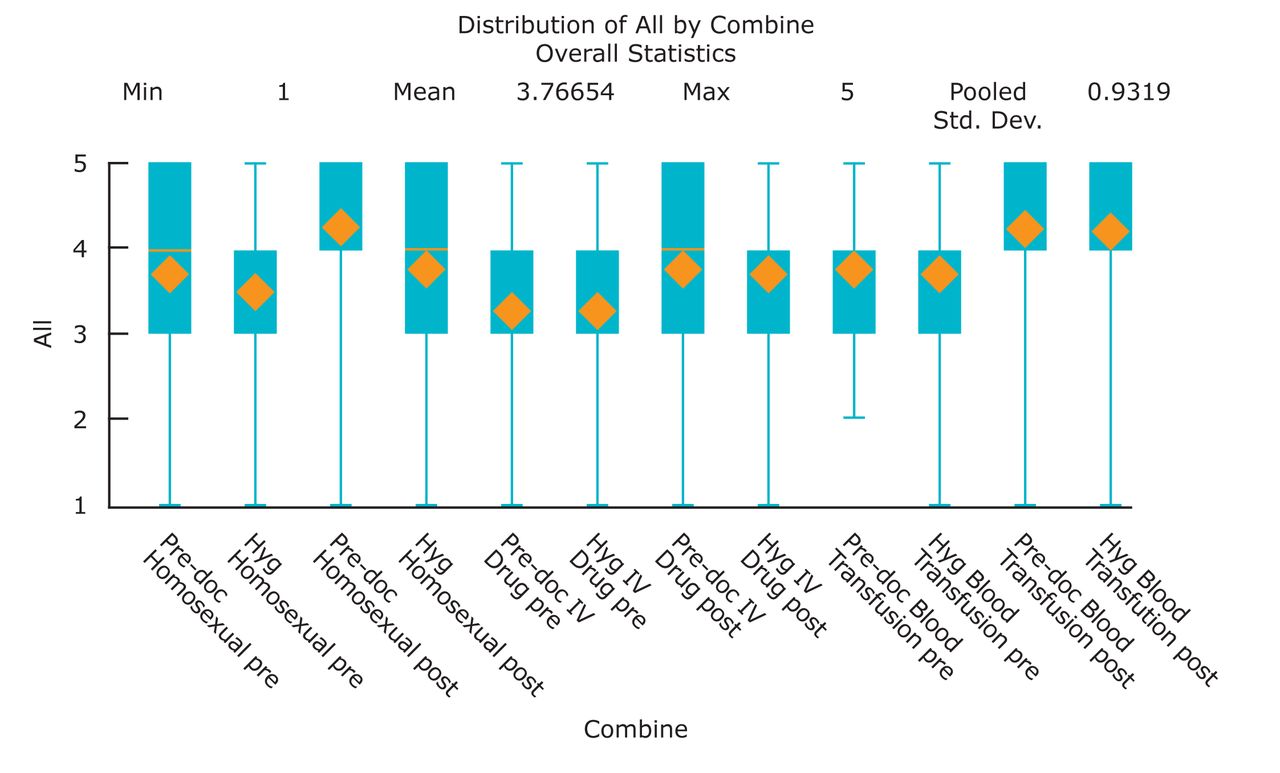
A graphic presentation of a comparison with quartiles (P25, median, P75) of the pre-session and post-session responses indicating students' level of comfort with treating certain patients is presented in Figure 1.
Discussion
The findings of this study indicate that as a result of the HIV and the dentist training program, there was a significant increase in the comfort level of students with regards to treating patients in the three categories of homosexual/bisexual individuals, intravenous drug users, and people who had blood transfusions. This indicates that the program was beneficial to both dental and dental hygienist students. Education and training can positively influence attitudes toward the provision of care to groups of individuals who have been, and often continue to be, stigmatized for their sexual orientation, lifestyle and/or medical condition.
To the best of the authors' knowledge, there has been no paper or publication thus far that has discussed the same variables examined in this paper with regards to pre-doctoral and dental hygiene students' comfort levels in treating high-risk patients. Some reports have discussed existing knowledge of bloodborne pathogens among dental students10 and have concluded that the need exists to improve education for dental students in U.S. dental schools in terms of enhancing their knowledge and willingness to perform procedures on patients with HIV.
The current study demonstrated that in general, dental hygiene students had stronger shifts towards enhanced comfort in treating patients with HIV in comparison with dental students. While this program altered the perception of both groups toward intravenous drug users, the dental hygiene students developed a more positive attitude towards treating such patients than the dental students. Dental hygiene students exhibited the same attitude pattern regarding patients with histories of blood transfusion. After attending the program, there was a positive statistical increase for both dental and dental hygiene students in terms of the intent to treat patients with histories of blood transfusion.
Studies in India concluded that providing awareness campaigns and re-orientation training for the medical intern students is essential in making them more comfortable in treating HIV patients.20-23 Other studies that found positive results through educational programs for dental hygiene and dental students similar to this study were conducted at Maulana Azad Medical College, New Delhi, where it showed a positive relation between the education given and a willingness to treat patients at risk.20
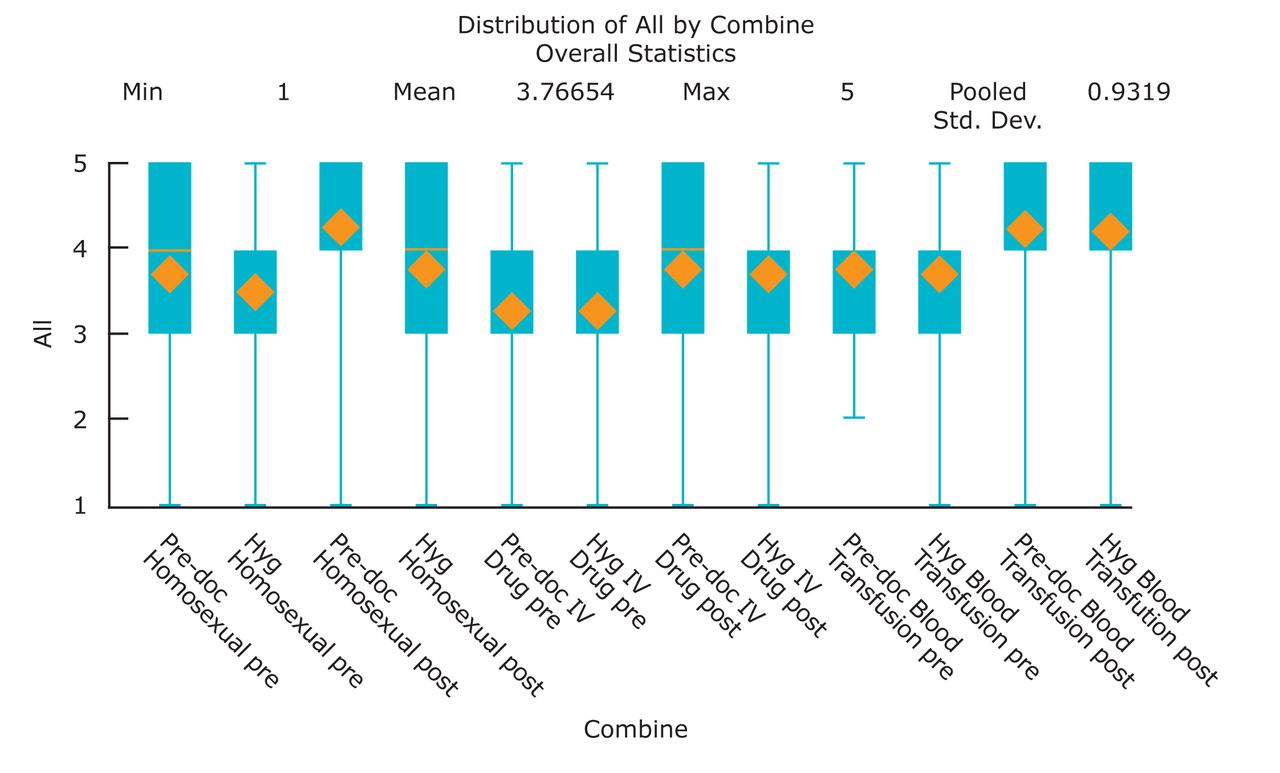
The Box Plot of Pre- and Post-Session Responses to the Intent to Treat Certain High-Risk Patients
However, a study from India that reported on the intent of students to treat patients with HIV and HBV found that even after attending an advanced education program, students still had negative attitudes towards treating patients with HIV/HBV,which could have been due to the need for a more sophisticated program, one that would facilitate a proper understanding of how to adapt to the practice experience of the students.21
There were a few limitations in our study; the variables homo/bisexual, IV user and history of blood transfusion are not commonly reported variables for the intent to treat by dental students and hygienists. These variables can carry a large array of infectious diseases in addition to HIV; hence a direct comparison between our study and previous publications cannot be obtained. The study consisted of a convenience sample of predoctoral and dental hygiene students that were not representative to the US population. An additional limitation would be changing the survey (even if only demographic data). The literature addresses the impact of reporting demographic data on respondents and it can be negative.23
Clinical Relevance
Dentists may be lacking in terms of willingness to treat and manage patients who are at risk of transmissible disease. For this reason, before they graduate, students need to be educated on how to handle such cases, so that they can serve as dental providers for all types of patients they might encounter in their careers. In addition, they need to learn about proper protection and how to reduce the risk of acquiring a disease during the course of treatment.
A focus on educating dental hygiene students is of equal importance in this regard, due to their higher chance of seeing more patients periodically compared to dentists. Hence, it is important to integrate additional training programs for both hygiene and dental students.
Details of the program contents in LLUSD were previously published in other articles, this program can aid any school in applying it's own methodology to its own curriculum and target population. We hope in the future to see more programs addressing this issue.
Conclusion
This study showed a significant improvement for both dental and dental hygiene students as a result of completing the LLUSD training program in terms of their perception and comfort level in treating patients who are homosexual/bisexual, intravenous drug users, or patients with histories of blood transfusion. Academic institutions need to ensure that dental and dental hygiene students are receiving the proper training to prepare them to provide optimal oral care to this patient population.
Footnotes
Zuhair S. Natto, BDS, MBA, MPH, DrPH, is currently a resident in the graduate program in Periodontics at Tufts University School of Dental Medicine, Boston, Massachusetts, and is also a Lecturer in Community Dentistry, School of Dentistry, King Abdulaziz University, Saudi Arabia. Majdi Aladmawy, BDS, AGD is currently a resident in the graduate program in Periodontics at Tufts University School of Dental Medicine, Boston, Massachusetts, and is also is employed as a restorative dentist at Prince Sultan Military Medical City, Saudi Arabia. Thomas Rogers, DDS, MPH, MA, is an Associate Professor at the Loma Linda University School of Dentistry.
This study supports the NDHRA priority area, Occupational Health and Safety: Investigate the impact of exposure to environmental stressors on the health of the dental hygienist.
Disclosure
This project was supported by a Community–Based Dental Partnership Grant issued under Part F of the Ryan White Program by the Federal Health Resources and Services Agency (HRSA) HIV/AIDS Bureau, Grant number H65HA00004.
- Copyright © 2015 The American Dental Hygienists’ Association





{kind=link}